
Abstract
Abstract
Lymphoscintigraphy following subcutaneous injection of a radiolabeled macromolecule, such as Tc-99m-nanocolloid, is used to investigate limb swelling, usually to confirm lymphedema. A well-known abnormal finding is dermal backflow, which occurs a result of diversion of lymph into skin lymphatic vessels. We describe a case in which this important sign was partially obscured by a stocking. The case also illustrates, first, the frequent though poorly recognized occurrence of lymphatic dysfunction in the clinically normal contralateral limb of a patient with unilateral swelling, and second, the principle underlying treatment with compression hosiery. Stockings should be removed before injection and all subsequent imaging.
Introduction
L
From the epifascial space in the lower limb, tracer accesses epifascial lymph vessels that drain to the groin via the main epifascial lymphatic trunk. There are two major categories of abnormality in lymphoscintigraphy: first, lymph delay, and second, lymph diversion, which may be into the deep (subfascial) system, with visualization of popliteal nodes, 2 or into superficial skin vessels giving the so-called appearance of ‘dermal backflow.’
We describe a case of a patient in whom dermal backflow was present. This important finding, however, was partially obscured by a tight stocking.
Clinical Details
A woman of 41 years presented with right leg swelling. The left leg was clinically normal. Before lymphoscintigraphy, the patient was investigated with Doppler ultrasound, which revealed that the deep venous system was patent and competent, with normal response to Valsalva, flow augmentation, and external compression. The long and short saphenous venous systems also appeared competent and patent.
Method
20 MBq of Tc-99m-labeled nanocolloid in 0.2 mL (GE, Amersham, UK) was injected subcutaneously into the dorsum of the first webspace of each foot using a 1 mL syringe and a 25-gauge needle. Penetration of the needle into a blood vessel was excluded by careful aspiration before injection. The injection, being subcutaneous, produced a bubble in the skin rather than a blister. No massage, warm compression, or leg elevation was performed after injection. Half-body anterior and posterior images from upper abdomen to toes were obtained with a large field-of-view gamma camera (GE Discovery NM630) commencing immediately and at 45 and 150 min after tracer injection. Each image took 10 min to acquire. The patient was allowed to take a short walk between the 45 and 150 min scans but not to undertake any strenuous exercise (like climbing flights of stairs). The patient removed her stockings for the injection and the first scan and then replaced them.
Ilio-inguinal nodal quantification
The percentages of the administered radioactivities present in regions of interest placed over the right and the left ilio-inguinal nodes were recorded in separately acquired, dedicated static images obtained at 45 and 150 min after injection. The geometric mean of counts simultaneously recorded from anterior and posterior projections were corrected for background and radionuclide decay and compared with a standard placed over the groin.
Criteria of abnormal lymphoscintigraphy
Abnormal scan findings can be divided into major and minor. 3 The major general criteria for lymphatic dysfunction after web space injection in the lower extremities are twofold: first, delay, identified as asymmetric or no visualization of ilio-inguinal lymph nodes, either at any time or before 150 min; and second, lymph diversion either into the skin, giving dermal back flow, or into the deep lymphatic system that accompanies the femoral venous system, leading to visualization of popliteal lymph nodes.
Results
Lymphoscintigraphy revealed abnormal findings in both legs. On the right, dermal back flow in the skin of the gaiter region was seen at 150 min. (Fig. 1). There was a well-defined horizontal lower border to this, suggesting the presence of a tight stocking that prevented entry of lymph into the small dermal lymphatics. The wearing of the stocking for the 150 min scan was confirmed. There was no evidence of diversion into the deep system.
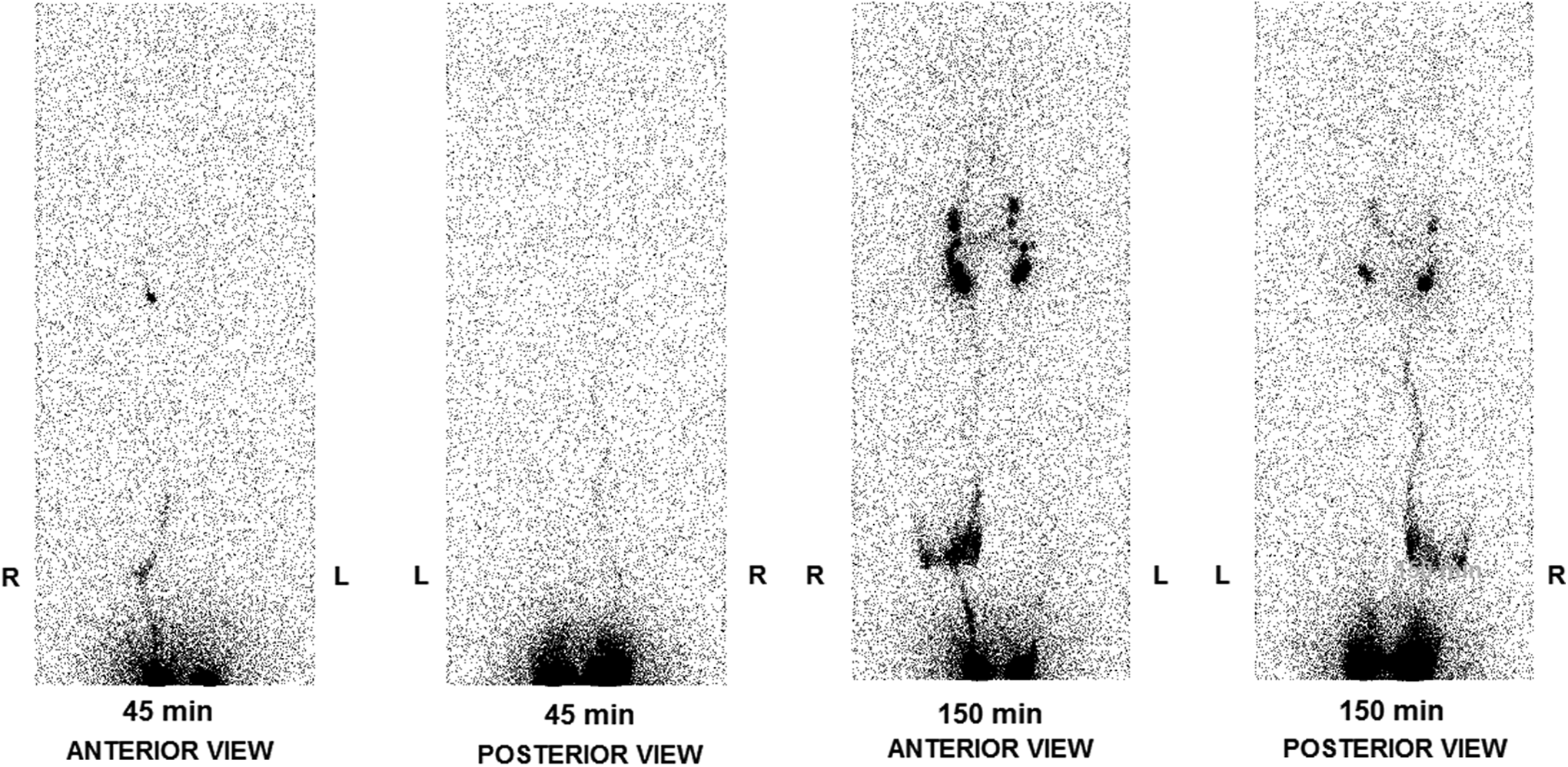
Anterior (left) and posterior (right) half-body lymphoscintigraphy performed 45 and 150 min after bilateral subcutaneous webspace injection of 20 MBq Tc-99m-nanocolloid in 0.2 mL. Note the well-defined horizontal margin limiting dermal backflow to the skin above a tight stocking in the gaiter region of the right leg. Note also, on the asymptomatic left side, the absence of any lymphatic structures at 45 min and absence of main epifascial trunk at any stage. Ilio-inguinal nodal activity is asymmetrical at 150 min, reduced on the left, best appreciated from the posterior projection. Note absence also of popliteal node activity, an abnormality resulting from lymph diversion into the deep system of lymphatics, which when present is best seen on the posterior projection and often associated with dermal backflow.
Lymph transport in the left leg was also abnormal with no visualization of the main epifascial trunk at any stage and ilio-inguinal lymph node activity not seen until 150 min (Fig. 1). No evidence of lymph diversion was noted in this limb. The ilio-inguinal nodal quantification was also below normal bilaterally with values at 45 min of 0.1% on the right and 0% on the left, and at 150 min of 4.5% on the right and 2.6% on the left. The lower limit of normal is not well-defined but is in the region of 10% at 150 min.
Discussion
In the extremities, the lymphatic system consists of a superficial (epifascial) system that collects lymph from the skin and subcutaneous tissue, and a deep system that drains subfascial structures such as muscle, bone, and deep blood vessels.
Lymphoscintigraphy of extremities is generally performed for investigation of lower limb swelling. Subcutaneous and intradermal injections into the web spaces deliver tracer to the epifascial lymphatic system, which normally remains separate from and does not communicate with the deep system. Tracer removal from the depot injection site is much faster following intradermal injection as a result of high pressure of the injection. This forces tracer initially into the dermal lymphatic vessels from which it rapidly enters collectors and the main epifascial trunk. 4 It is therefore more rational to test the lymphatic system by injecting subcutaneously, from where the tracer accesses small peripheral lymphatic vessels before entering the epifascial trunk.
Diversion of lymph through skin lymph vessels (dermal backflow) following subcutaneous injection is a major abnormality in lymphoscintigraphy. 1 In the current case, dermal backflow was obscured under the stocking as a result of compression of the epifascial system and resulting prevention of lymph from entering dermal lymphatics. With a longer stocking, the dermal backflow may have been completely obscured, which would have led to false negative findings. The take home message from this case report is that it must be ensured that patients remove stockings not only for the injection but also for all subsequent imaging.
The case also illustrates the effectiveness of treatment with compression hosiery. In principle, edema results when capillary fluid filtration exceeds lymph drainage capacity. The resulting swelling takes place in the epifascial space. Swelling in the subfascial space is prevented by the fascial envelope, so in the presence of subfascial lymphatic dysfunction, lymph is diverted to the subcutis, which swells as a result. 5 A massage technique known as manual lymph drainage stimulates the lymph vessels so that edematous fluid drains from the affected area. External compression therapy also promotes the movement of interstitial fluid into the lymph collectors and increases lymph transport capacity. 6 Significant edema reduction using this technique was shown by Boris et al, achieving rates of 79% volume reduction in the lower limbs. 7 Compression therapy combined with manual lymph drainage is also called complex physical decongestive therapy. This is supplemented by physical exercise. It is symptomatic rather than curative treatment.
The clinically normal contralateral limb was also abnormal on lymphoscintigraphy. Bilateral lymphatic dysfunction is typical of constitutional lymphatic weakness. Lymphatic dysfunction that is clinically evident unilaterally is often accompanied by contralateral dysfunction. Burnand et al. 8 found that a significant proportion of patients (32%) with unilateral clinical abnormalities had abnormal lymphoscintigraphy in the clinically normal limb (‘latent’ lymphatic dysfunction). Moreover, the ilio-inguinal nodal accumulation of the tracer in contralateral limbs of patients with unilateral lymphedema that were otherwise apparently normal on lymphoscintigraphy was on average two-thirds that of patients with no clinical or lymphoscintigraphic evidence of lymphatic dysfunction. Ilio-inguinal nodal quantification is essential in order to avoid missing latent dysfunction, as reduced quantification may be its only sign. The clinical significance lies in the detection of limbs at risk of lymphedema and especially cellulitis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.