
Abstract
Background:
Acute dermatolymphangioadenitis (ADLA) is a risk factor for increasing of edema and worsening severity. Reducing ADLA frequency is an important objective of lymphedema management because ADLA episodes are strongly associated with poor quality of life. Lymphedema changes dermal and subcutaneous structure, favoring ADLA; ADLA recurrence may be caused by structural change of the dermis. However, the structure of the skin following ADLA episodes has not been studied in depth. The aim of this study was to examine changes in the skin after episodes of ADLA in breast cancer-related lymphedema (BCRL) using histogram analysis of ultrasonography findings.
Methods and Results:
This was a case-control study with matching for the duration of lymphedema. We compared 10 limbs (5 BCRL patients, Cases) with a history of ADLA and 14 limbs (7 BCRL patients, Controls) without. Ultrasonography was performed using a 20-MHz probe, and measurements were made at a site 10 cm proximal to the ulnar styloid process. We compared “skewness” of the images in the dermis from the histogram analysis. This study was approved by the Ethics Committee of Kanazawa University. Skewness was significantly different between the affected and unaffected limbs (p = 0.02). Cases showed a positive value (median 0.74, range −0.18 to 1.26), whereas Controls showed a negative value (median −0.21, range −0.45 to 0.31).
Conclusions:
Episodes of ADLA changed the distribution of echogenicity on imaging, which indicates a change in the collagen fibers in the dermis. These findings might contribute to improving the management of lymphedema and prevention of recurrent ADLA.
Introduction
A
Reducing ADLA frequency is an important objective of lymphedema management because ADLA episodes are strongly associated with poor quality of life.7,8 The British Lymphology Society reported that the management of ADLA during an acute attack in the setting of lymphedema involves initiation of antibiotics according to local guidelines and avoiding the use of compression garments until after inflammation resolves. 9 After the inflammation resolves following an acute episode of ADLA, patients are instructed to restart basic lymphedema management that was being done before the ADLA episode. In a previous study, basic lymphedema management including combined physical therapy 10 that involves skin care, lymph drainage, bandaging, and exercise was found to be feasible and effective for reducing the number of ADLA attacks per year.11,12
However, after the inflammation resolves following an ADLA episode, the details of basic lymphedema management, special techniques, and/or pressure and/or frequency of methods have not been identified, because the dermal change has not been described. After resolution of an acute episode, the dermal structure changes during the phases of tissue healing. Addiss et al. reported that the mean duration of ADLA attacks was 2.6 days (range 1–44 days), 11 and others reported similar results. 12 After the inflammatory phase, the wound enters the proliferative phase.13,14 The proliferative phase is essentially the generation of repair material that is involved in the production of scar tissue.
The production of type III collagen, which commences after 2–3 days, reaches a peak at 2–3 weeks post-injury.13,14 One fundamental process is fibroplasia, which is the formation of collagen. Collagen maturation and remodeling start approximately 2–3 weeks after injury. The tensile strength of the tissue improves because of formation of intra- and extramolecular cross-linkages between the collagen fibers. 15 Therefore, the dermal structure, particularly the distribution of collagen fibers, is changed in patients who have had ADLA episodes.
The dermal structure can be seen by ultrasonography.16–18 Using a 20-MHz probe, it has been shown that both skin thickness 16 and the number of low echogenicity pixels (LEP)17,18 are increased in affected limbs. Changes in the imaging findings due to fluid accumulation in the skin have been reported. However, collagen distribution in the dermis of patients with a history of ADLA episodes is altered. Collagen distribution cannot be evaluated by measuring thickness and LEP. Therefore, we focused on histogram analysis, in which the asymmetric distribution of echogenicity of ultrasound imaging is examined. 19
The purpose of the present study was to identify changes in the dermis due to episodes of ADLA in breast cancer-related lymphedema using ultrasonography.
Materials and Methods
Study design and setting
This study was a case-control study that was performed from June 2012 to March 2014 in two lymphedema clinics in Japan. In these clinics, there were physicians specializing in lymphedema, and nurses who had experience of more than 5 years in lymphedema management.
Participants and ethics
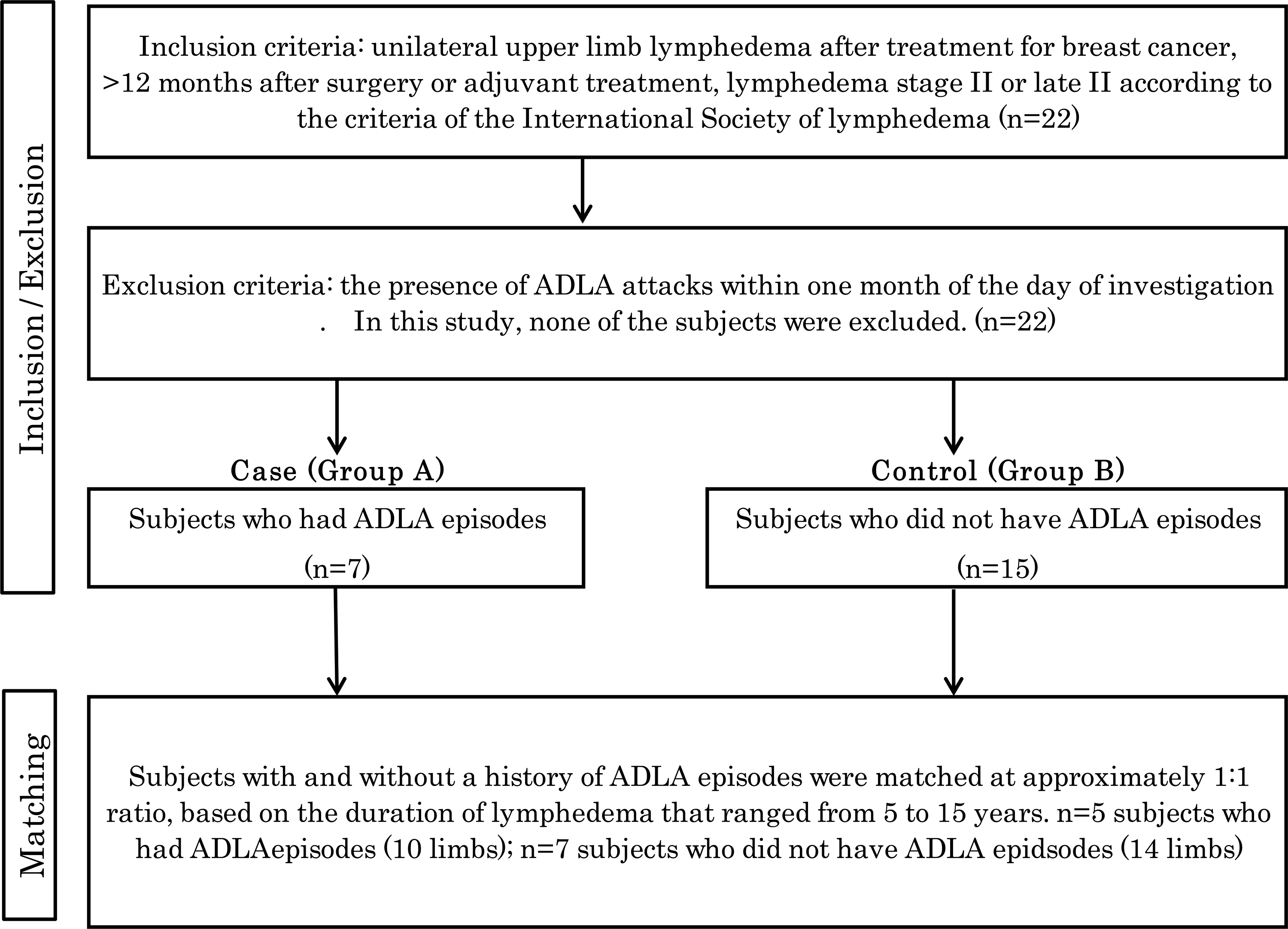
Subjects with unilateral upper limb lymphedema after treatment for breast cancer, classified as either stage II or late stage II according to the criteria of the International Society of Lymphedema, 10 were eligible for the study. The exclusion criterion was the presence of ADLA attacks within 1 month of the day of investigation. Patients were identified and recruited by physicians who specialized in lymphedema.
The sample size of about thirty patients was calculated with an effect size of 0.5, α error of 0.05, and a power of 0.8. The number of patients was based on feasibility rather than any formal statistical technique.
Measurements
Both limbs underwent edema evaluation and ultrasound imaging. Outcomes were then assessed by a researcher. The extent of edema and the ultrasonography results were analyzed. The investigator marked the site of examination at 10 cm proximal to the ulnar styloid process for both the affected and unaffected arms.
Ultrasonography images
Images of the dermis were recorded using a Derma scan C ultrasound system (Cortex Technology, Smedevaenget, Denmark) at 20 MHz. Ultrasound gel was applied liberally to the skin, and the probe was placed longitudinally on the arm. Field size was set to a width of 13.42 mm and a depth of 22.40 mm. A two-dimensional image of the skin was produced and recorded by the computer and viewed in color. Gain was adjusted as necessary to optimize image quality and boundary definition. To help minimize the effect of noise on measurement, the image was convolved with a 9-point low-pass filter. 20
We determined the quantitative parameters through qualitative assessment. We then calculated skewness from the histogram analysis in the region of interest (ROI) that was set in the images of the dermis, using the same technique for both limbs. Measurements were performed each day between 13:00 and 16:00, while the patient sat in a chair with the arm supported in abduction. The researcher supervised the assessment and analysis of ultrasound images by a physician who specialized in lymphedema.
Edema evaluation
These data included differences in circumference and skin hardness. The principal researcher measured the arm circumference using a tape measure at 10 cm below the elbow. Skin hardness was assessed by each patient using a 10-cm visual analog scale, with 0 cm representing “soft,” 5 cm representing “same hardness as the unaffected limb,” and 10 cm representing “hard.”
Analysis
The characteristics and edema evaluations of patients with a history of ADLA episodes (Cases) and Controls without a history of ADLA episodes were compared.
The degree of skewness of the histogram is a measure of symmetry, or more precisely, the lack of symmetry. A distribution is symmetrical if it looks the same to the left and right of the center point. The histogram is an effective graphical technique for showing the skewness of a data set. The formula for skewness
19
is:
where n = pixel number in the ROI; xi = intensity of pixels (0–255); and
The skewness for a normal distribution is zero, and symmetrical data should have skewness near zero. Negative values for skewness indicate data that are skewed to the left, and positive values for skewness indicate data that are skewed to the right. These data were analyzed by ImageJ analysis software (v1.42q, National Institutes of Health).
We calculated the skewness of the histograms for both limbs.
Statistical analysis
All data are presented as medians and range. The Wilcoxon rank-sum test was used to test the significance of differences, and p values <0.05 were considered significant. JMP® statistical software (SAS Institute, Cary, NC, USA) was used for all calculations.
Results
Participants
A total of 22 patients were initially recruited: 7 with and 15 without a history of ADLA. Subjects with and without a history of ADLA episodes were matched at an approximately 1:1 ratio, based on the duration of lymphedema, which ranged from 5 to 15 years. Finally, 5 Cases and 7 Controls were analyzed (Fig. 1).
Study subjects were selected based on whether they were diagnosed with stage II or late stage II lymphedema between June 2012 and March 2014.
Characteristics and edema evaluations
Groups A and B showed no significant differences in age, body mass index (BMI), duration of lymphedema, circumference, and skin hardness (Table 1).
The Wilcoxon rank-sum was used to test the statistical significance of differences for all variables.
Skewness on histogram analysis
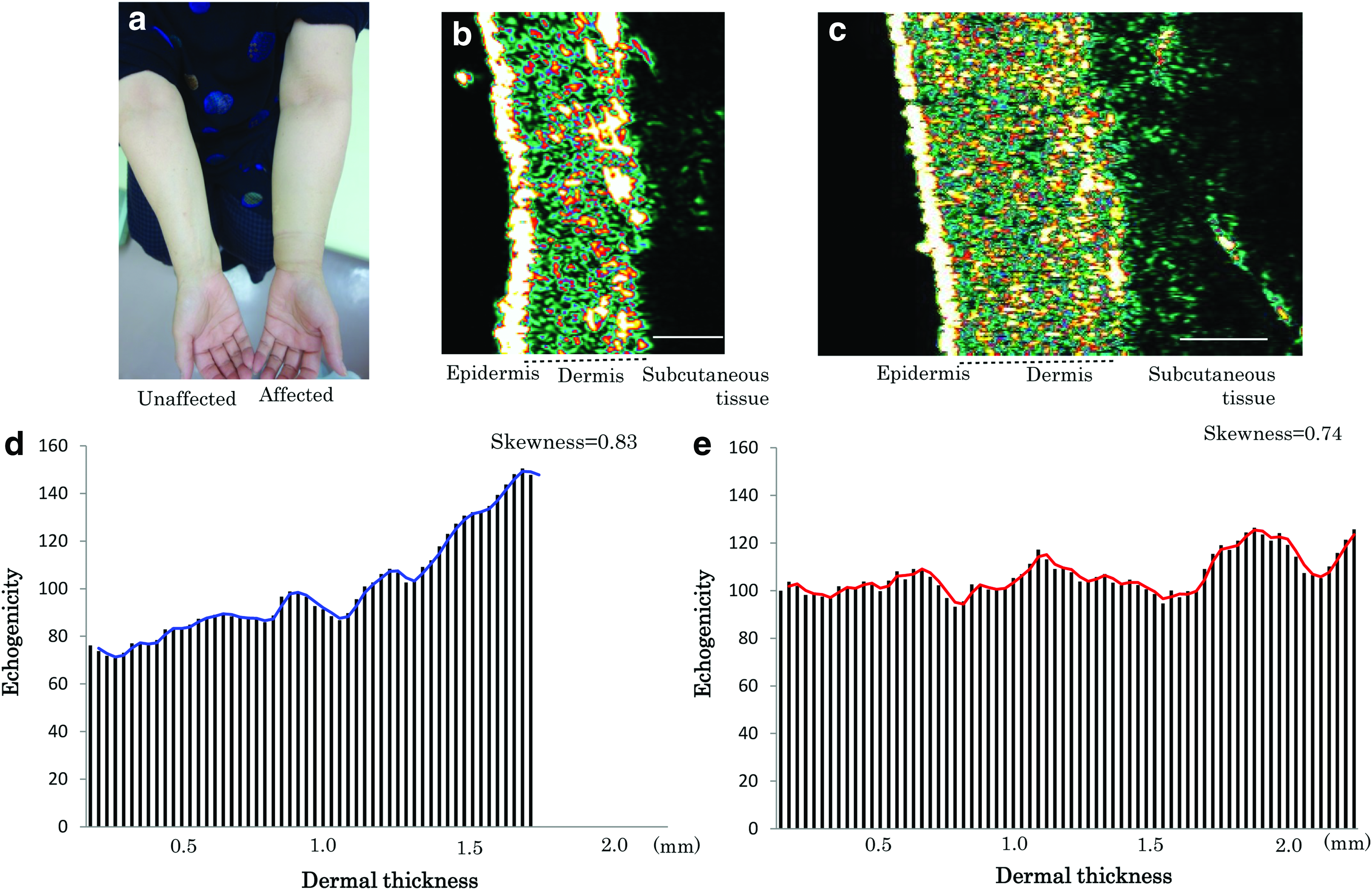
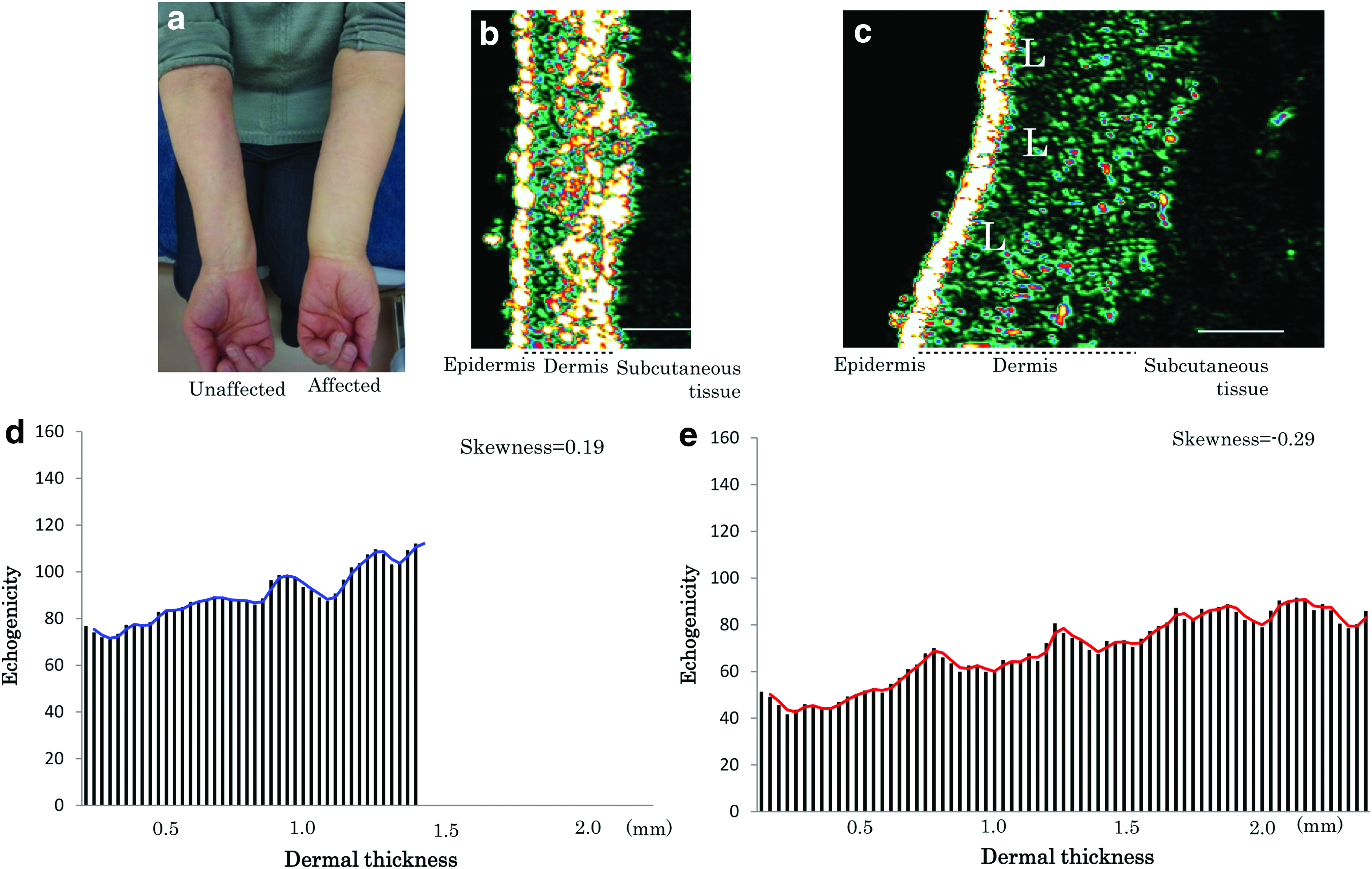
The distribution of echogenicity on ultrasound images differed between the groups (Figs. 2 and 3). Skewness in the affected limb was significantly different between the Cases and Controls (p = 0.02). Cases showed a positive value (median 0.74, range −0.18 to 1.26), whereas Controls showed a negative value (median −0.21, range −0.45 to 0.31) (Table 2).
A representative case of a 62-year-old woman with a history of ADLA.
A representative Control case of a 62-year-old woman
The Wilcoxon rank-sum was used to test the statistical significance of differences for all variables. For the affected limb, skewness was significantly different between Cases and Controls (*p < 0.05).
Discussion and Conclusions
This study is the first to report changes in the dermis after episodes of ADLA in breast cancer-related lymphedema using histogram analysis of high-frequency ultrasonography. Skewness histogram analysis of the affected limb was significantly different between those with a history of ADLA episodes and those without. Adjustment was made for the period of lymphedema because it may affect collagen quantitatively, and the duration of lymphedema was matched.
In this study, high-frequency ultrasonography and skewness histogram analysis were used to focus on the dermal structure and distribution of echogenicity. Previously, some studies identified particular aspects of lymphedema on ultrasonography.16–18,21–24 The affected limbs have shown increases in both skin thickness 16 and the number of LEP17,18 using a 20-MHz probe. Subcutaneous tissue has shown a cobblestone appearance and thickening on imaging at 7.5–10 MHz.16,17,21–24 Such studies have revealed the characteristics of skin and subcutaneous tissue showing lymphedema, but collagen distribution in the dermis cannot be evaluated by these parameters.
This study indicated that the distribution of collagen in the papillary layer of the dermis was different after ADLA episodes based on the results of skewness and high echogenicity pixels. The skewness data of patients with a history of ADLA episodes showed positive numbers, whereas patients without a history of ADLA showed negative numbers. Positive skewness means that the left tail is long. The results of skewness indicate a difference in skin structure. In particular, high echogenicity pixels indicate the presence of collagen fibers; 25 therefore, their existence indicated the presence of collagen in the upper area of the dermis, which might be the papillary layer in patients who had ADLA. We think that this is related to post-inflammation collagen maturation and remodeling that was initiated as part of the inflammation process.
The present findings have implications for the management of lymphedema in patients with previous episodes of ADLA. In the clinical setting, we suggest using ultrasonography to assess skewness and confirm dermal structure. It is then important to change the conditions of basic lymphedema management in the setting of ADLA, for example, application of pressure, frequency, and special techniques. However, the details of these methods need more study.
This study has several limitations. First, imaging and histological findings were not compared. The changes in the distribution of echogenicity pixels and in collagen fibers in the skin were inferred, but the actual relationship between high echogenicity pixels and collagen fibers could not be determined. Second, because of feasibility, further data cannot be collected. Thus, the sample size was small. However, it was possible to compare skewness between cases and controls. Third, since one single site of ultrasound imaging was chosen, this could have limited the significance of the resulting findings. In fact, ADLA may affect different areas. Nevertheless, there was a significant difference. Given this result, in the next investigation, at least three or four sites will be assessed to achieve a more comprehensive assessment. Despite these limitations, the present results suggest that the dermal structure of limbs affected by episodes of ADLA differs from that of limbs without episodes of ADLA.
In conclusion, episodes of ADLA changed the distribution of echogenicity on imaging. This indicates a change in the collagen fibers in the skin. The results of this study will be useful in the management of lymphedema in patients with a history of ADLA, as well as in the prevention of recurrence of ADLA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.