
Abstract
Abstract
Background:
Biomechanical skin changes in breast cancer-related lymphedema (BRCL) have barely been described and objectively tested. This study aims to compare the skin of upper limb lymphedema with skin of the healthy contralateral arm, in order to demonstrate changes of elasticity, viscoelasticity, and level of hydration of the skin in BCRL. The secondary aim is to investigate the correlation between biomechanical skin changes and measurements that are currently used in clinical practice, such as volume measurement and lymph-ICF score.
Methods and Results:
Eighteen patients with BCRL and 18 healthy individuals were included in the study. A Cutometer® was used for measurements for skin elasticity and viscoelasticity on both arms of each subject. A Corneometer® was used for measurements of skin hydration. Measurements of both test groups were compared. In BCRL patients, there was a significant difference (p=<0.028) between the elasticity of the skin of the lymphedema arm compared to the healthy contralateral arm. There were no significant differences for level of skin hydration or viscoelasticity in lymphedema patients between the measurements on the skin of the lymphedematous and healthy arm. In healthy individuals, there were no significant differences for all measurements between skin of both arms. Spearman's correlation was significant (p=<0.01) for difference in volume and difference in elasticity in BCRL patients.
Conclusion:
This study shows an impaired elasticity for the skin of the lower arm in patients with lymphedema compared to the contralateral healthy arm. Promising evidence is suggested for the use of the Cutometer device in the diagnostic evaluation of BCRL.
Introduction
O
Activation of lymphocytes, leukocytes, and release of cytokines induce connective tissue synthesis in fibroblasts. The excessive deposition of extracellular matrix, especially collagens, is the complex tissue response that is called fibrosis. 1 Ultrastructural research has shown that this process is accompanied by the degeneration of smooth muscle cells in the lymphedematous tissue. 2 The contraction of these smooth muscle cells, together with the compression of skeletal muscles, determine the interstitial pressure that stimulates lymphatic drainage. The above-described pathological changes of the lymphedematous tissue can be regarded as a key step for the progressing pathological status of lymphedema.3,4
Tissue resistance in post-surgical lymphedema has previously been measured and evaluated with the use of tonometry. 5 Indentation measurement on lymphedema patients has shown increased tissue resistance in lymphedematous skin.6,7 Both the pathogenesis of BCRL and the previous findings of increased tissue indentation in lymphedatous tissue implicate a role of biomechanical skin changes within development of BCRL.
The Cutometer device is seen as an attractive and suitable option for testing and monitoring changes in biomechanical properties of the skin.8,9 This device has been used in previous research for the evaluation of skin properties in facial wrinkles, wounds and scar healing.10–12 Furthermore, it has been used for measuring elasticity of the skin after radiotherapy. 13
Besides the biomechanical skin properties in the evaluation of BCRL, fluid accumulation is an initial component in edematous and lymphedematous conditions. Tissue fluid water and proteins accumulate in the interstitial space.14,15 This makes it both of fundamental and clinical interest to know what relationship exists between tissue water and tissue resistance.
Local tissue water in lymphedema has already been quantified using the tissue's dielectric constant (TDC), showing significantly greater values in lymphedematous legs compared to healthy legs. 7 These outcomes gained our interest for determining skin hydration in lymphedematous conditions. In the past, measurements of skin hydration have particularly been used in dermatologic testing of products and for the evaluation of skin development.16–18 Measurements are mostly performed by use of a Corneometer, which is a validated tool for measuring hydration of the stratum corneum of the skin. 20
The primary aim of this study is to compare the lymphedematous skin to that of the healthy contralateral arm in breast cancer survivors, in order to demonstrate the biomechanical changes (elasticity, viscoelasticity) and level of hydration of the skin. The secondary aim is to correlate biomechanical skin changes with current clinical assessment measurements of lymphedema, such as objective volume measurement as well as subjective functional impairments measured with the Lymph-ICF score.
Materials and Methods
Subjects
A total of 34 women with BCRL were asked to participate in the study, of which 24 were willing to participate. All subjects were over 18 years and were treated for unilateral early stage breast cancer in Maastricht University Medical Centre+ (MUMC+) between May 14, 2004 and December 21, 2010. During routine follow-up visit after primary breast cancer surgery, upper limb volume of the affected side was measured with the water-displacement method and compared to that of the healthy contralateral arm.
Patients were enrolled in the study if they had more than 200 mL volume difference and had subjective complaints or if they were currently being treated by a lymphedema therapist. Patients were excluded from participation if they had recurrent breast cancer, bilateral breast cancer, distant breast cancer metastases, or if they had a medical history of cancer other than breast cancer. A total of 22 patients met the inclusion criteria. Subjects were instructed not to wear elastic arm garments on the test day so that volume measurements were not influenced. Written consent was obtained from each subject prior to inclusion of this study.
Eighteen healthy participants, all women, without BCRL or open lesions on their upper extremity were asked to participate.
Three subjects with unilateral BCRL wore an elastic arm garment on the test day (against the given instructions). One patient exceeded the maximum arm volume measurable by the water displacement method. These four BCRL patients were excluded from the study before calculations were made (Fig. 1).
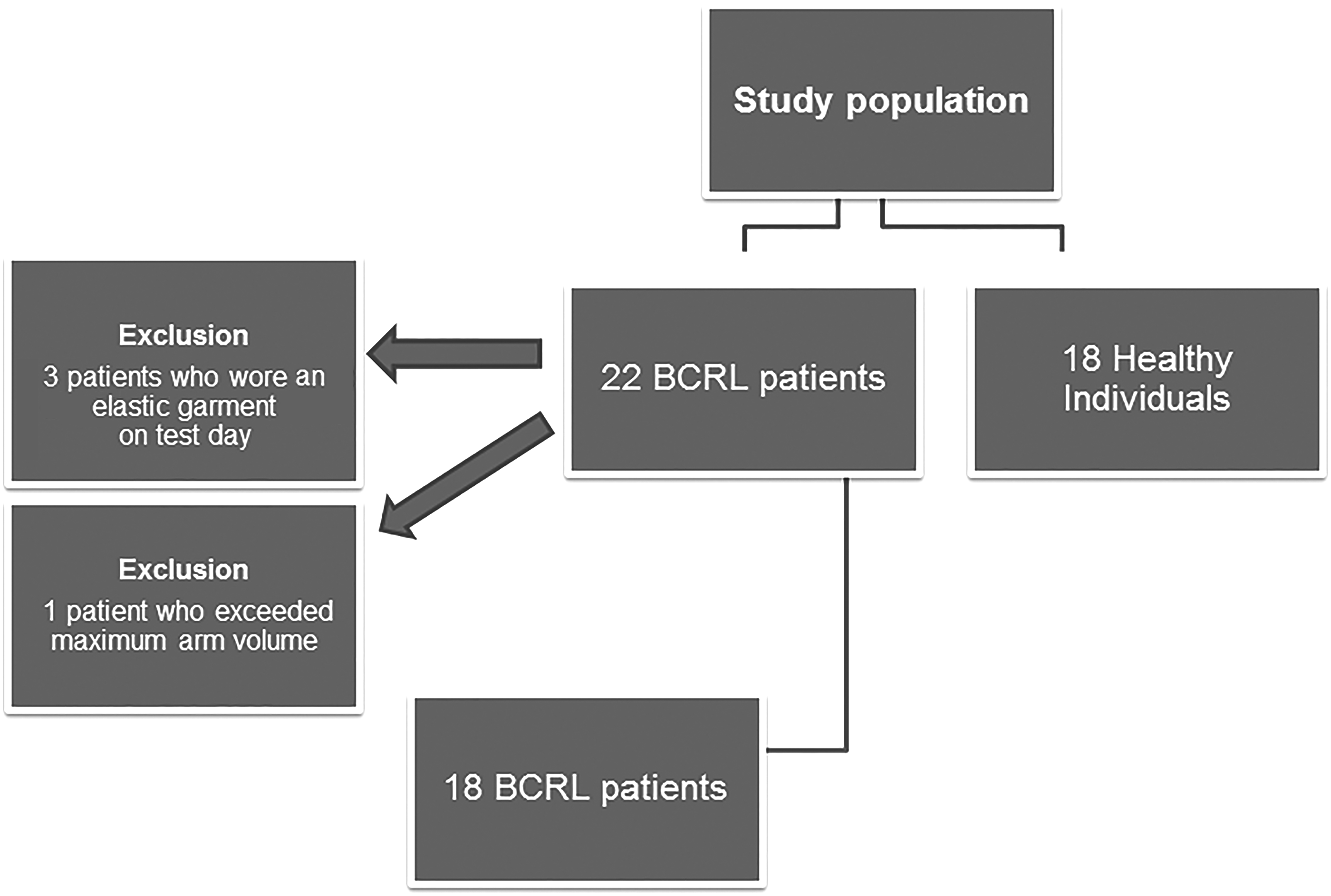
Flow chart for study population.
Ultimately 36 subjects completed the study, 18 subjects with unilateral BCRL and 18 healthy individuals. Baseline characteristics of all subjects were collected before testing.
Study design
All subjects were invited for a single consultation in the outpatient clinic of MUMC+. Measurements were done in the same room with specified conditions; a temperature of 20°–22°C and 40%–60% humidity as instructed in the measuring principles of the Cutometer® MPA 580 (Courage and Khazaka, Köln, Germany). Patients were seated with their arm on the surface of the table with their hand and fingers relaxed during Cutometer measurements. The angle of the elbow was approximately 120°, the angle between the upper arm and the supporting surface was approximately 40°, and the angle between the upper arm and the shoulder was approximately 90°. Measurements for elasticity, viscoelasticity, and hydration were performed on each subject on both arms.
Elasticity measurements were taken of the skin of both lower arms, at the volar midpoint between the tip of the ulnar styloid process and medial epicondyle of the humerus (F-MP). This is one of the predetermined sites of the lower arm where extra lymphatic fluid of the upper limb can accumulate. 19 The volar site of the arm was taken so that measurements were not influenced by body hair on the dorsal site of the arm. Cutometer measurements were repeated after 10 minutes, as advised by the device manufacturer. The suction and release time of the Cutometer could cause the skin to be strained and might distort the results of the next measurement. The average of both measurements was taken and used for analysis.
All study procedures were in accordance with the ethical standards of the Medical Ethical Committee Maastricht and with the Helsinki Declaration of 1975, as revised in 2008.
Elasticity and viscoelasticity of the skin
Vertical extensibility of the skin was measured using a Cutometer MPA 580 system with a Cutometer Q probe: a noninvasive suction device that measures the vertical deformation of the skin surface. A constant negative pressure of 450 mbar during 6 sec was applied, to draw the skin up into the circular aperture (6 mm diameter) of the probe, followed by normalization of the pressure and returning of the skin in original shape. 20
The Cutometer device generates a graph showing skin extensibility (Ue), delayed distension (Uv), final deformation (Uf), immediate retraction (Ur), and final retraction (Ua) (Fig. 2). The Cutometer software MPA 580 was used to automatically generate R parameters (R0 to R9). These parameters are relative parameters that are thought to be independent on skin thickness, which varies in age, sex and anatomical region. 9 Skin elasticity is reflected by R2, R5, and R7. 21 These values were generated as follows (Fig. 2): R2 (Ua/Uf) (gross elasticity), R5 (Ur/Ue) (net elasticity), and R7 (Ur/Uf) (biological elasticity). Value R6 (Uv/Ue) represents the viscoelasticity ratio.

Graph for skin deformation generated by Cutometer device; in which the following absolute parameters are represented: Ue (skin extensibility), Uv (delayed distension), Uf (final deformation, Ur (immediate retraction), Ua (final retraction).
Hydration of the skin
An additional Corneometer CM 825 probe was used to assess the level of hydration of the stratum corneum in the lymphedema and healthy contralateral arm. The probe contains a grid of electrodes, which are used for measuring the capacitance of the electrodes and epidermal skin to calculate total skin capacitance. The values of capacitance of the skin are converted in the instrument in arbitrary units of skin hydration ranging from 0 to 120. 16 Calibration was performed using a cellulose filer paper saturated with a 15% NaCl aqueous solution, giving a maximal hydration value of 120. To increase reliability, measurements at F-MP on both arms were taken three times from which the average was taken.
Determining severity of lymphedema
The degree of lymphedema is determined by different measurements and values, including volume difference of the upper limb and experienced disabilities as a result of the lymphedematous limb.22,23 All lymphedema patients in the study underwent an objective measurement of volume of both arms, and had to fill out the Lymphedema Functioning, Disability and Health” (“Lymph-ICF”) questionnaire for evaluation of the current functional impairments they were experiencing from the lymphedema.
The Lymph-ICF is a validated questionnaire that assesses the impairments in function, activity limitations, and participation restrictions in patients with upper limb lymphedema, based on 29 questions corresponding with a score between 0–100. A higher score indicates more problems with functioning related to upper limb lymphedema. 24
Inter-limb volume difference was measured using the water displacement method, the golden standard for measuring arm volume. 23 A Volumeter (Varitex, Haarlem, The Netherlands) was filled with tap water with a temperature of 25°C and 32°C. Water temperatures across the range of 20–32°C were not found to affect the volume measured.25,26 A circumference line was drawn at 80% of the arm length, measured from the tip of the third digit to the tip of the acromion. Subjects were instructed to lower the arm into the Volumeter until the water reached the circumference line. The Volumeter weighed the overflowing water with an integrated calibrated scale with an accuracy of 1 cc.
All water displacement measurements were done after hydration measurements with the Corneometer CM 825 probe, so that the hydration state of the stratum corneum of the skin could not be influenced by the water exposure of the arm in the Volumeter.
Data analysis
Patients and clinical characteristics were described using descriptive statistics. Reliability analysis was used to calculate intraclass correlation coefficient (ICC) to determine the intra-rater reliability of the Cutometer measurements in the lymphedematous arm. The Intraclass Correlation Coefficient (ICC) was used to determine the intra-rater reliability of all elasticity measurements in healthy and lymphedema skin. Intra-rater reliability was determined from two repeated measurements with the Cutometer done by the same investigator. To assess differences between biomechanical skin properties in both arms, a Paired Samples t-test was used. A p value of <0.05 was considered statistically significant. The measurement parameters (elasticity or hydration) that were significantly different in the BCRL arm and the healthy contralateral arm, were correlated to clinical assessment points (difference in limb volume and lymph-ICF score). These correlations were calculated with Spearman's correlation coefficient. Data were analyzed using statistical software (SPSS 20.0 Inc Chicago, Ill).
Results
Participants
All 36 subjects were able to complete the study. BCRL patients had a median age of 63 years [SD 9.2]. Ten patients had left-sided lymphedema, 8 patients had right-sided lymphedema. Healthy individuals had a mean age 23 [SD 12.4] of and a mean BMI of 22 [2.7]. All 18 individuals were female. Patient characteristics of both groups are described in Table 1.
Reliability of measurements
Intraclass correlation coefficients (ICC) for all elasticity parameters were high, ranging from 0.707 (R7) to 0.882 (R2) for single measures. ICC for viscoelasticity (R6) was 0.753 (Table 2).
Interlimb difference
Elasticity and viscoelasticity
Patients with BCRL had an impaired elasticity of the skin in the lower lymphedematous arm, compared to their healthy contralateral arm. All values for elasticity showed a significant difference (R2: p=0.028; R5: p=0.019; R7: p=0. 013). The mean elasticity difference between both arms ranged from 0.127 (R5) to 0.08 (R7). There was no significant difference between viscoelasticity of the lymphedematous arm and contralateral healthy arm (R6: p=0.409).
Healthy individuals showed no difference for values of elasticity and viscoelasticity between the skin of both lower arms (R2: p=0.782; R5: p=0.339; R7: p=0.147 and R6: p=0.632) (Table 3).
Paired Samples t-Test. *significance level p<0,05
Hydration
The hydration of the skin between both arms was not significantly different in BCRL patients (p=0.218). In healthy individuals, the difference was also not significant (p=0.488) (Table 3).
Volume
Mean difference for volume between both arms in BCRL patients was 385 cc [SD 369].
Lymph-ICF score
Mean Lymph-ICF score for BCRL patients was 36 [SD 19.5].
Correlations (between biomechanical skin changes and volume difference or Lymph ICF score)
Spearman correlations for inter-limb differences in elasticity (R2,R5, and R7) and inter-limb volume difference were significant for R2: r=0.591 (p=0.010); R5: r=0.618 (p=0.006), and R7: r=0.649 (p=0.004) (Figs. 3, 4, and 5). Correlation coefficients for elasticity and Lymph-ICF score were low and not significant, ranging from r=0.031 (R7) to r=0.088 (R2).
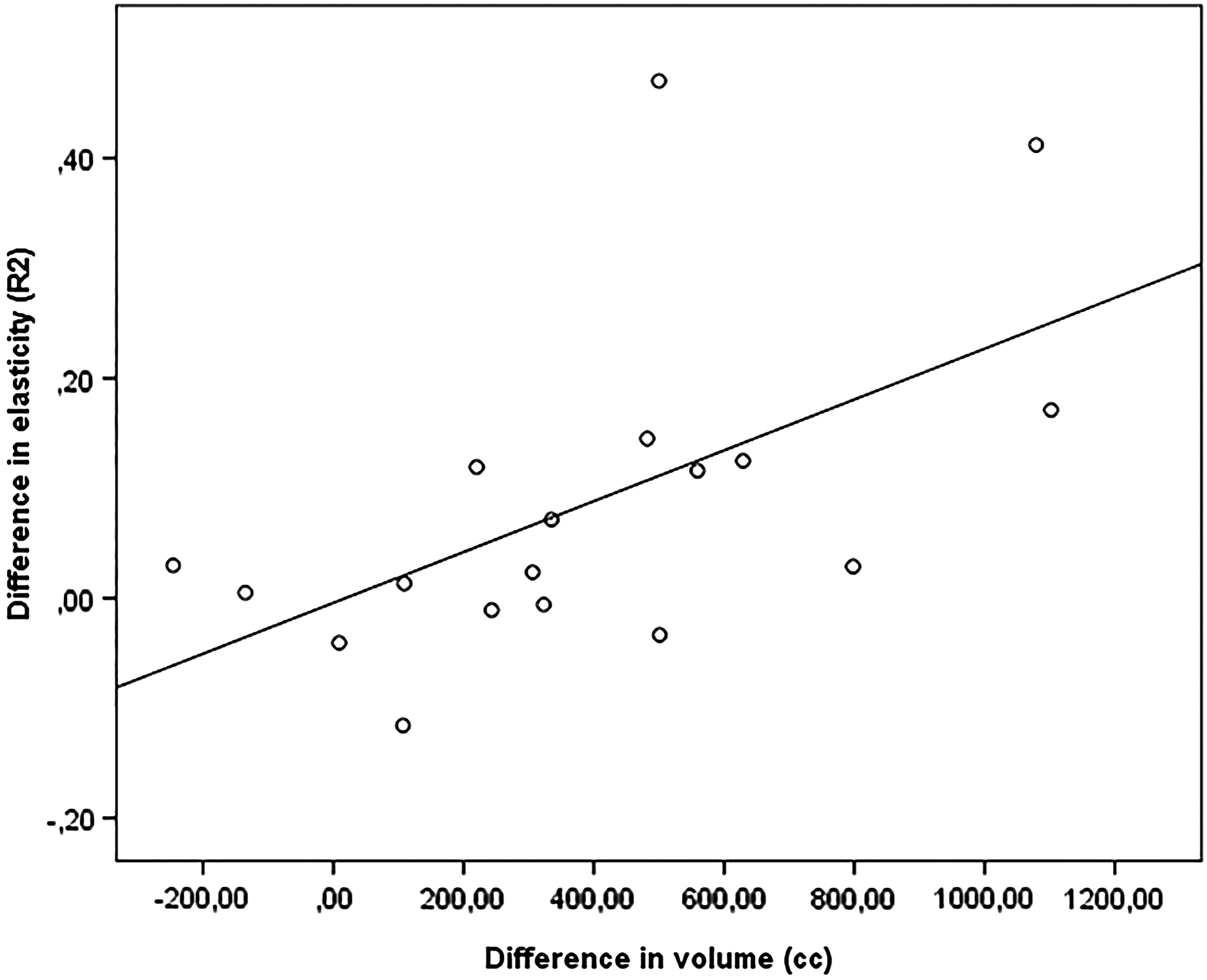
Correlation between elasticity difference (R2) and volume difference (cc) between both arms; r=0,59 (p=0,010).

Correlation between elasticity difference (R5) and volume difference (cc) between both arms; r=0,62 ( p=0,006).
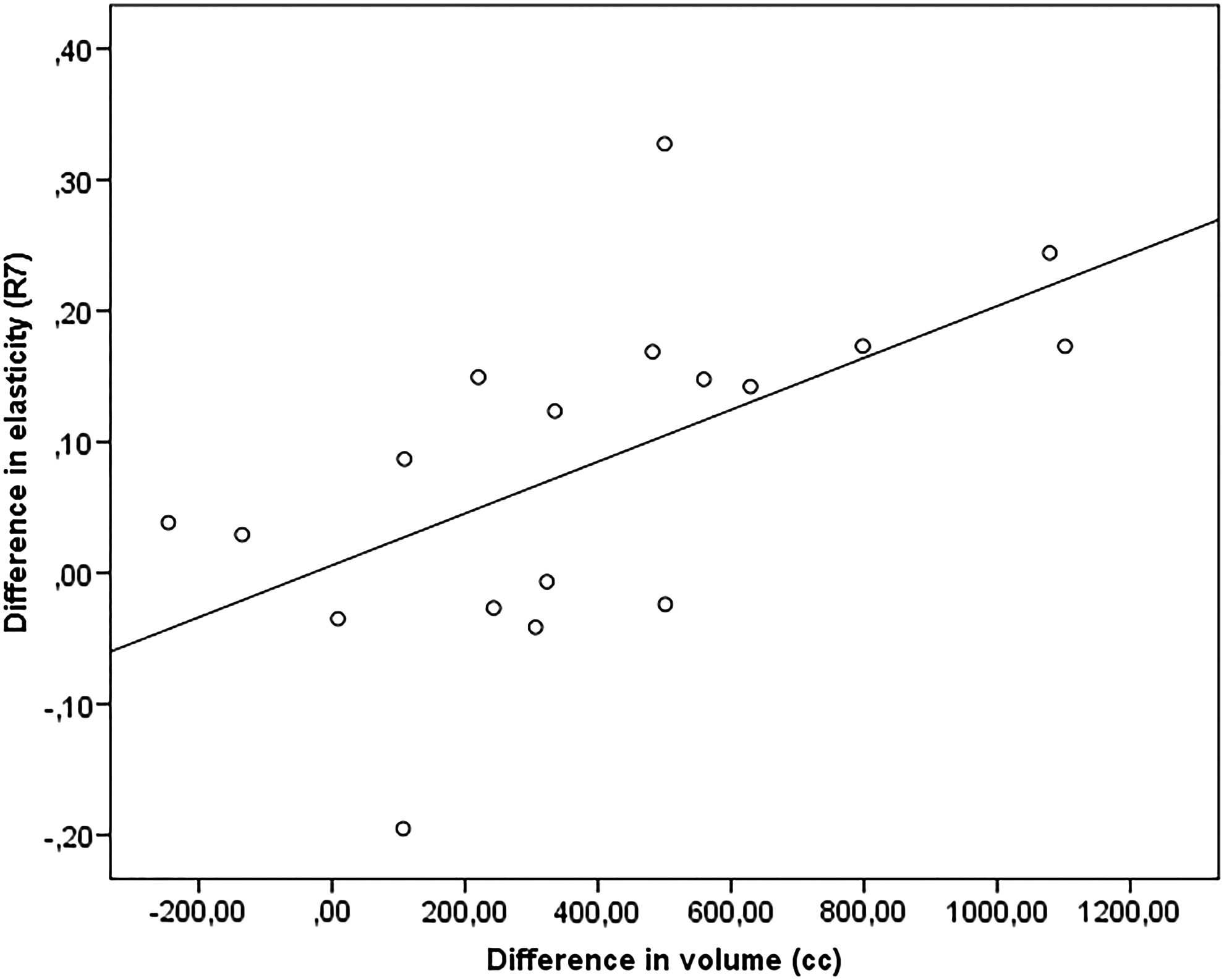
Correlation between elasticity difference (R7) and volume difference (cc) between both arms; r=0,65 (p=0,004).
Discussion
The results of this study show a significantly lower elasticity of the skin in upper limb lymphedema. This finding is supported by the theory that there is an increase in volume of the subcutaneous tissue that affects the skin by increasing its tension at rest. 22 The proportional changes within the tissue result in modification of the intermolecular bridging and thickening of the collagen bundle. 27
The Cutometer Device was a reliable method for the evaluation of skin elasticity in lymphedematous skin using the suction method. Values for extensibility and elasticity were reliable with a reproducibility ranging from 0.707 to 0.882. Other studies using a Cutometer for measuring skin properties found small coefficients of variation between measurements ranging from 0.7%–6.2%.8,28 Inter-relation parameters for elasticity measurements show high correlations. (R: 0.7– >0.9). 29
The advantage of measurements with the Cutometer is that the outcome for elasticity is corrected for the depth of deformation applied with the instrument. The small size of the measuring probe makes it very applicable in clinical practice. In addition, the minimal measuring diameter decreases the chance of bias due to topographical irregularities.
Tools that have previously been used for the measurement of biomechanical properties of the skin are a tonometer or a caliper. A tonometer can be applied to the skin to measure the depth of the mass that is descended. Results of measuring with the tonometer highly relied on the correct positioning and amount of pressure applied when placing the tool on the skin.5,30 A caliper, which is used to measure skin creases of the arm, appeared to be a reliable measuring method, but edema of the deeper tissues is not taken into account. 31 Tissue indentation measurements for the assessment of lymphedema have previously been developed to evaluate tissue resistance.
Tissue resistance is not only dependent on the biomechanical properties of the skin, but also influenced by the underlying accumulated interstitial water. 7 The amount of interstitial water can be easily influenced by therapy such as manual lymphatic drainage. Indentation measuring is therefore not suitable for quantifying the biomechanical properties of the skin alone. Measurements with the Cutometer are less dependent on the amount of interstitial water, as it measures only the skin extensibility with use of the suction method. This can make the measurement very suitable for diagnostic of follow-up measurement in clinical practice to investigate the pathological changes of the skin in BCRL.
There are a few other studies that use a Cutometer for measuring skin extensibility and elasticity in lymphedematous skin. Auriol et al. showed a 20% reduction of skin extensibility (Ue) and elasticity (R5) in the lymphedema lower limb in comparison to its healthy contralateral limb. 31 These results are consistent with our findings of an impaired elasticity in the skin of upper limb lymphedema. In addition, the current study shows a significant correlation between elasticity and volume difference of both arms. This suggests a clinical relevance for the elasticity parameter. In other words: a continued decrement in the elasticity parameters may be an indication for further progression of lymphedema.
Lymphedema evaluation in clinical practice tends to focus on volume change. 32 Although volume is important and is the most objective current clinical measure, using only volume may overlook important tissue texture changes, as well as latent stage lymphedema disease. 33 Hacard et al. studied patients undergoing therapy for lymphedema, and used values of elasticity measured with a Cutometer to evaluate the changes in skin properties before and after therapy. 21 Correlations were calculated for elasticity parameters and decrease of volume after therapy. A correlation was not found. This could be explained by the fact that in severe stages of lymphedema, where skin fibrosis and accumulation of extracellular matrix occurs, 1 elastic fibers might be destroyed. The elasticity parameter is therefore probably not applicable for a solitary follow-up measurement after treatment. However, elasticity parameters might be very useful in the late stages of lymphedema where fibrosis of the skin occurs despite a constant volume of the limb.
Considering that a relatively small population group is used in this study, individual patients might have had a big influence on results and significance. If elasticity parameters are to be used as a follow-up or diagnostic tool in clinical practice, research should be further carried out in a prospective setting with more patients in different stages of lymphedema, and measurements taken before and after lymphedema treatment. Subgroup analyses can then be performed to investigate for which purposes in clinical practice the Cutometer measurements are most relevant.
Our Corneometer measurements showed no significant differences for levels of hydration in the lymphedematous arm compared to the contralateral healthy arm. This is explained by the fact that the Corneometer mainly measures the hydration state of the stratum corneum of the skin. 34 Fluid in lymphedema usually accumulates in the subcutaneous tissue of the arm, which cannot be measured on the skin surface. Measurements with use of tissue's dielectric constant (TDC) have shown a significantly higher amount of local tissue water in lymphedematous arms when compared to healthy arms or arms of breast cancer patients prior to surgery.35,36 TDC measurement might therefore be more suitable for assessing local tissue water in BCRL then the Corneometer measurement.
Conclusion
In this article a new method for measuring skin elasticity of upper limb lymphedema is proposed. This study showed an impaired elasticity for the skin of the lower arm in lymphedema compared to the contralateral healthy arm. There is no significant difference in elasticity in skin of both arms in healthy individuals.
This study reports promising evidence for the use of Cutometer device in the evaluation of BRCL. Further research is planned that includes a larger population in a prospective setting in subgroups for different stages of lymphedema, so subgroup analyses can be performed. The use of the Cutometer as a diagnostic or follow-up tool in clinical practice can then be more extensively evaluated.
Footnotes
Acknowledgments
We wish to acknowledge the help provided by Maaike Erends with the organization of this project. All subjects are thanked for their participation in this study.
Author Disclosure Statement
No competing financial interests exist.