
Abstract
Abstract
Background:
Combined physical therapy (CPT) is the treatment of choice for patients with lymphedema. Intensive stage CPT (I-CPT) results in a substantial reduction of the size of lymphedema, while the second stage CPT (M-CPT) maintains the achieved result for many years.
Aim:
The article analyses the outcome M-CPT for 5 years in patients with lymphedema after mastectomy.
Methods:
Forty patients had regularly been attending follow-up appointments every six months for five years (Group A). Out of the group of patients who had not been reporting for follow-up, twenty women accepted an invitation for assessment (Group B); none of them complied with the prescribed compression therapy. All patients were submitted to I-CPT and patients from group A completed M-CPT comprising compression garments and an individual program of physical exercises.
Results:
During five-year M-CPT, the difference in limb volumes (Vo), relative size of edema (Vor) reduction achieved after I-CPT was maintained in Group A, while in Group B a considerable increase of Vo by 14% was noted. Ultimately lymphedema in these patients was more pronounced than before their physical therapy had commenced. For 40 women using compression sleeves the mean Suitability Score System was 8.3 points on maximum 11-point scale, for 15 patients wearing additional compression gloves, the mean score was 4.3 points on maximum 5 points.
Conclusions:
The reduction of lymphedema achieved during I-CPT can be retained during M-CPT when the patient systematically attends follow-up examinations, applies compression therapy, and follows the therapy instructions. Non-compliance is followed by a worsening of lymphedema.
Introduction
L
CPT is carried out in two stages. The first, intensive stage (I-CPT), which usually spans about 1 or 2 weeks, permits a reduction in the size of lymphedema, while the purpose of the second stage, which comes directly after the first one and continues for several years, is to maintain the patient's improved condition (hence the name, maintenance-CPT, M-CPT). 5 The long-lasting stage of the therapy helps to maintain reduced volume of the limb, but the patients are required to be compliant and scrupulous in fulfilling the instructions. They must turn up for follow-up examinations at the appointed dates, which tends to be more difficult than the completion of the previous two-week therapy. 6 Regular monitoring for changes in the size of edema permits an early diagnosis of any deterioration in the patient's condition and the consequent intensification of treatment (for instance, by reintroducing I-CPT).
The aim of this article is to analyze the outcome M-CPT applied for 5 years in patients with lymphedema after unilateral mastectomy, taking into account the patients' adherence to the therapy instructions and the suitability of the prescribed compression garments.
Materials and Methods
Between 2006 and 2012, 157 women who had undergone mastectomy due to breast cancer and in whom recurrence was excluded were registered at the Lymphedema Clinic at St Lazarus Hospice in Cracow. Eighteen women did not consent to 10-day intensive CPT (encompassing two 5-day cycles carried out within 2 weeks). 139 patients completed I-CPT and were submitted to M-CPT. This comprised the wearing of fitting compression garments—namely compression sleeves and/or gloves, compression class 2—for use during the day, preventive and hygienic instructions, an individual program of physical exercises, and follow-up examinations carried out once every 6 months.
Five years after having completed I-CPT, forty patients (28.8%) continued to systematically turn up for follow-up appointments (one patient died). On average during the 5-year period, one patient in the group developed complications in the form of cellulitis, and a 10-day course of I-CPT had to be reintroduced in three cases because of clinical deterioration. Attempts to contact the 98 women who had not been reporting for follow-up examinations (despite having had appointments) were successful in 22 patients.
All patients who had completed preliminary I-CPT were prescribed compression garments (standard or made to measure) with a standardized compression level-class 2 (23–32 mmHg, medium) according to German regulations. If the size of lymphedema was abnormal, compression garments made to measure were prescribed. In Group A, 21 patients (with mild edema, ISL stage 1 or 2) were provided with circular-knit garments (standard sleeves), while nineteen patients (with advanced edema, ISL stage 2 or 3), with flat-knit garments (7 sleeves made to measure), and fifteen women were also given compression gloves (3 gloves made to measure). Three patients with lymphedema of the hand received lengthened compression sleeves that extended over the hand (standard garments). The compression garments for all the patients came from the same manufacturer and were given out along with standard educational handouts addressing wear time, washing intervals, and garment replacement intervals. None of the patients in Group B complied with the prescribed compression therapy.
The patients in Group A regularly attended follow-up examinations (once every 6 months on average) and applied the prescribed compression garments during the day, taking proper care of them and removing them before a night's rest. 36 patients systematically replaced their prescribed garments with new ones (once a year on average), while four women were not as systematic. Fifteen patients applied compression for more than 12 hours per day, twenty patients, for anything between 6 and 12 hours per day, and five patients, for less than 6 hours per day. Thirty-seven women carried on with the prescribed physical activity during compression therapy on a daily basis (three patients were doing exercises irregularly). Thirty-seven patients required additional bandaging for the night; three of them applied bandaging every night. Thirty-two patients declared that their compression garments were easy to put on, 33 patients associated the wearing of compression garments with greater comfort, and all patients experienced a subjective sensation of reduced swelling when they were wearing compression garments.
Circumferential upper limbs measurements were taken every 4 cm from the wrist, measurements of the hand were not included. Calculation of limb segment volumes was undertaken using a simplified frustum formula. The lymphedema volume (mL) was calculated by the difference between the affected limb and normal limb. The percent relative lymphedema volume was determined by subtracting the volume of the normal limb from the affected one and dividing it by the normal one.
The fitting of sleeves and gloves was assessed using the Suitability Score System (SSS). 7 The aspects taken into account in the assessment of a sleeve included knitting technique, application time, periodic replacement, garment care, problems with putting on the sleeve, subjective effectiveness and comfort of the sleeve, and additional night bandaging—the best-fitted sleeves scored ten points. The assessment of a glove comprised five different aspects, including garment size, pressure, and the indications of discomfort related with length of the fingers, cutting in the wrist, finger cyanosis, and ampleness of the glove.
Given that the obtained results did not fall within the normal distribution, the statistical significance of differences within the groups was assessed using the Wilcoxon signed-rank test, and between the groups, using the Wilcoxon rank-sum test, with the null hypothesis rejection at p<0.05.
The research reported in the article was undertaken in compliance with the Helsinki Declaration. The protocol for the research project has been approved by the local Ethics Committee.
Results
The baseline characteristics of the investigated patients are summarized in Table 1. Group A consisted of 40 patients who regularly attended follow-up appointments for 5 years from the completion of I-CPT, and group B of twenty patients who did not attend the appointments and were assessed after the 5-year period. Arm volumes were significantly larger in Group B (as compared to Group A), both for the affected and for the contalateral extremity.
p<0.001.
BMI, Body mass index; ISL, International Society of Lymphology.
Group A consisted of constitutionally slimmer women (lower mean Vn) but the mean edema volume within two Groups were similar both in the absolute (difference between Va and Vn, Vo) and relative values (Vo divided by Vn). Pitting edema of the forearm and arm, classified as ISL stage 2 lymphedema, was prevalent in either of the groups before the treatment (Table 1).
A significant swelling reduction was achieved in Groups A and B after I-CPT (Vo reduction by 278.2 mL [13.1%] and 283.7 mL [11.1%], respectively)—the absolute (Vo) and relative (Vor) sizes of edema did not differ between the two groups after the intensive stage of treatment. During 5-year M-CPT, the Vo and Vor reduction achieved after I-CPT was maintained in Group A, while the patients in Group B were diagnosed with a considerable increase of Vo by an average of 399.2 mL (14%); in consequence, lymphedema in these patients was bigger than before their physical therapy had commenced (Table 2).

p<0.001.
I-CPT, intensive phase of Combined Physical Therapy.
I-CPT in Group A reduced affected limb volume (Va) by 9% in average, which is fairly maintained by M-CPT in the following 5 years; however. the values after 5 years are slightly but significantly higher at the and compared to after I-CPT (p<0.05).
I-CPT in Group B reduced affected limb volume by 10% in average, but during the next 5 years without therapy, affected limb volume (Va) increased by 7% in comparison to the initial status. There is no significant change of volume between the initial status and the volume after 5 years (Fig. 1).
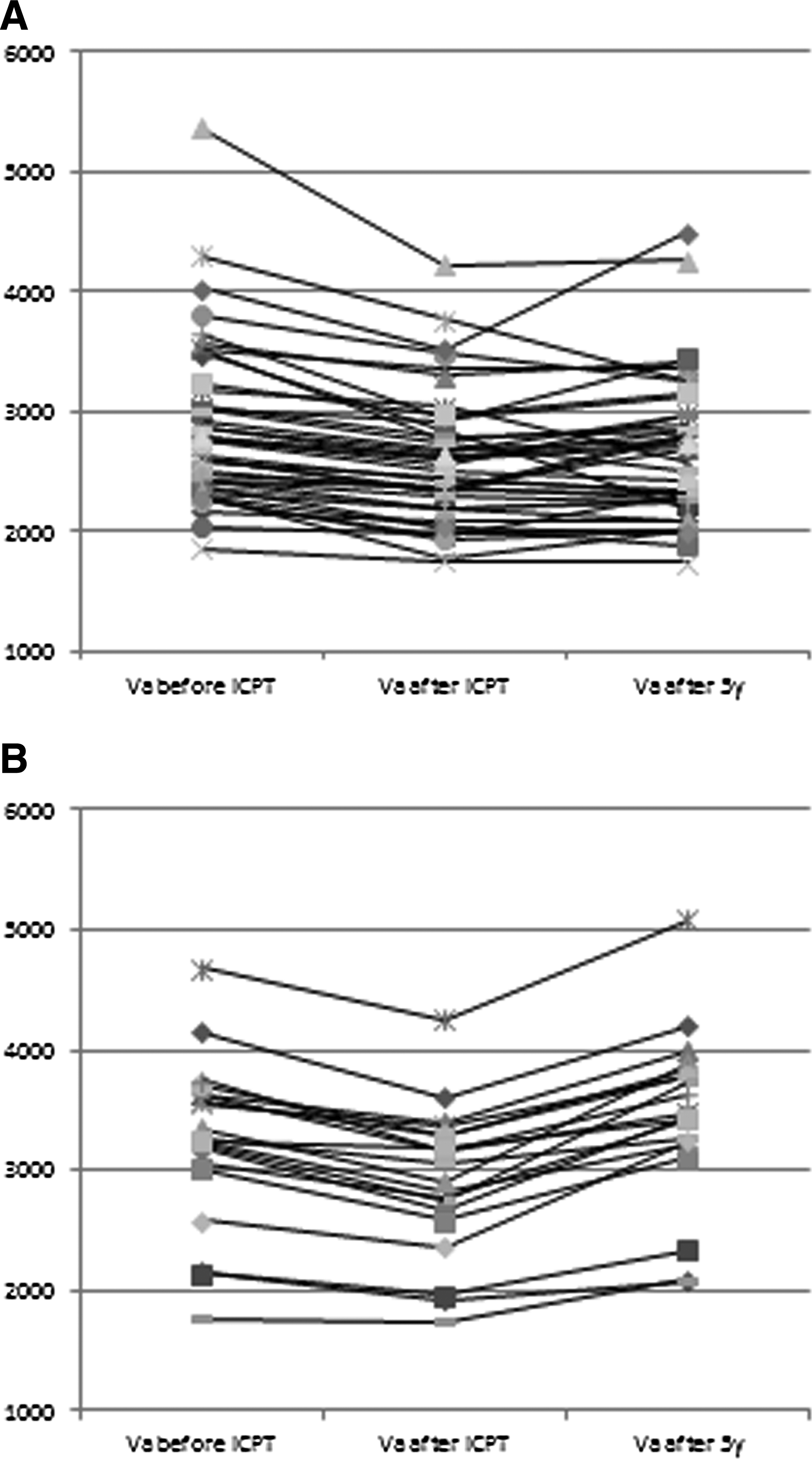
Affected limb volume (Va, mL) before and after therapy in Group A and B.
Compression garment suitability assessment
Out of the 40 patients using compression sleeves, 25 women scored eight or nine points on the eleven-point SSS scale (the mean was 8.3 in the range from five to ten points (Fig. 2).
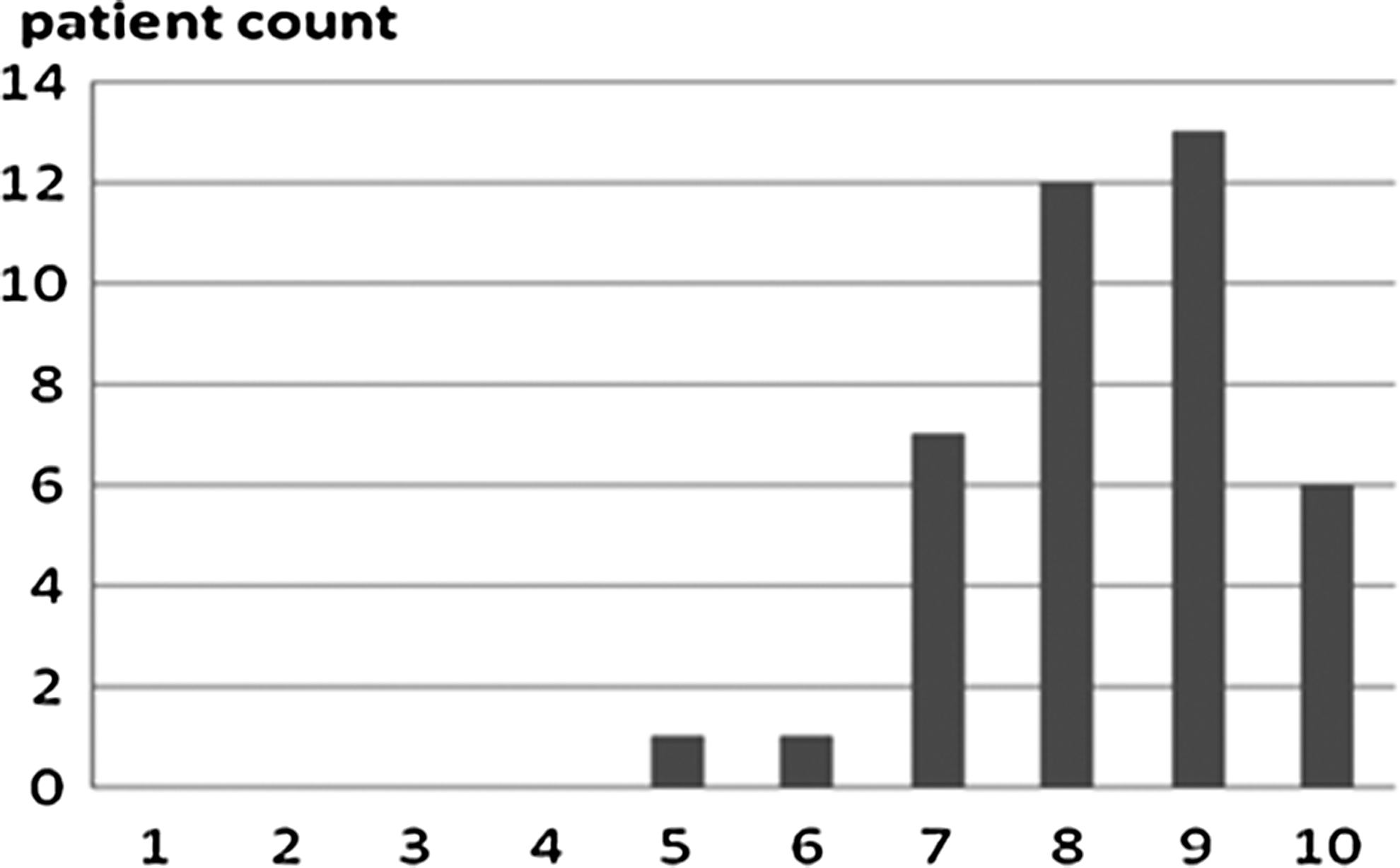
Sleeve suitability assessment on a suitability score scale from 1 to 10 in 40 patients from Group A.
The most frequent complaints about the sleeves were concerned with skin reddening in the elbow pit (reported by twelve patients), edema of the hand (twelve patients), excess pressure in the region of the armpit (five patients), and curling of the material (four patients). Out of the fifteen patients wearing additionally compression gloves, twelve women scored four or five points on the six-point SSS scale (the mean was 4.3 in the range from two to five points (Fig. 3). The most frequent complaints about the gloves were concerned with cyanosis of the fingers (reported by three patients) and excess pressure in the region of the wrist (four patients).

Glove suitability assessment on a suitability score scale from 1 to 5 in 15 patients from Group A.
A link was also established between a short time of wearing compression sleeves and a lack of any sense of comfort while using compression garments (seven patients had never experienced such comfort). In two cases the wearing time had been less than 6 hours.
Discussion
The effectiveness of physical therapy is determined by a number of factors whose actual impact depends on the therapist as well as the patient and spreads over a period of many years. On the stage of qualifying the patients for I-CPT, 11.5% of the women in the analyzed group (namely 18 out of 157) refused to submit to the suggested treatment. The commonest reasons for the refusal were concerned with a large distance between the therapy facility and the patient's place of residence (impeded access), and a substantial cost of treatment (given that not all compression garments are refundable in Poland). The women who submitted to I-CPT were very cooperative; all of them completed the intensive therapy as planned. The daily appointments with a therapist were also spent on encouraging the patients to follow the prescribed treatment in the future, all the more so because the swelling and its concomitant symptoms began to subside noticeably within a few days of the intensive therapy. A marked and rapid improvement was achieved using the full scope of I-CDT, although similar results can also be obtained without manual lymphatic drainage, applying only compression with bandages and physical exercises. 8
It is a more credible indicator of the effective treatment of lymphedema—which is a chronic condition—when patient's health improves in the long term, meaning that the outcome of I-CPT has been maintained. Judging from this analysis, it was possible to maintain a long-lasting therapeutic effect in the patients who were systematically following the instructions; however, the group of such systematic patients was decreasing over the period when the women were kept under observation and treated as outpatients, and after 5 years, only one in three patients adhered to the prescribed therapy regime (28.8% of the group of 139 women). Patients lacked the motivation to assume partial responsibility for the treatment even though they had experienced a significant reduction of swelling during the first stage of therapy. Other authors point out that the reduction of lymphedema achieved during the intensive stage can be retained during the maintenance stage when the patient systematically attends follow-up examinations, applies compression therapy, and follows the therapy instructions. 9 Otherwise, especially when compression therapy is neglected, the achieved improvement soon goes to waste. Also, a long-lasting effect of I-CPT is possibly maintained thanks to not only wearing and regularly replacing compression garments, which should come from the same manufacturer, 10 but also additionally bandaging the limb for the night, as the majority of patients in Group A (namely 37) were doing. 11 Additional benefits of night-time compression have been observed as well. 12
In retrospect, the patients who were regularly turning up for follow-up examinations (Group A) tolerated the prescribed compression by means of sleeves and gloves, and their high scores in the suitability assessment according to the SSS testified to that trend. Other authors made similar observations. The majority of the patients undergoing treatment in the analyzed period (71.2%) did not accept compression therapy as a long-lasting procedure. By analogy, therapists dealing with chronic venous insufficiency observed that about 42% of their patients had not been attending follow-up examinations. 13
Conclusions
The reduction of lymphedema achieved during the intensive stage can be retained during the maintenance stage when the patient systematically attends follow-up examinations, applies compression therapy, and follows the therapy instructions.
Acknowledgments
We would like to thank Professor Hugo Partsch for help and comments during the writing of this article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.