
Abstract
Abstract
Background:
Early diagnosis of breast cancer treatment-related lymphedema (BCRL) is of great importance for longstanding treatment results. Tissue dielectric constant (TDC) and bioimpedance spectroscopy (BIS) both have a potential for early diagnosis, but have not been compared.
Methods and Results:
One hundred women, treated for breast cancer with breast surgery, axillary dissection, and radiotherapy, were examined within one year after breast cancer treatment, as part of the follow-up procedure. Affected/at-risk and contralateral arms were measured with the TDC technique specific to localized skin water content and the BIS technique assessing arm extracellular fluid (ECF). Thirty-eight patients were clinically diagnosed for lymphedema (38.0%). The sensitivity and specificity for the TDC method were 65.8% and 83.9%, and for BIS method 42.1% and 93.5%, (p<0.001 and NS), respectively. Of all lymphedema, 18.4% were detected only by TDC and 2.6% by BIS. Affected arm to contralateral arm TDC ratios for upper arm and forearm, 1.56±0.49 and 1.28±0.33, demonstrating the localized feature of the TDC measurements were significantly greater than the BIS arm ratio 1.12±0.12 (both p<0.001).
Conclusions:
Discrepancies between TDC and BIS techniques in assessing lymphedema are related to different measurement techniques and assessed tissue water components. Independently of selected technique-specific threshold limit, the TDC technique was more sensitive than the BIS technique in the early assessment of BCRL and demonstrated that nearly 20% of early lymphedema are only superficially localized. The results further supported the complementary role of TDC and arm volume measurements as a highly diagnostic method for early lymphedema.
Introduction
E
Bioimpedance analysis (BIA), bioimpedance spectroscopy (BIS), and tissue dielectric constant (TDC) using electric current or electromagnetic fields in the noninvasive assessment of tissue fluids are available to aid clinical evaluation of BCRL. The bioimpedance systems BIA or BIS apply one or several kHz to 1 MHz frequencies to estimate arm extracellular fluid (ECF) in patients with BCRL.2–6 In the bioimpedance method, voltage between measurement electrodes is registered in response to imposed electric current between drive electrodes positioned on the hands and foot. This information is used to determine the electrical resistance of each arm. Difference in the calculated resistance between affected and contralateral sides yields a parameter describing a lymphedema-related increase of the ECF space in the affected limb. However, it is not possible to determine in which tissue component this increase of the ECF fluid is localized. Since bioimpedance measurements above 30 kHz decrease sensitivity to changes in ECF, they are not considered reliable for early detection of lymphedema. 7
Using age, sex, and race-specific validated fluid distribution equations, 8 single-frequency BIA analyzers allow the determination of body composition parameters, including extracellular water, in ‘average’ subjects without significant fluid abnormalities and changes in fluid ion status. 9 Abnormal fluid distribution due to arm lymphedema may lead to marked errors in the body composition parameters. 10 If the shape of a lymphedematous limb differs from that of the normal limb, tissue shape correction factors have been applied in the estimation of resistance of extra- and intracellular fluids by BIA analysis. 2 In multi-frequency BIS measurement, such shape or composition based geometric factors are not applied. Tissue composition changes in inter-arm fat and fibrotic tissue are suspected to have impact on the diagnosis of confirmed lymphedema.7,11
The TDC method applies a high-frequency electromagnetic (EM) field (300 MHz) through an open-ended coaxial probe to measure the dielectric properties of biological tissues.12–15 In human tissues the dielectric properties are strongly related to tissue water content.16,17 Since the water content in skin is high and the dielectric constant of water is much greater than those of macromolecules (mainly proteins and proteoglycans) and adipose tissue, the measured TDC value is directly proportional to water content in skin.14,16,18 Therefore, measurements of tissue water are best focused into skin where the first signs of lymphedema are often thought to manifest19–24 and where edema is often located.25,26 Using this approach, Mayrovitz27–28 and Mayrovitz et al.29–34 found in lymphedema patients significantly greater ratios of affected to contralateral arm TDC values than ratios of arm volumes or girths.
At the applied frequency of 300 MHz free and bound water,35–37 molecules rotating in the EM field absorb equally energy from the field. Thus their dielectric constants are equal 35 and both components absorb energy in relation to the amount of water in these components. The measured reflected part of the EM field is attenuated and phase-shifted. 38 From this reflected wave information the tissue dielectric constant (TDC) reflecting localized total water content is calculated. Unlike BIA or BIS analyzers the TDC method is applicable to assess superficial tissue water content at all body regions, not just with limbs.
When TDC and BIS methods were compared in the detection of BCRL during 24 months after radiotherapy (RT), an increase in the TDC values and inter-arm TDC ratio reflecting increase of tissue water in forearm skin and at lateral thorax was found, while BIS and limb volume measurements showed practically no increase as compared to pre-surgery values. 34 However, in these studies, arm volumes were estimated from girth measurements and thus there was no additional independent direct measurement of arm volume changes from which edema volume could be directly determined. Thus the present study was undertaken to extend the prior initial findings using direct water displacement volume determinations as a comparison reference for changes in TDC versus BIS.
Materials and Methods
Patients
One hundred women aged 57.4±11.5 years (mean±1 SD) (range 29–84 years) treated for breast cancer with surgery including axillary lymph node dissection (ALND) and radiotherapy to the breast and axilla were included in the study (Table 1). Patients were a part of the continuous institutional follow-up program already lasting for 20 years 39 at the Lymphedema Unit, Skane University Hospital, Lund, Sweden. All procedures and measurements are orally informed, conducted in accordance with the Declaration of Helsinki and approved verbally by the patient. According to previous analysis with similar patient material at the Lymphedema Unit, the incidence of BCRL was 38.7%. 1
All patients had axillary RT as well as RT to remaining breast tissue (after lumpectomy) or to the thoracic wall (after mastectomy).
The first visit was scheduled at 3 months post-RT. However, 20 patients called or were referred to the Lymphedema Unit with arm swelling or symptoms within 3 months post-RT. Sixty-five patients were investigated within 3–6 months post-RT. Fifteen patients were investigated after 6 months. The reason for the late measurements was mainly due to practical issues such as the lack of clinical time, sick-leave, or a patient's wish to postpone the visit due to a long distance or an asymptomatic condition at 3 months. However, with later occurrence of arm swelling they wanted to be examined. In the whole material the first measurement visit was realized at 4.5±2.6 months post-RT (Table 1). During this visit, which occurred with all patients after the surgery and RT, the TDC, BIS, and arm volumes for affected or at-risk and contralateral arms were measured and respective arm ratios calculated.
Since the patients were not seen pre-surgery, a handedness (dominance) adjustment was used to compensate for possible natural differentials in arm volume ratios. Right arm volume in right-hand dominant women is 1.6% greater than left arm volume and 1.4% less than left arm volume in left-hand dominant women. 40 Accordingly, when setting a threshold for lymphedema based on the ratio of the volume of the at-risk or affected arm to the contralateral arm, this natural difference was taken into account. If, as is done typically, a 5% increase in the ratio is taken as the lymphedema threshold, then the threshold ratios shown in Table 2 may be calculated and used. As an example to derive the figures of Table 2, a right hand female has a right-to-left arm dominance ratio=1.016. If she has a right-sided cancer, the required threshold ratio for a 5% increase would be 1.05×1.016=1.067. If she has a left-sided cancer, her left-to-right threshold ratio would be (1/1.016) ×1.05=1.033.
Criteria for lymphedema
The three criteria in the diagnosis of lymphedema (LE) were (1) affected or at-risk arm excess volume ≥5% measured by water displacement method (WDM) and corrected for arm dominance, (2) increased subcutaneous thickness on palpation of the medial and lateral side, and (3) a patient's experience of arm tension, the latter two criteria also compared to the contralateral arms. 41 Of these three criteria, two should be fulfilled for the diagnosis of lymphedema. In 90 patients, the diagnosis was based on WDM and on criterion 2 and/or 3. In 10 patients, the diagnosis was based exclusively on criteria 2 and 3 (i.e., the dominance-corrected arm volume ratio in these patients was less than 5%). With all patients, the diagnosis of lymphedema was made by one of the authors (KJ). During the interview, a patient's experience on arm tension was registered followed by palpation of subcutaneous thickness and measurements of BIS, TDC, and arm volume, always in the same order.
Measurement systems
Water displacement method (WDM)
Arm volume was measured with the water displacement method,42–44 considered by some as a gold standard. Accordingly, the at-risk and contralateral arms were submerged in a cylindrical water container as described previously. 1 Arms were in a straight position with fist resting with the proximal phalanges at the bottom of container. Since the upper edge of the container was tightly pushed against the axilla due to the water drain pipe, the proximal site of arm volume measurement was approximately 5 cm distal to axilla. The volume displacement was measured in grams and converted into milliliters.
Tissue dielectric constant (TDC) measurement
The TDC technique in the assessment of lymphedema has been described in the literature.19,27–34 The device, (MoistureMeterD, Delfin Technologies Ltd, Finland), consists of four open-ended coaxial probes intended to measure tissue water at effective depths from 0.5 to 5 mm. The dimensions of the coaxial probes define the penetration of EM fields in tissue. 45 Physically, the effective measurement depth is defined as a depth where the EM field has attenuated to 37% of the value at the surface. 18 The probe used in this study had a diameter of 2.3 cm and an effective measurement depth of 2.5 mm. This is the probe depth that has most often been used to assess lymphedema in skin and upper subcutis.27–34
With the patient in a supine position with arms slightly abducted and outward rotated, two sites on the medial side of each arm were measured; one site on the upper arm 5 cm proximal to the antecubital fossa and one site on the forearm 5 cm distal to the antecubital fossa. The medial site was selected since by clinical experience increased thickness of subcutaneous tissue is most often found at the medial site of the arm. When the probe is gently placed on the surface of skin, the measurement starts. After 5 seconds, the dielectric constant of the measurement site (i.e., the dimensionless TDC value) can be read on the device display. At the applied EM frequency of 300 MHz, the TDC values vary between 1 (vacuum or practically air) and about 78.3 for pure water at 25°C. 46 The TDC values of the biological materials range typically between 20–50 corresponding tissue water content of about 25%–60%. Inter-arm TDC ratios 1.45 and 1.30 for upper arm and forearm were used to differentiate a lymphedema patient and non-lymphedematous patient. 47
Bioimpedance spectroscopy (BIS)
Extracellular fluid in the arm was measured using a sweeping frequency bioelectrical impedance meter (model SFB7, Impedimed Ltd, Australia). All measurement procedures were fully in accord with the manufacturer's recommendations. Using several frequencies between 5 kHz and 1 MHz and Cole-Cole modeling, 48 the resistance at zero frequency R0, the indicator of arm ECF, was calculated.4,6,49,50 Prior to the application of surface electrodes all jewelry was removed and the skin was cleaned with an alcohol wipe. With the patient lying supine with arms along her side, the electrodes were positioned on the upper limbs using the equipotential principle, 51 in line with the ulna styloid and 5 cm distally, on the dorsum of the hands. One electrode was placed on the dorsal surface of the right foot over the third metatarsal bone. Both arms were measured in a similar manner and the resistance at zero frequency (R0) determined for each arm in order to express the result as R0 of contralateral arm/R0 of affected or at-risk arm (i.e., BIS R0 ratio). The BIS R0 threshold ratios of lymphedema 1.066 and 1.139 for nondominant and dominant arm were used. 6
Table 3 summarizes the technical features and differences between the practical measurements of the TDC and BIS methods.
Information on TDC and BIS from authors' experience, published articles and user instructions/recommendations or preferences.
Skin hydration creams may increase skin surface hydration (i.e., hydration of stratum corneum) if applied just before TDC measurement. Cream removal with alcohol wipe is then recommended. For skin water content measurement, stratum corneum hydration has a negligible influence.
Statistical calculations
Statistical calculations were conducted using SPSS (version 19.0.0.2, IBM, NY, USA) and Microsoft Excel (version 2010, Microsoft, WA, USA) software. Statistical significance in TDC (upper arm and forearm) and BIS R0 parameters between lymphedema and non-lymphedematous patients was tested with paired sample t-test. Significance of differences in arm ratios between TDC and BIS techniques was tested using a paired t-test. Difference in TDC (upper arm TDC and forearm TDC) and BIS R0 absolute values between affected or at-risk arm and contralateral arms in lymphedema and non-lymphedematous patients was tested using a paired t-test. In the four-field analysis comparing the TDC and BIS techniques in the diagnosis of LE, the correlations among parameters were performed using a χ2-test. A p-value <0.05 was considered significant.
Results
Thirty-eight patients (38.0%) had BCRL (Fig. 1). The sensitivity and specificity for the TDC method were 65.8% and 83.9% and for BIS method 42.1% and 93.5%, (p<0.001 and NS), respectively. In 25 TDC-detected skin lymphedema patients, 9 patients (36.0%) had increase of skin tissue water in upper arm, 6 (24.0%) in forearm, and 10 (40.0%) at both sites.
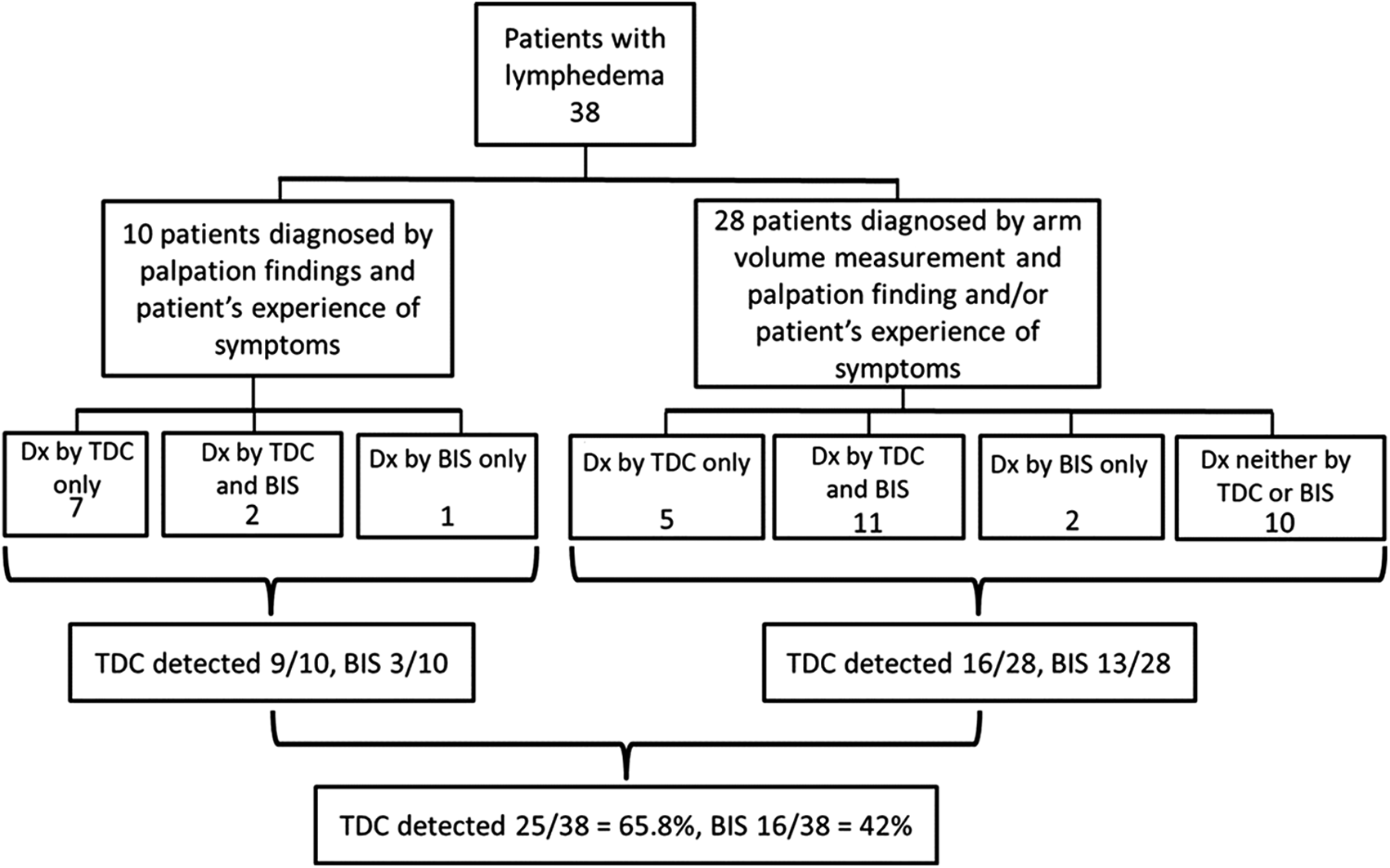
Technique-specific classification of the clinically diagnosed (Dx) patients with lymphedema. The patients were classified into different groups if the lymphedema threshold limits of each technique were exceeded.
In ten lymphedema patients who were diagnosed only by clinical criteria (Fig. 1) not supported by arm volume measurement, 9/10 (90.0%) had increase in skin tissue water via TDC and 3/10 (30.0%) in arm ECF via BIS. In non-lymphedematous group, 10/62 (16.1%) and 4/62 (6.4%) patients exceeded the TDC and BIS lymphedema threshold limits, respectively.
The 13/38 (34.2%) lymphedema patients whose skin tissue water was not increased had an increase of arm volume ratio (mean 7.3%, range 3.0%–12.3%). In 22/38 (57.9%) lymphedema patients whose arm ECF via BIS was not increased the arm volume ratio was increased (mean 7.5%, range 3.3%–11.1%).
In seven patients (7/38=18.4%) TDC was the only quantitative tool to assist lymphedema diagnosis but BIS only with one patient (1/38=2.6%).
Table 4 summarizes the TDC and BIS R0 absolute values for the lymphedema group and non-lymphedematous group of patients. In lymphedema patients, the upper arm and forearm TDC values were significantly greater than in contralateral arms (upper arm: 33.9±9.7 vs. 21.7±2.6, forearm 32.7±8.1 vs. 25.6±2.9, both p<0.001), while with the BIS technique the affected arm R0 values were significantly smaller than in contralateral arms (295.3±41.3 vs. 331.1±32.9, p<0.001). In non-lymphedematous group of patients the at-risk side upper arm and forearm TDC values were significantly higher than in contralateral arms (upper arm: 23.5±4.3 vs. 22.2±3.4, p=0.014; forearm: 27.0±4.4 vs. 25.8±3.7, p=0.03, respectively) while with the BIS technique the respective values were significantly smaller than in contralateral arms (327.3±33.8 vs. 335.7±34.3, p<0.001).
LE group: *TDC and BIS R0 values of affected arms were significantly greater than for contralateral arms (p<0.001). The upper arm TDC ratio was significantly greater than the forearm TDC ratio (p<0.001). The upper arm and forearm TDC ratios were significantly greater than the BIS R0 ratio (both p<0.001).
No LE group: **TDC values of upper arms and forearms were significantly greater than for contralateral arms (p=0.014 and 0.03, respectively), BIS R0 values were significantly smaller than contralateral arms (p<0.001).
Figure 2 illustrates the arm ratios of the WDM, BIS, and TDC techniques for affected or at-risk and contralateral arms of the lymphedema and non-lymphedematous patients. In six lymphedema patients, the increase of skin water content was more than 100% compared with the contralateral side. The upper arm TDC ratio 1.56±0.49 was significantly greater than forearm TDC ratio 1.28±0.33 (p<0.001) and the ratios were significantly greater than the BIS R0 ratio 1.12±0.12 (both p<0.001).

Affected or at-risk arm to contralateral arm ratios for each patient and as means±SD with different methods (arm volume, BIS, and TDC) in lymphedema (LE) and non-lymphedematous (Non LE) patients. The TDC ratios for upper arm and forearm in patients with LE were significantly greater than the respective ratios with arm volume and BIS R0 methods (both p<0.001). The arm ratios of various methods in non-lymphedematous patients were not statistically different.
Discussion
Observed prevalence of BCRL 38.0% within one year post-RT is in accordance with previous estimates of 33%–54% in patients with breast cancer surgery, axillary clearance, and related RT.1,52–54 Based on the technique-specific lymphedema threshold limits, the TDC technique detected 25 of 38 (65.8%) patients clinically diagnosed for lymphedema. Thirteen lymphedema patients who could not be diagnosed via TDC had a marked increase in arm volume (mean 7.3%). On the other hand, in 10/38 lymphedema patients whose arm volume was under the 5% lymphedema threshold limit, the TDC measurements indicated a marked superficial lymphedema with increased skin water content ranging from 21% to 126% (mean 62%). As discussed in the next section, these findings can easily be explained, if in the former case lymphedema was mainly deeply localized and in the latter case only superficially. These data then raise a question whether the TDC and arm volume method would work complementary. In the present material, the sensitivity of the combined TDC/arm volume technique increases to 97.4% with only one false-negative case among 38 lymphedema patients (Fig. 1). The complementary technique might then replace the semi-quantitative lymphedema criteria (palpation of subcutaneous thickness and a patient's experience of arm tension) with quantitative measures.
The BIS technique detected 16/38 (42.1%) patients clinically diagnosed for lymphedema illustrating a marked difference between the TDC and BIS methods. The lower sensitivity of the BIS method might partly be due to the present findings where lymphedema was manifesting only in the upper arm or forearm segment but the BIS technique is measuring whole arm ECF space. Second, as discussed in the next section, the sensitivity is lowered if the BIS technique is measuring mainly deeply localized lymphedema, although lymphedema might only be superficial. If the previously presented TDC/arm volume complementary principle is applied with the combined BIS/arm volume lymphedema detection, the sensitivity of the BIS method would increase from 42.1% to 81.5% and the number of false-negative cases would decrease from 58.0% to 18.4%. The number of false-negative patients is still high but slightly better than 27.0% when diagnostic accuracy of the BIS and arm volume by a Perometer technique was compared. 55
Diagnostic power between TDC and BIS techniques
Since the diagnostic power of a specific technique is dependent upon the selected inter-arm threshold ratio and threshold criteria (mean+2SD or mean+3SD determined from a healthy population), the sensitivity and specificity based on conservative and revised BIS threshold limits6,56 were calculated and compared with those obtained with the TDC threshold criteria. Table 5 illustrates that the selection of 2SD criteria increased sensitivity of all techniques compared with 3SD criteria. Simultaneously, the specificity decreased with 2SD criteria. While specificity of the revised BIS 3SD criteria was better than with conservative 3SD criteria (100% vs. 93.5%), sensitivities were poor in both cases, 42.1% vs. 36.8%. These results support the conclusions that the TDC skin water measurements were best aiding the diagnosis of early lymphedema and early swelling detected in the first measurement visit within one year post-treatment may occur only in skin but also at deeper structures. The situation may be different when pretreatment data is available and patients are in a regular follow-up.
The two techniques compared in the present study are sampling different tissue compartments that may complicate the comparison of the current results. Recently, segmental and spot bioimpedance measurements have become available for the assessment of BCRL57–59 and thus, it would be valuable to compare such measurements with highly-localized TDC measurements. However, currently there is no scientific evidence whether the diagnostic power of these local/loco-regional BIS measurements would be better than that of the conventional and widely used BIS technique. Thus, comparison of the diagnostic power of TDC and conventional BIS techniques, both proposed for early detection of BCRL, might be more relevant than evaluating the performance of segmental/spot BIS measurements.
Although sensitivity and specificity are dependent on the selected thresholds limits and 2SD or 3SD criteria, they are also dependent on clinical diagnostic criteria applied in different studies. In the present study, the diagnosis was based on three criteria, while in previous BIS studies the diagnosis of lymphedema was mainly based on single BIS-specific criteria. 56 If the BIS technique is essentially a volume measurement technique, 55 all patients with lymphedema cannot necessarily be diagnosed by single BIS threshold criteria.
Figure 1 illustrates that 10 of 38 lymphedema patients were diagnosed for lymphedema even their affected arm volume (<5%) was not indicative for lymphedema. In the present investigation we have adopted the arm volume measurement, palpation of skin and subcutis in the medial and lateral elbow region, and a patient's symptom of arm heaviness for the basis when diagnosing early lymphedema (i.e., the authors follow the Stanton et al. recommendation on multiple criteria in predicting early, mild lymphedema). According to Stanton et al., 41 “arm volume is of little value in diagnosing early, mild BCRL, and reliance on comparison of arm volumes or circumferences will cause an underestimation of the prevalence of BCRL” and “edema can be limited to certain region, e.g., hand and wrist only, or upper arm.” The co-author of the manuscript (KJ) has found that using this diagnostic approach BCRL can be identified at an early stage and edema volume kept at a low level for at least 10 years. 1
Localization of arm skin lymphedema
The TDC ratio in lymphedema patients in the affected arm with respect to the contralateral arm was significantly greater in upper arm 1.56±0.49 than in forearm 1.28±0.33 (representing edema of 56% and 28%, respectively) (Fig. 2). The observation of the greater edema in upper arm skin might be related to dermal backflow when due to axillary blockage subfascial lymph flow is redirecting back to epifascial lymphatics, 60 resulting in an increase of tissue water in skin.
Non-lymphedematous patients exceeding technique-specific lymphedema threshold limit
The TDC ratio in the non-lymphedematous 62 patients indicated that 10 patients (16.1%) had an increase of tissue water in skin. In 5 of these patients, a TDC ratio was supporting lymphedema only in the upper arm, while in another 5 patients only in the forearm, respectively. Increase of arm volume or ECF fluid was found by the WDM or BIS methods in 5/62 (8.1%) and 4/62 (6.4%) of patients. The follow-up of these patients will show whether the patients were at-risk to develop lymphedema.
Origin of physiological information between the TDC and BIS techniques
The BIS technique is described as measuring extracellular fluid at the applied low kHz to 1 MHz frequencies.2–6,49,51,55 The BIS technique is essentially a volumetric technique providing a measurement index that is highly correlating with Perometer-measured increase of lymphedematous arm volume in patients with confirmed arm lymphedema, 55 but whether such a correlation exists with early lymphedema has not been reported.
The data at each frequency are used in a Cole-Cole model
48
from which the resistance R0 at zero frequency is calculated. R0 is a model-based value for arm extracellular fluid that is calculated since the resistance of the arm at direct current (i.e., at zero frequency) cannot be measured. R0 is a composite resistance that includes all arm tissue components and as far as the authors know there is no scientific evidence available on the relative contributions of the individual components to R0. However, since arm tissues at low kHz to hundreds of kHz are essentially resistive, an arm segment can well be approximated by five parallel tissue components consisting of skin, subcutis, muscle, bone and blood for constant current BIS devices (Fig. 3a,b). The resistances of the components can be calculated in the following way. Assume the arm segment has a length L and volume V. Thus V, the volume of the segment is given by V=L×A, where A is the arm cross-section consisting of each tissue component Ai expressed as
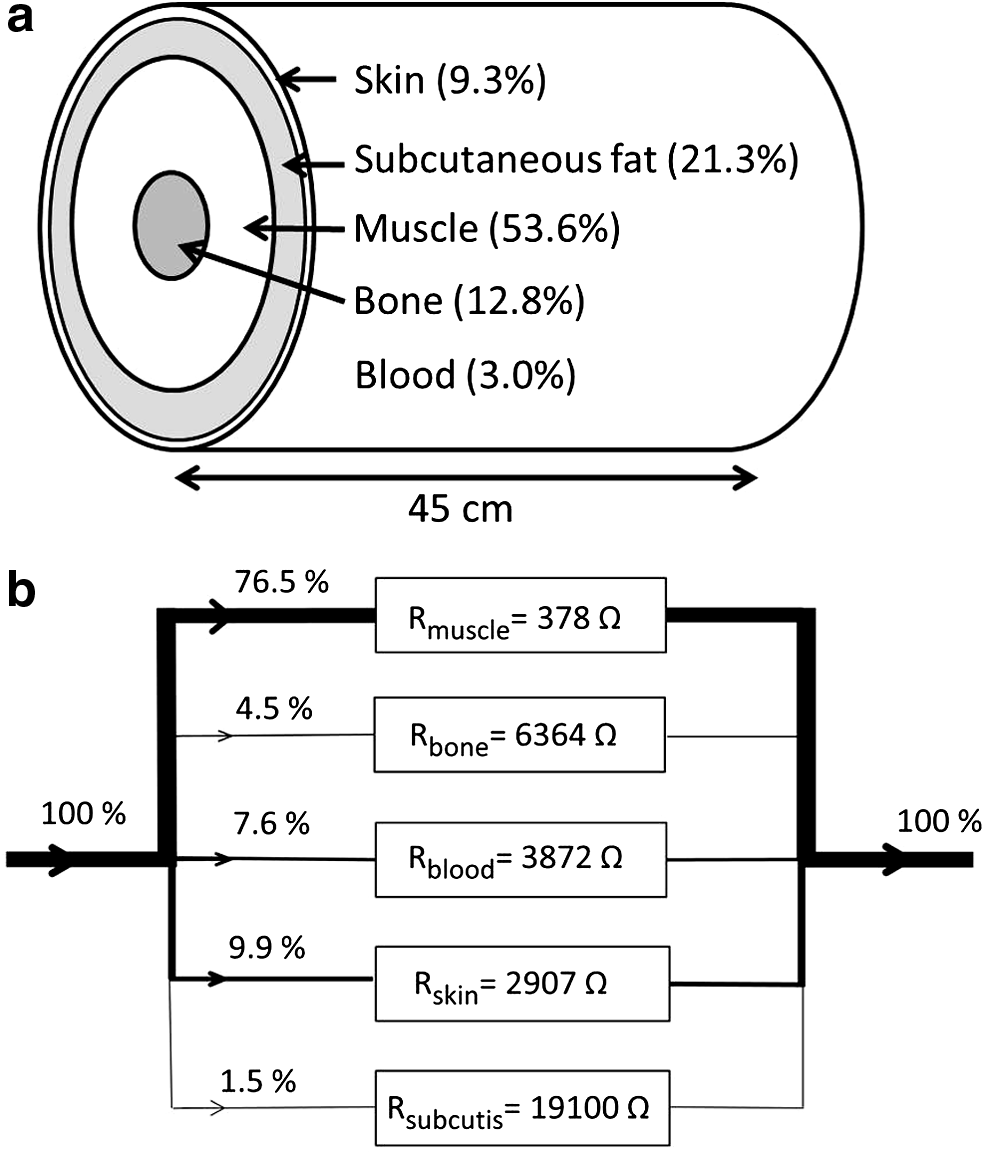
Five-component resistive model for the arm (length L=45 cm) describing
Since the resistance of each component Ri can be expressed as
only the surface areas Ai and conductivities σi of different tissue components are needed to calculate the resistance of each component. To obtain approximate values we can calculate the resistance of an average arm assuming it is with a 45 cm length and with a diameter of 8.4 cm. For skin, subcutaneous fat and bone components the average cross-sectional areas can be calculated from the published data22,61 (Table 6).
Estimated fractional blood volume.
Diameter of mid-humerus 25 mm, radius and ulna together approximated to have the same diameter 25 mm. Since distal and proximal ends are larger, a diameter of ‘average arm bone’ 30 mm was selected.
Muscle layer between fat and bone, calculated by subtracting skin, subcutaneous fat, blood, and bone cross-sectional areas from arm cross-sectional area.
Blood cross-sectional area was estimated by average fractional blood volume data for major arm tissue components to 3%.62,63 The muscle area was calculated by subtracting from the arm total cross-sectional area the surface areas of skin, fat, bone, and blood. Average conductivity values for skin, fat, bone, and blood and a longitudinal conductivity for muscle from kHz to hundreds of kHz were used 64 (Table 6).
Figure 3b illustrates that the muscle component has the lowest resistance while subcutaneous fat with low conductivity has the highest resistance. The calculated total arm resistance that includes all of the parallel components in the model is R=289 Ω. This value is of the same order as the typical resistance values R0 (290–360 Ω) obtained by the BIS technique in this study and with Cole-Cole modeling.4,6,56 Based on the resistance values of the each tissue component it can be calculated that 76.5% of the total electric current flows through the muscle component and 9.9, 1.5, 4.5, and 7.6% through skin, subcutis, bone, and blood components, respectively. According to model calculations for an increase of 20% in skin tissue water, the total resistance changes less than 2.5%. This indicates that such a 20% change in skin water would be essentially undetectable with multi-frequency BIS analyzers that have a reported accuracy of ±3% for resistance R0. 65
Using the same model it can be shown that for an increase of 20% in skin tissue water the arm volume changes less than 2% (i.e., such a 20% change in skin water volume is practically undetectable by arm volume measurement). Calculations based on this simple, but representative model, suggests that the main route of electric current in the BIS technique is through the well-conducting (subfascial) muscle component that is largely spared of swelling and to a lesser amount through the skin where early lymphedema is thought to manifest.20,21,66 The simulations also demonstrate that arm volume measurement is not sensitive to assess lymphedema in skin. Thus measurements of skin changes would seem to be indicated.
Technical differences between TDC and BIS methods in the assessment of lymphedema
Technical basis underlying the TDC and BIS techniques is different. In the TDC technique, a very high frequency EM field of 300 MHz is induced locally into the skin. This selection enables the measurement of the major components of extracellular water (i.e., free water and bound water attached on the surface of macromolecules with equal access until to the effective depth of 2.5 mm).18,45 Although intracellular fluid (ICF) space is also measured the size of ICF, localizing mainly to thin epidermis, is small compared with ECF space of the skin. Therefore, the TDC technique reflects changes of interstitial fluid space in skin.
In the BIS technique of applying several low kHz to 1 MHz frequencies, the contributions of free and bound water in the measured conductivity have not been investigated but at higher frequencies (>10 MHz) the free water component may dominate the ECF measurement due to higher conductivity of free than bound water component. 35 Since in skin, up to 50%–90% of the skin tissue water is considered bound,24,37,67,68 it has not been shown whether the BIS technique has equal access to both tissue water components of the extracellular fluid space.
Conclusions
In the TDC technique, localized tissue water in skin where early swelling in lymphedema is thought to exist was measured. The TDC skin water measurements were best aiding the diagnosis and localization of early lymphedema and also detected a number of non-lymphedematous patients potentially at risk for later occurrence of lymphedema. The present results, without pretreatment data available, support the view that early swelling detected in the first measurement visit within one year post-treatment may occur only in skin but also at deeper structures. The situation may be different when pretreatment data are available and patients are in a regular follow-up. Arm volume measurements are an important supplement when the TDC measurement cannot characterize lymphedema superficially. The results thus support the complementary role of TDC and arm volume measurements as a highly diagnostic method for lymphedema.
Results from the BIS technique were not correlating well with TDC technique in the assessment of patients with or without lymphedema. This is due to differences in the physiological basis of measurement information, but also in the technical and electrical solutions between the TDC and BIS methods. Five-component resistive arm model suggested that subfascial muscle component dominates the results of the BIS technique since the muscle component has the lowest resistance of arm tissues.
Footnotes
Author Disclosure Statement
During the research (years 2013–2014) the authors had no financial conflicts of interest. From January 2015, T. Lahtinen has acted as a research and development manager to Delfin Technologies Ltd.