
Abstract
Abstract
Background:
Lymphangioleiomyomatosis (LAM) is a tumor consisting of benign-looking neoplastic cells, but its wretched clinical outcome often resembles a malignant disease. LAM cell clusters (LCCs), unique microstructures commonly found in LAM-associated chylous effusion, are aggregates of LAM cells rimmed by lymphatic endothelium. LCCs seem to be crucial participants in the dissemination and progression of LAM.
Methods and Results:
LCCs isolated from LAM-associated chylous effusion were embedded in a three-dimensional (3-D) culture gels, and then placed in a humidified CO2 incubator. During serial observations of their morphological changes, we found tube formations with lymphatic endothelial cells when LCCs settled side by side in 3-D gels. On the other hand, when LCCs were embedded separately enough to be isolated at their initial sites of settlement in the gels, each of LCCs gradually broke down, leaving a “cyst-like” hole after 7 days at the site where LCCs initially resided. Finally, we demonstrated that “cyst-like” hole formation in 3-D gels was inhibited with treatment with doxycycline or recombinant human VEGF receptor-3.
Conclusions:
We consider that our observation of this sequence in vitro illustrates how LCCs behave in vivo while enacting their important role in the progression of LAM. Our results indicate that the 3-D gel culture system for LCCs is a useful tool for exploring the effects of new therapeutic drugs under conditions when LCCs are constantly available.
Introduction
P
Also peculiar to LAM is the formation of organized microstructures with a diameter of approximately 50 to 150 micrometers: LAM cell clusters (LCCs), 2 LAM cell aggregates rimmed by lymphatic endothelium. They are usually found histologically within LAM-associated lymphatic vessels of lymph node as well as lung tissues or cytologically in chylous fluids of pleural, peritoneal or pericardial effusion. 3 We assume that they arise from LAM nodules by lymphangiogenesis-mediated shedding into the lymphatic circulation and have a role in the dissemination and progression of this disease. 2
However, how LCCs metamorphose to LAM nodules or cysts at sites where they have settled remains unknown. Therefore we adapted here a three-dimensional (3-D) culture system to scrutinize LCCs and to elucidate the morphogenesis of LAM as a model of LAM's clinical behaviors.
Materials and Methods
Smears of chylous fluids obtained from LAM patients were prepared with Papanicolaou's stain and immunostained with antibody for VEGFR-3 (Flt-4, dilution 1:50, R & D Co. Ltd., Minneapolis, MN) for detecting LCCs, as described previously. 3 To isolate LCCs, chylous fluid was placed in a Falcon® 40 μm Cell Strainer (BD Falcon, Amsterdam, The Netherlands). LCCs trapped in the strainer were washed with phosphate-buffered saline (PBS) to reduce contamination of lymphocytes and mesothelial cells.
The strainer was then inverted for placement on a culture dish and the LCCs were collected in PBS gently pouring onto the reverse side of the strainer. Under an inverted microscope (TS100, Nicon Corporation, Tokyo, Japan), one or a few LCCs were manually aspirated into a 200 μm micropipette and then seeded in a prepared 3-D culture gel (3D collagen cell culture system, Chemicon International, Temecula, CA) in a 6-well culture plate (Sigma-Aldrich Co. LLC., St. Louis, MO) on ice. Then they were incubated at 37°C in a conventional CO2 incubator.
We observed them under the inverted microscope until 14 days after seeding. 10 LCCs each in 3D culture system which included none, 10, or 50 μg/mL of doxycycline hydrochloride (MP Biomedicals, LLC., Santa Ana, CA), and 1 or 5 μg/mL of recombinant human VEGFR-3-Fc (rhVEGFR-3-Fc) chimera (R&D Systems,Inc., Minneapolis, MN). We took digital photographs of each “cyst-like” hole on day 1 to 5 using a digital camera (DS-5M-L1, Nikon Corporation) and measured pixels of their maximum diameter on a computer. To compare the diameter of hole among groups, the diameter of hole measured on each day was normalized by the diameter of day 1.
Statistical analysis was performed using the Kruskal–Wallis test (StatMate III, ATMS, Tokyo, Japan). A p-value of <0.05 was considered to be statistically significant. As a control experiment for the 3-D LCC culture, spheres of human lymphatic endothelial cells (HLECs) 4 , human uterine smooth muscle cells (HUSMCs, Lonza Walkersville, Inc. Walkersville, MD), or human lung fibroblasts (HFL1, American Type Culture Collection, Manassas, VA) were prepared by culturing each cells (approximately 4–9 × 105 cells) in Ultra Low Cluster Plate (6-well with Lid, Flat Bottom, Ultra Low attachment, Corning Inc., Corning, NY) at 37°C in a conventional CO2 incubator for 3 days. These “control sphere” were embedded in 3-D culture system as LCCs were done.
To detect lymphatic endothelium or LAM cells in 3-D culture gel, a gel was fixed with 4% paraformaldehyde at 4°C for 16 h, washed with PBS three times and immersed in PBS with 2% bovine serum albumin, and finally incubated with D2-40 antibody (1:200 dilution; DAKO Cytomation), alpha-smooth muscle actin (1:200 dilution; Dako Cytomation, Glostrup, Denmark) at room temperature for 4 h. After washing with PBS three times, it was incubated with alkali phosphatase-conjugated secondary antibody (Nichirei Biosciences Inc., Tokyo, Japan) at room temperature for 1 hour and stained with Fast red (Farma, Tokyo, Japan). Non-immune IgG1 (1:200 dilution; Dako Cytomation) were utilized as a negative control for immunocytochemistry.
The procedures followed were in accordance with the ethical standards of the ethics committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. This study was approved by the Ethics Committee of Juntendo University.
Results
Representative microscopic features of LCCs on smear preparation are presented in Figure 1; they are globular-shaped microstructure composed of a monolayer of lymphatic endothelium at the surface and an aggregates of LAM cells inside. When LCCs happened to settle side-by-side in a gel, tube-like protrusions emerged and radiated from the surfaces of LCCs and then interconnected with those of the neighboring LCCs (Fig. 2A). Immunocytochemistry demonstrated that these fibers were composed of lymphatic endothelium positive for D2-40 (Fig. 2B), indicating that lymphatic vessel-like tube formation derived from lymphatic endothelium on LCCs.
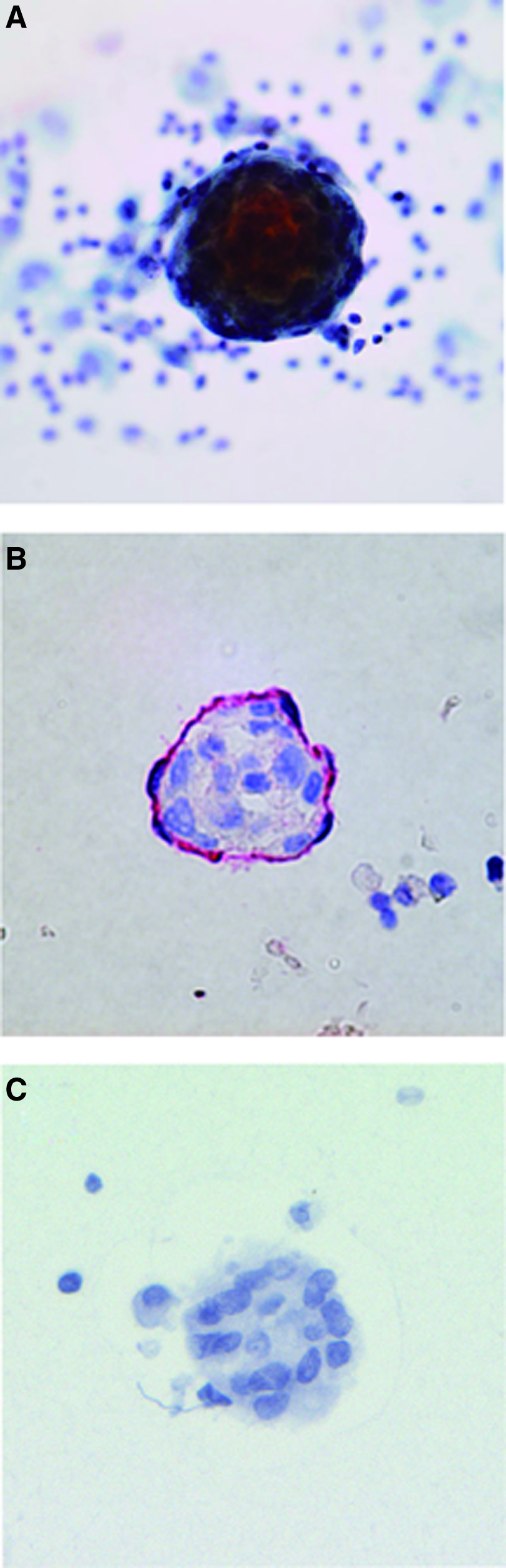
LCC in chylous fluid. The cluster is composed of aggregated LAM cells and surrounded by lymphocytes and macrophages

Lymphatic vessel-like tube formation arises from LCCs in 3-D culture system. Tube-like protrusions between neighboring LCCs appear on the day 3 after seeding,
In contrast, LCC that settled as solitary units (instead of alongside other LCCs) in a gel, underwent peeling away of their lymphatic endothelial covering by day 3 after seeding. The cluster then broke down to disappear by day 5 after seeding (Fig. 3A–3D). However, a “cyst-like” hole emerged concomitantly at the place where the cluster formerly existed (Fig. 3E–3G). Spindle-shaped cells were clearly recognizable at the bottom of a “cyst-like” holes and small “daughter” cell aggregates gradually formed at the periphery of the “cyst-like” hole (Fig. 3G and 3H, respectively).
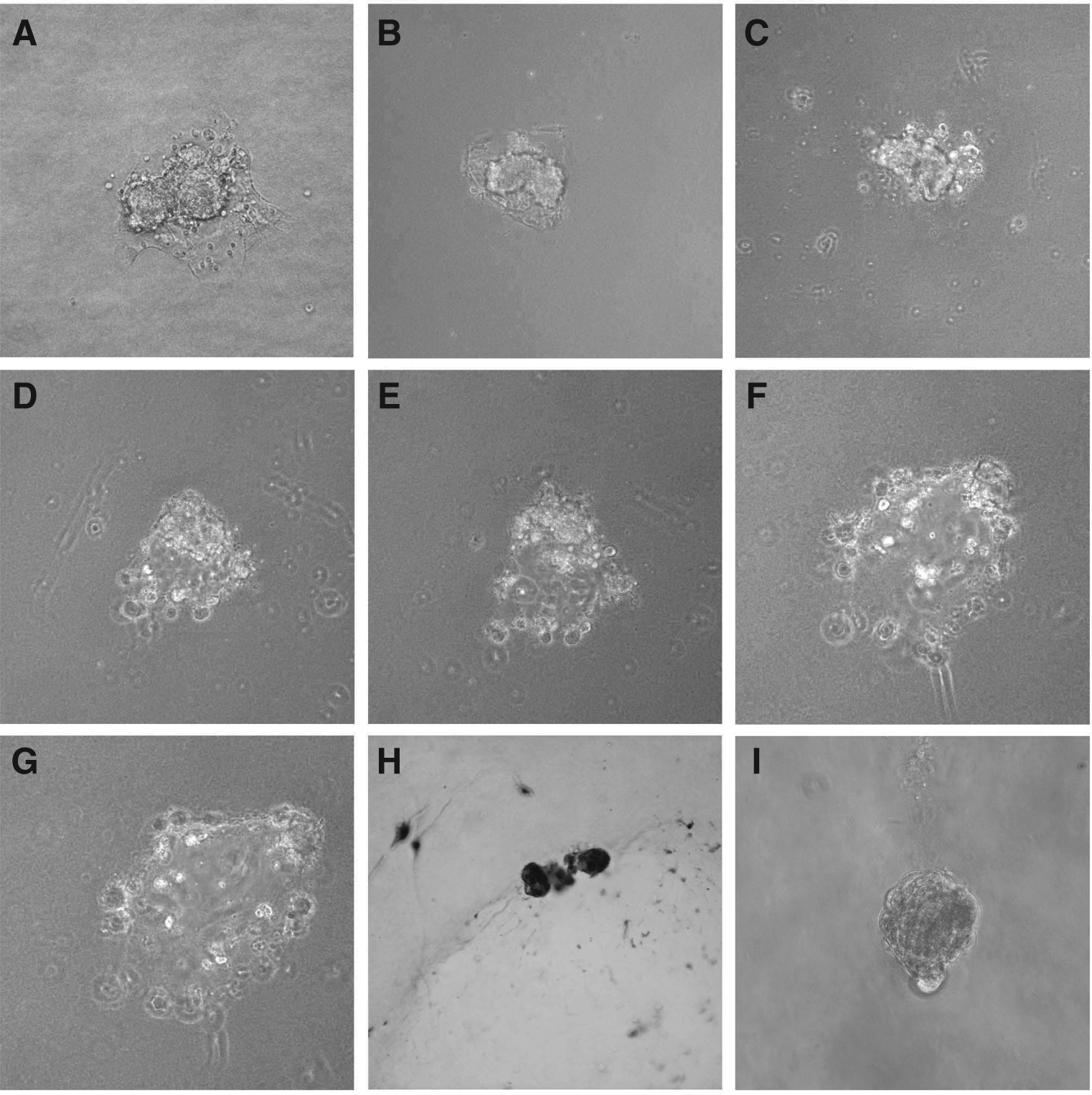
Formation of “cyst-like” hole in the 3-D culture gel. Lymphatic endothelium has peeled away from the surface of a cluster, and disappeared by day 5 after seeding (
None of these cells appeared to survive beyond day 14 after seeding. The “cyst-like” hole formation is characteristic of LCCs in 3-D culture system because spheres of other mesenchymal cells such as HFL1 (human fetus lung fibroblasts) or human uterine smooth muscle cells did not form “cyst-like” hole structure in the 3-D culture system (Fig. 3I) (only the representative result of spheres of uterine smooth muscle cells were shown). The results presented in Figures 2 and 3 are a representative of three independent experiments using LCCs from three unrelated patients with sporadic LAM.
Next we examined whether either doxycycline or rhVEGFR-3-chimera prevents LCCs from forming “cyst-like” hole in 3-D culture system. When doxycycline was include in a gel at 10 or 50 μg/mL, the diameter of “cyst-like” hole was significantly smaller at day 2 and 5 (10 μg/mL) or at all days examined (50 μg/mL) (Fig. 4A). On the other hand, the diameter of hole was significantly smaller only at day 5 when rhVEGFR-3-Fc chimera was utilized at 5 μg/mL (Fig. 4B).
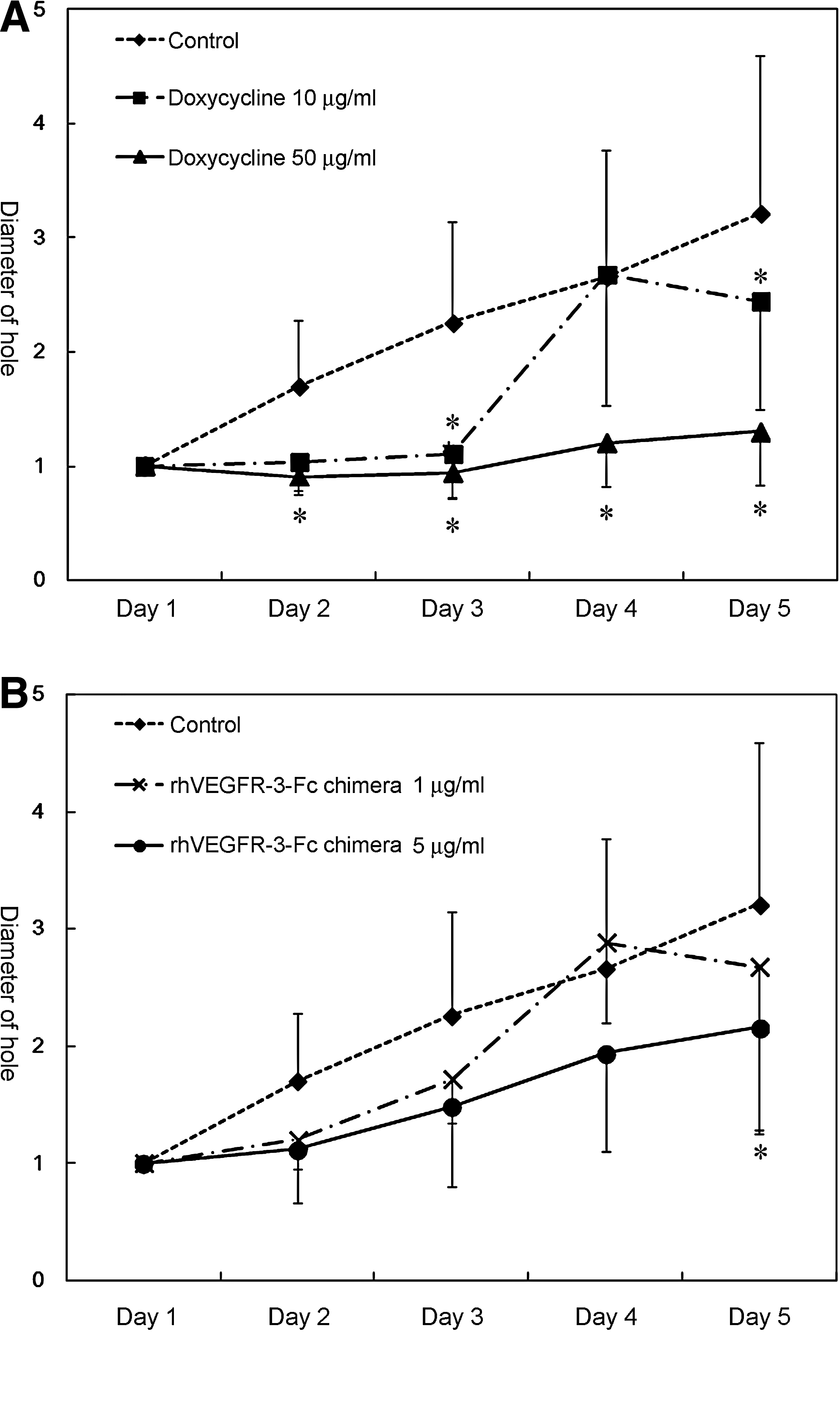
Doxycycline or recombinant rhVEGFR-3-Fc chimera prevents LCC from forming a “cyst-like” hole in 3-D culture system. LCCs treated with 10 or 50 μg/mL of doxycycline
Discussion
Our observations in vitro in this 3-D culture system for LCCs illustrate graphically the likely behavior of LCCs in vivo in LAM patients. Thus, lymphatic endothelial cells on the surface of a LCC would be able to proliferate and contribute to lymphangiogenesis at the site where they settle from lymphatic circulation; in contrast, an aggregate of LAM cells inside a LCC would be likely to unravel and generate cysts in the lungs.
We propose that the sequence described here is an in vitro disease model of LAM. We speculate that both processes would proceed through expression of matrix metalloproteases5,6 and VEGF-D 7 by LAM cells, the mechanisms currently believed to be operative from the results of precedent studies. Actually, our proposal seems to be supported by the findings that the addition of doxycycline (an inhibitor of matrix metalloproteases) or rhVEGFR-3-Fc chimera (an inhibitor of interaction between VEGF-D and VEGFR-3) significantly inhibited “cyst-like” hole formation by LCCs. It is unfortunate that we have had no opportunity to test the effect of rapamycin on this 3-D model system due to the very limited availability of LCCs.
Another weakness in our 3-D culture system as a model of LAM is a lack of alveolar epithelial cells that might have some role in the cyst formation of the LAM lungs. However, this 3-D culture system for experimentation with LCCs may be a useful bioassay in elucidating the mechanisms of morphogenesis as well as metastasis and/or invasion of LAM(1,2,8) and hence in developing new therapeutic agents for LAM once LCCs were obtained or prepared in vitro.
Footnotes
Acknowledgment
The authors thank Ms. Phyllis Minick for her excellent assistance in the writing of English.
Sources of Support: This study was supported in part by Grant-in-Aid for Scientific Research No. 21659210 (Seyama K) from the Ministry of Education, Culture, Sports, Science, and Technology, Japan; a grant to the Respiratory Failure Research Group (Seyama K) from the Ministry of Health, Labour and Welfare, Japan; the High Technology Research Center Grant from the Ministry of Education, Culture, Sports, Science, and Technology, Japan; and the Institute for Environmental and Gender-Specific Medicine, Juntendo University Graduate School of Medicine, Tokyo Japan.
Author Disclosure Statement
No competing financial interests exist.