
Abstract
Abstract
Background:
Lymphangiomatosis is a rare disorder of the lymphatic system that can impact the dermis, soft tissue, bone, and viscera and can be characterized by lymphangiomas, swelling, and chylous discharge. Whether disordered lymphangiogenesis in lymphangiomatosis affects the function and anatomy of the entire systemic lymphatic circulation or is localized to specific sites is not fully known.
Methods and Results:
A 35-year-old Caucasian female diagnosed with whole-body lymphangiomatosis at 2 months of age and who continues to present with progressive disease was imaged with near-infrared fluorescence lymphatic imaging. While the peripheral lymphatics in the extremities appeared largely normal compared to prior studies, we observed tortuous lymphatic vessels, fluorescence drainage from the peripheral lymphatics into lymphangiomas, and extensive dermal lymphatics in the left thigh and inguinal regions where the subject had previously had surgical assaults, potentially indicating defective systemic lymphangiogenesis.
Conclusions:
Further research into anatomical and functional lymphatic changes associated with the progression and treatment of lymphangiomatosis could aid in understanding the pathophysiology of the disease as well as point to treatment strategies.
Introduction
L
The disease can present at any time during life although it generally manifests prior to adulthood. 4 Although lymphangiomas are typically benign, significant morbidities can occur when they invade the lungs, skeleton, or other critical organs and/or compress adjacent structures. 2 The etiology of lymphangioma is poorly understood, but is thought to be a result of congenital defects in the formation of the lymphatic system in which lymphatic cisterns become detached from or fail to connect to the normal lymphatics.5,6 Treatment options are limited and typically include diet, drainage or surgical removal, sclerotherapy, radiation therapy, and/or laser treatment.2,7,8 Unfortunately, owing to the difficulty in identifying and destroying all the abnormal lymphatics associated with a lymphangioma, there tends to be a high rate of recurrence. 4
Herein, we report the case of a patient with a history of lymphangiomatosis who presented to our clinic for imaging of the peripheral lymphatics using investigational, near-infrared fluorescence lymphatic imaging (NIRFLI). We sought to determine whether the peripheral lymphatics were altered in anatomy and function.
Subject and Methods
This study was conducted under US Food and Drug Administration (IND#: 102,827) and University of Texas Health Science Center at Houston Institutional Review Board approval and in accordance with the Helsinki Declaration of 1975, as revised in 2008.
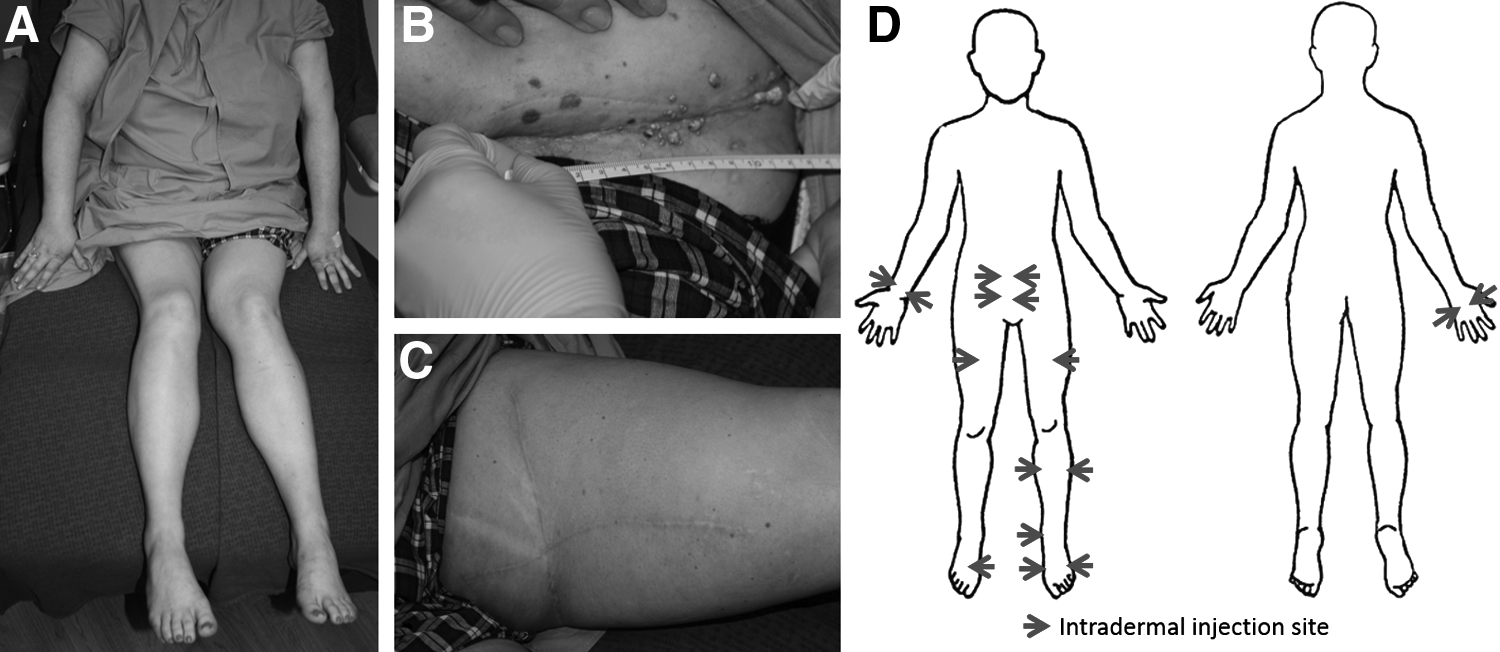
The subject was a 35-year-old Caucasian female who was diagnosed with whole-body lymphangiomatosis at 2 months of age and, as detailed in Table 1, had an extensive medical history related to the disease including two lung surgeries, multiple debulking procedures, left and right vulvectomies including bilateral inguinofemoral lymphadenectomy, as well as a history of ascites, chylous ascites, and pleural effusion. Reports from truncal CT scans 5 months prior to presentation in our clinic indicated the presence of lymphangiomas and pockets of fluid throughout the thoracic, abdominal, and pelvic regions. Figure 1A–1C shows images of the subject's arms and legs just prior to imaging, as well as images of the lymphangiomas observed in the left pelvic region and the extensive scarring in the left leg from previous tissue expansion and debulking procedures. The subject had no history or evidence of lymphedema (Fig. 1A).
The clinical appearance of the patient's
The subject presented at our clinic for NIRFLI, an investigational technique which enables the noninvasive visualization of peripheral lymphatic architecture and contractile function following the intradermal administration of indocyanine green (ICG). NIRF lymphatic imaging has been previously reported, and distinct differences between healthy and diseased lymphatics, such as in lymphedema, have been noted.9–12 To maximize the opportunity to visualize the lymphatics in the subject we opted to focus our NIRF lymphatic imaging primarily on one leg and one arm, with a secondary focus on the abdomen and the contralateral leg. Because the subject reported that her left leg and right arm were more symptomatic than their corresponding contralateral limbs, we selected those limbs as our primary focus for imaging.
Following informed consent, a total of sixteen injections of 25 μg of ICG in 0.1 mL of saline were administered. Initially we administered six injections in the left leg, and four injections in the right arm, as shown in Figure 1D. After imaging the leg and arm, four additional injections were administered in the abdomen near the navel, and two final injections were administered the right leg, with each set of injections followed by imaging. Immediately after injection, images were acquired for 2 hours by illuminating the limbs with the diffuse output of a 785 nm laser diode to excite the ICG laden lymph. A custom, intensified charge coupled device (ICCD) camera was then used to collect the resultant fluorescent signal (830 nm) emanating from the lymphatics. Exposure times of 200 ms allowed the acquisition of movies of contractile lymphatic function.
Images were analyzed to determine the presence of lymphatic abnormalities such as dermal backflow, characterized by dense networks of fluorescent lymphatic capillaries and/or extravascular fluorescence, as well as dilated and/or tortuous lymphatic vessels. The movement of fluorescent lymph through the lymphatics was also noted and, as described previously, 11 its contractile propulsion was measured by calculating the average propulsion velocity of packets of fluorescent lymph propagating between two regions of interest along the lymphatic vessel. The period between propulsion events was determined by measuring the time lapse between two successive packets of fluorescent lymph propagating through a single region of interest. The subject was contacted 24 hours after imaging to verify that no adverse events occurred. The results of imaging were not used in clinical care. Unfortunately, as a consequence of her disease, the subject expired several months after imaging.
Results
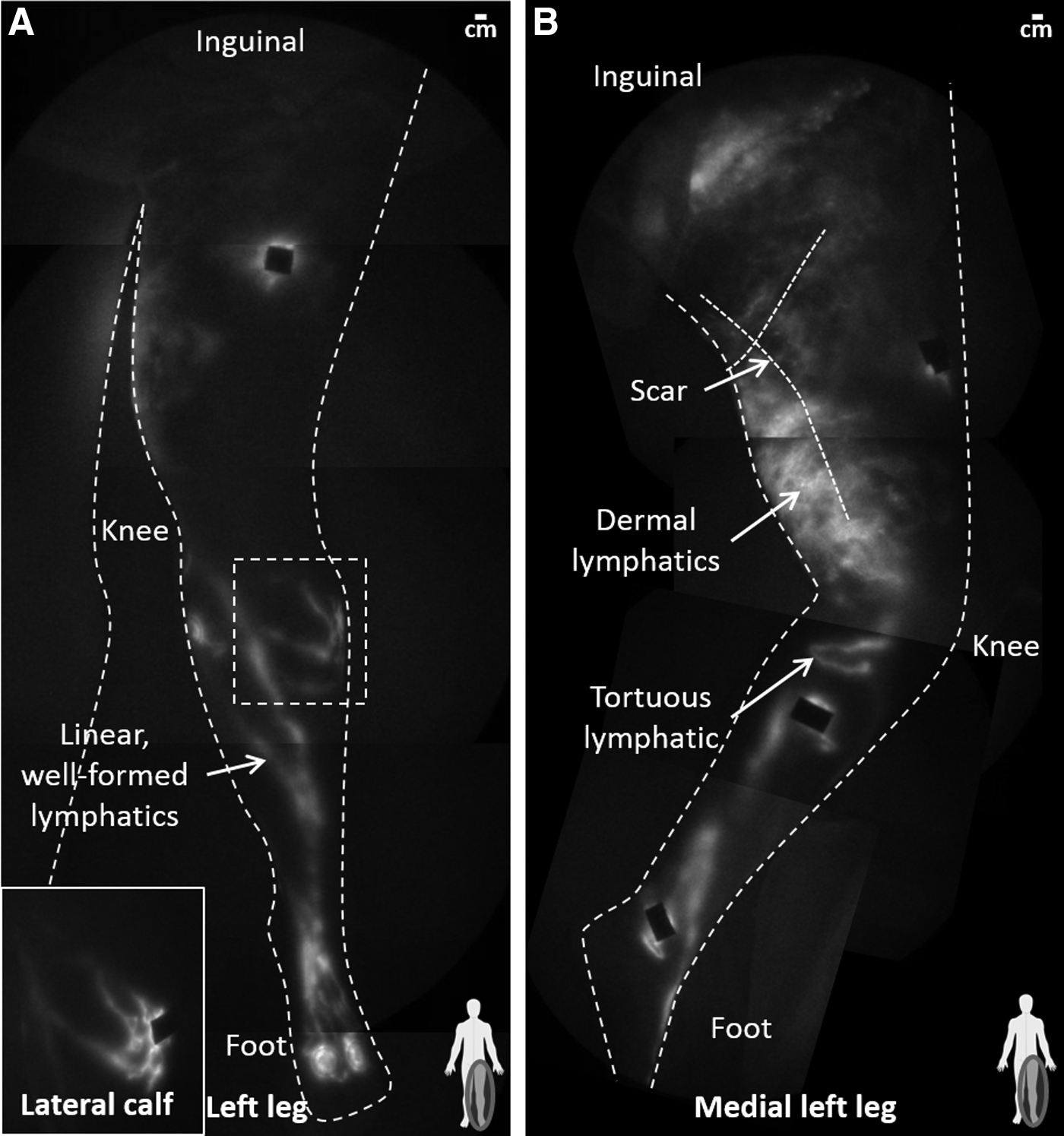
As shown in Figure 2, the lymphatics in the lower left leg were generally well defined with active lymphatic propulsion (see Supplementary Video 1; supplementary material is available online at www.liebertpub.com/lrb) although tortuous lymphatics were observed in the lateral and medial calf. Furthermore, the peripheral lymphatics in the upper left leg manifested extensive dermal lymphatics that actively propelled fluorescent lymph from the medial thigh towards the lateral thigh (Supplementary Video 2). In addition, packets of lymph are clearly observed being propelled through a larger and deeper lymphatic vessel from the injection site in the left thigh towards the inguinal region despite the fact that the vessel itself is not clearly delineated beneath the fluorescent dermal lymphatics.
Montages of the
The presence of larger functional lymphatics away from the medial thigh in conjunction with the active propulsion seen in the medial dermal lymphatics may explain why this subject had not developed any sign of lymphedema despite the repeated surgical trauma inflicted on the medial thigh. In contrast, while fluorescent dermal lymphatics, commonly referred to as dermal backflow, are frequently seen in subjects with lymphedema, they typically have little observable propulsion and, more often than not, appear to bloom from, instead of delivering lymph to, the larger lymphatic vessels.10,11,13,14 No adverse events were observed during this study.
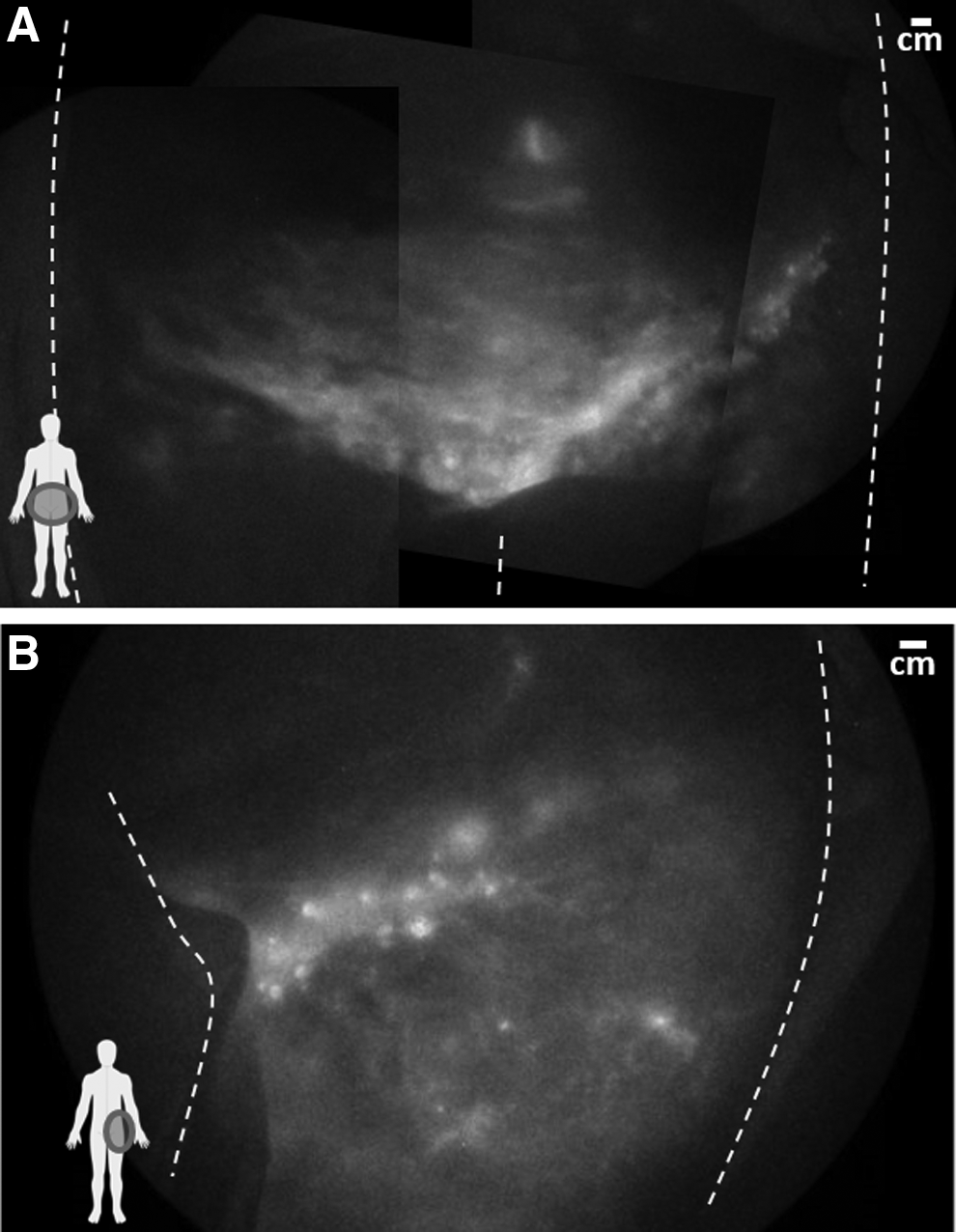
The fluorescent lymph in the left inguinal region drained into the right inguinal region, as shown in Figure 3A, and the lymphangiomas on both the left and right sides were fluorescent (Fig. 3B). The crosstalk between the left and right inguinal regions is unusual, although it is similar to the pelvic regions of some lymphedema subjects with genital or lower abdominal involvement, 15 as well as a subject with Parkes-Weber syndrome who also had fluorescent lymphoceles on the groin. 16
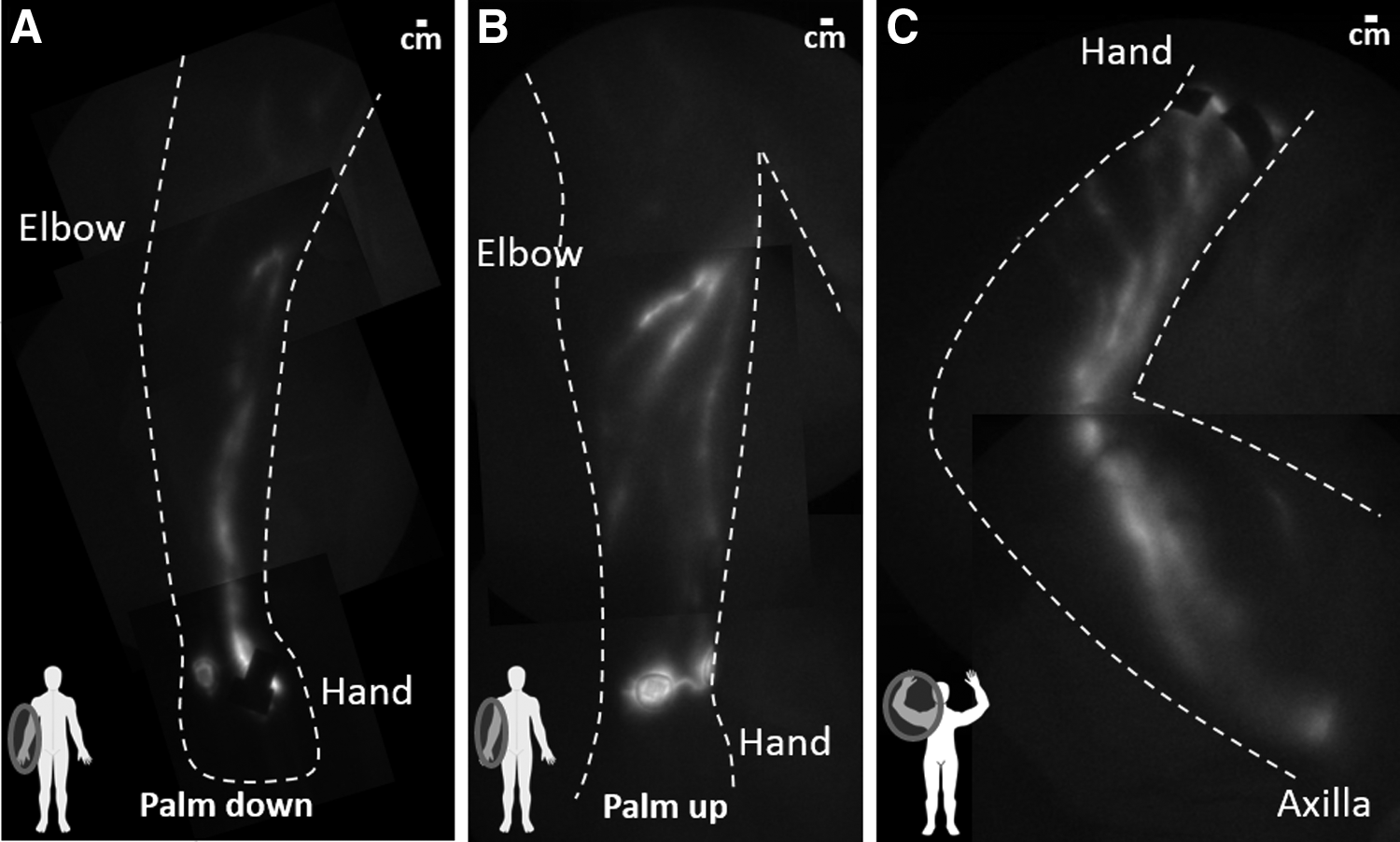
As shown in Figure 4, and with the one exception of a tortuous fluorescent lymphatic vessel connecting the injection sites on the medial wrist, the lymphatics in the right arm were linear and well-defined as typically seen in healthy subjects. Fluorescent nodes were also observed in the axilla (Fig. 4C).
The lymphatics in the right arm with
The lymphatics in the abdomen above the navel were tortuous and drained towards the axillary regions, as shown in Figure 5. Dermal backflow was observed around the injection sites above the navel, indicating lymphatic communication across the midline of the subject. In addition, a tortuous lymphatic vessel, which was very faint, was observed actively propelling fluid from the left injection site towards the right axilla (Supplementary Video 3). The injections below the navel had no clear lymphatic drainage pathway towards the inguinal or axillary regions, although there was a fluorescent lymphatic vessel observed between them.
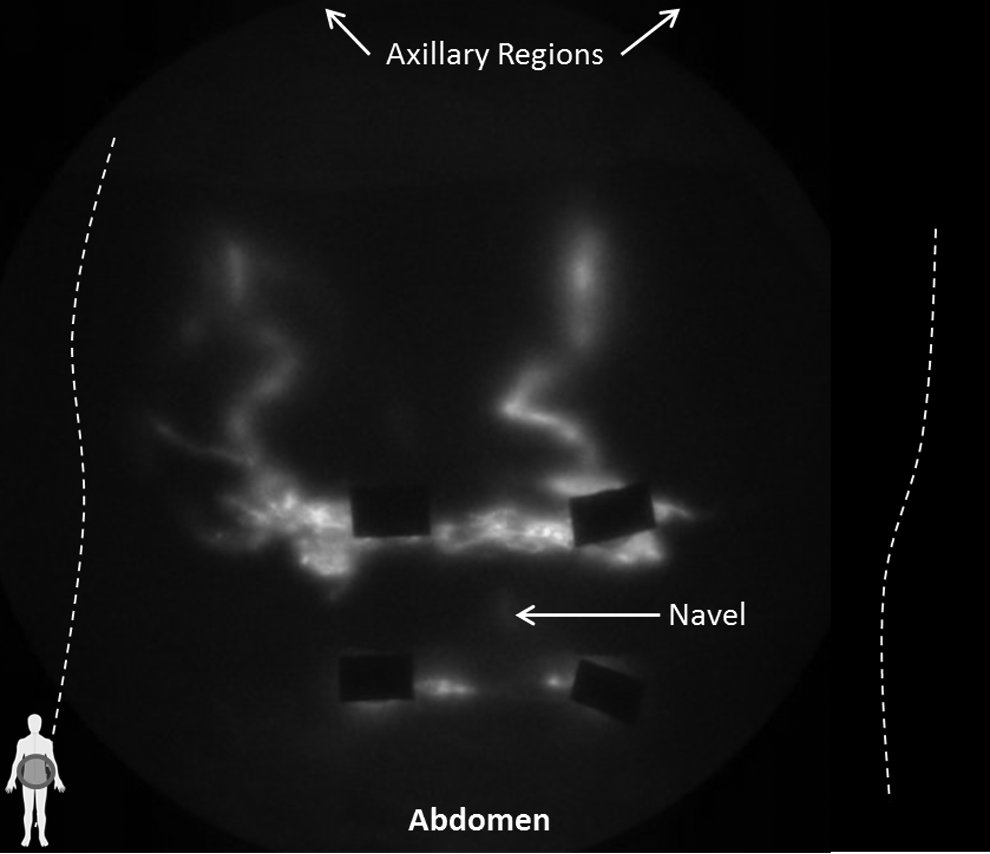
The lymphatics in the abdomen above the navel were tortuous and drained towards the axillary regions. Fluorescent lymphatic capillaries were also observed around the injection sites above the navel. The injections below the navel had no clear lymphatic drainage pathways.
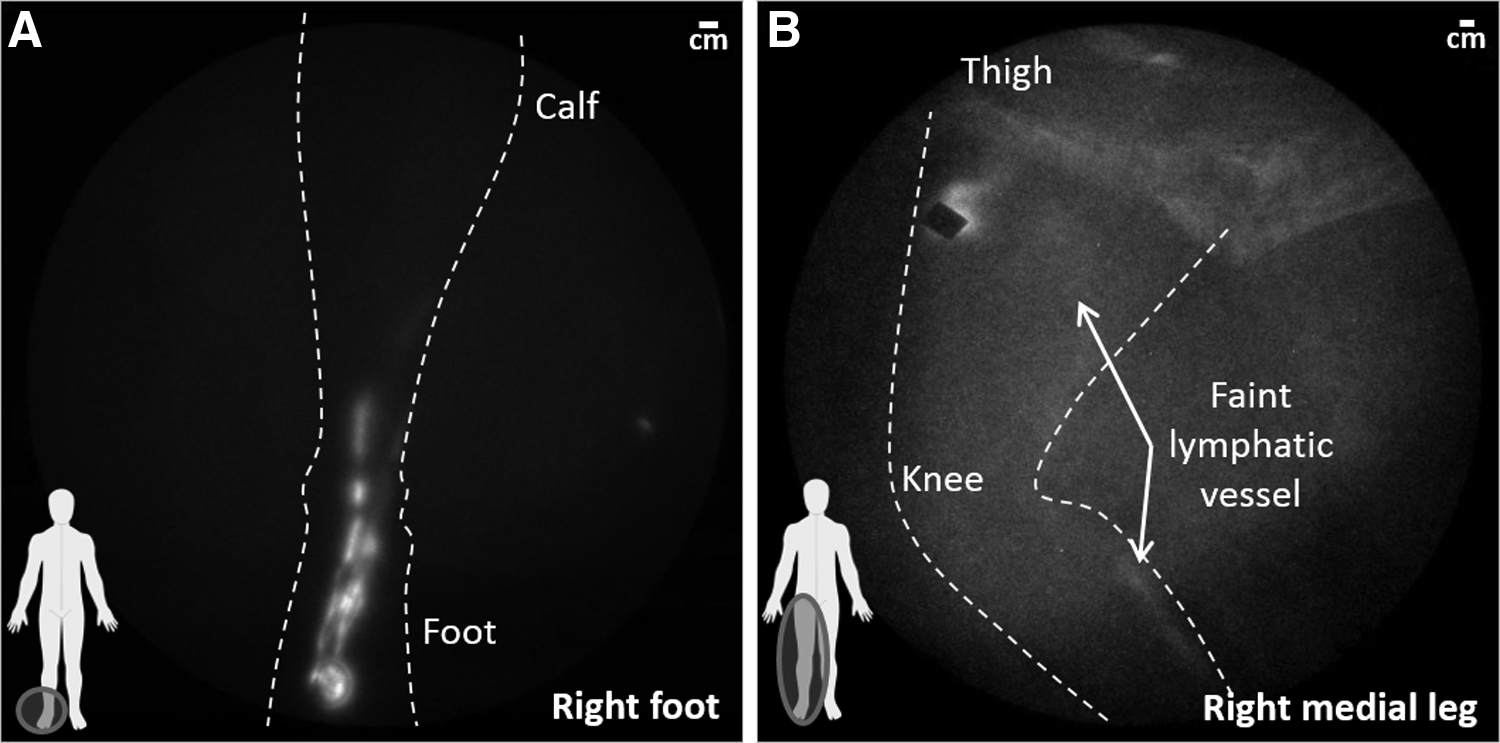
The lymphatics in the lower right leg (Fig. 6A) were linear and well-defined though the lymphatic vessel draining from the foot to the inguinal region was very faint (Fig. 6B), most likely owing to the fact that we only administered one injection on the foot and lower leg. The injection sites on the right leg drained toward the right inguinal with no indication of dermal backflow in the thigh.
The lymphatics in the
The average velocity in the well-defined lymphatics observed in the legs and arm was 0.9 cm/sec and 1.1 cm/sec, respectively, with an average period of 28 sec between propulsion events. These values are similar to those that we have measured previously in healthy subjects 11 and, in the case of the arm velocity, is similar to the fastest transit time reported by Yamamoto et al. 17 The dermal lymphatics observed in the medial thigh also actively propelled lymph towards the lateral thigh (Supplementary Video 2) with an average velocity of 1.4 cm/sec and an average period of 19 sec. The faster propulsion rates in these dermal lymphatics may enable these smaller, more superficial lymphatics to remove excess fluids adequately from the medial thigh, thus preventing the accumulation of interstitial fluids and proteins that are indicative of lymphedema and its associated sequelae.
While the subject reported multiple lymphangiomas throughout her body, the lymphatics in the right arm, lower left leg, and the abdomen largely appeared to be intact with contractile function. The lack of ICG pooling in those areas indicate that any abnormal lymphatics associated with local lymphangiomas are indeed disconnected from the normal lymphatics, as has previously been reported.6,18 The obvious exception to this are the extensive fluorescent dermal lymphatics observed in the upper left leg and bilateral inguinal regions, and the presence of fluorescence in the superficial lymphangiomas located in the inguinal region. However, these dermal lymphatics may not be a direct result of the lymphangiomatosis itself, but rather a result of significant lymphatic trauma associated with the subject's bilateral vulvectomies and inguinofemoral lymphadenectomies, as well as the placement of a tissue expander in the left thigh (Table 1).
One may speculate that the abnormal anatomy and function may be due to defects in lymphangiogenesis following surgical assault. Indeed, significant scarring is readily seen on the left medial thigh (Fig. 1C) where the extent of fluorescent dermal lymphatics is the greatest (Fig. 2B). Some, if not all, of the surviving lymphatics in the legs likely leak lymph directly into the inguinal basins where it is subsequently taken up by the other collecting lymphatics, including both the normal lymphatics and the abnormal lymphatics associated with the lymphangiomas.
Because the abnormal lymphatics are not thought to be directly associated with normal peripheral lymphatics, the ability to use NIRFLI to find and identify cavernous and/or cystic lymphangiomas may be limited, and conventional imaging modalities such as MRI and ultrasound, which may not require exogenous contrast to discriminate fluid filled voids from surrounding tissues, may be needed. However, as shown herein, NIRFLI may provide a unique opportunity to visualize cross communication between the abnormal lymphatics associated with lymphangiomas and the normal lymphatics if/when it does occur.
In addition, if ICG were to be injected directly into a known lymphangioma, the fluorescent signal could potentially help to identify the extent of the diseased tissues and to plan and carry out appropriate therapeutic procedures. For example, as has been shown previously for sentinel lymph node dissection (for review, see Zhu and Sevick-Muraca 19 ) and surgical guidance of lymphaticovenular anastomoses,20,21 NIRFLI may provide opportunities for surgical guidance in the resection of all the abnormal lymphatics associated with a lymphangioma, thereby reducing the chance for recurrence. This would be particularly useful in the resection of localized lymphangiomas that have a higher probability for cure if all the abnormal lymphatics are removed.
Conclusion
We have demonstrated the use of NIRFLI to image normal and abnormal lymphatics in a subject with lymphangiomatosis. While NIRFLI may be limited in its use to discover deep abnormal lymphangiomas, we demonstrate its potential use to discover communication between the lymphangiomas and normal peripheral lymphatics. Additional studies are needed to determine if NIRFLI could provide a needed tool to guide intervention to destroy abnormal lymphatics associated with known lymphangiomas and visualize changes that are associated with disease progression.
Footnotes
Acknowledgments
The authors would like to thank Karen Gore and J. Rodney Morrow for clinical and regulatory assistance. This study was funded in parts by the Lymphatic Malformation Institute and grants from the National Institutes of Health R01 HL092923 (EMS) and U54 CA136404 (EMS).
Author roles: NIRF lymphatic imaging and analysis: JCR; Conceptualization: EMS and CEF; Writing and critical review: JCR, EMS, and CEF. All authors have approved the manuscript.
Author Disclosure Statement
JCR and EMS own stock in a UTHealth portfolio company, NIRF Imaging, Inc., which seeks to commercialize the NIRF lymphatic imaging technology. JCR has also received consulting fees from NIRF Imaging, Inc.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.