
Abstract
Abstract
Objective:
To investigate the ultrasonic effects of progressive resistance exercise (PRE) for the treatment of patients with breast cancer-related lymphedema (BCRL).
Subjects and Method:
The 32 patients with diagnosed BCRL were randomly divided into two groups: the PRE group and the non-PRE group. After complex decongestive physiotherapy, PRE was performed by 0.5 kg dumbbell while wearing a compression stocking or a multilayer bandage to avoid aggravation of the lymphedema in the shoulder and arm. In the first week, the PRE group performed five repetitions of each exercise, twice a day, and the exercise were increased to five repetitions every week during 8 weeks. The thickness of muscle and subcutaneous tissue and circumferences of proximal and distal upper limbs were measured at baseline, 4 weeks, and 8 weeks. Examiners measured the circumference of upper limbs with tape measure, then the thickness of the muscle and subcutaneous tissue were measured by ultrasonography.
Results:
Muscle thickness of the upper limbs was less in the affected limb than that of the nonaffected limb at pretreatment. The thickness of subcutaneous tissue and circumferences of the arm was more decreased in the PRE group than that of the non-PRE group. The thickness of muscle of the arm was more significantly increased in the PRE group than that of the non-PRE group (p < 0.05).
Conclusion:
For the treatment of patients with BCRL, PRE with complex decongestive physiotherapy did not cause additional swelling, and it reduced arm circumference by decreased subcutaneous tissue thickness and increased muscle thickness.
Introduction
L
Individual studies report arm lymphedema in up to 94% of patients with breast cancer, 4 with the wide variation (as low as 0%) in reported results of differences in study design, diagnostic methods, and criteria used, and timing of lymphedema measurement with respect to breast cancer diagnosis and treatment.5,6 It has been estimated that the incidence of arm lymphedema will be about 20% after breast cancer. This estimation is the average incidence of studies that have been included in several systematic reviews of lymphedema after breast cancer.7–9
Lymphedema can cause limitations in range of motion, pain, weakness, or stiffness in the affected arm.10–12 It also results in psychological problems, including anxiety, depression, sexual dysfunction, social avoidance, and exacerbation of existing psychiatric illness. 13
The treatments for lymphedema are physical therapy, medication, and surgery, but complex decongestive physical therapy (CDPT) is the most commonly used treatment.14–16 Remedial exercise, stretching, aerobic exercise, and resistive exercise are used as treatments for lymphedema. Remedial exercise is recognized as a standard treatment during the first and second phases of CDPT. Yet only a few studies have shown that resistance exercise reduces the volume of lymphedema, and does not aggravate lymphedema.14,17
Recent studies have reported that the severity of lymphedema is more associated with the subfascial lymphatic system than with the epifascial lymphatic system.14,18 These studies have shown that functional improvement in the subfascial lymphatic system may be very important for the treatment of lymphedema.
However, a realistic protocol of resistive exercise for lymphedema patients has not been established yet. We hypothesized that functional improvement in the subfascial lymphatic system is related to muscle strength gained via progressive resistance exercise (PRE), and this may reduce lymphedema volume. This study was designed to identify the therapeutic effects of PRE along with conventional therapy by ultrasonography in patients with BCRL.
Materials and Methods
Subjects
The patients (N = 32) were consecutively selected by a physician from the outpatient clinic of the Department of Rehabilitation Medicine of Chungnam National University Hospital, Korea. Recruitment to this study occurred from July 2013 to October 2013. Informed consent was obtained from all participants prior to the study. Prior to participation, all procedures were explained to each subject, and informed consent was obtained, as approved by the Institutional Review Board at Chungnam National University Hospital and with the Helsinki Declaration of 1975. The rights of the subjects were protected.
The criteria of diagnosed BCRL in breast cancer survivors were (1) patients who had a greater than 2-cm circumference difference between the affected arm and the normal arm, and (2) patients who had lymphedema diagnosed via lymphoscintigraphy (delayed or obstruction of lymphatic flow compared with the unaffected side, dermal backflow, poor to no visualization of the collateral and main lymphatics, and decreased or no clearance of radioisotope from the injection site). 19
The exclusion criteria of our study included (1) history of primary lymphedema; (2) patients who had lymphedema in both arms; (3) patients with a body mass index (BMI) greater than 35 kg/m2; (4) the need of concurrent anticancer chemotherapy; (5) patients who had cancer recurrence within 6 months from the time of entering this study; (6) patients who had vascular disease; (7) patients who had any neurologic signs, such as decreased motor power, sensory changes, or decreased deep tendon reflexes; and (8) patients who could not communicate. Characteristics of the participants are described in Table 1.
Values are presented as mean (standard deviation) or number.
BMI, body mass index.
Methods
Thirty-two patients were randomly divided into a PRE and a non-PRE group. The PRE group received conventional therapy together with PRE, and the non-PRE group received conventional therapy without PRE. The conventional therapy consisted of manual lymphatic drainage, non-elastic bandage compression therapy, and skin care. It was performed by a trained physical therapist for 1 hour a day, 5 days a week. The manual drainage was performed at trunk to distal upper extremity toward lymphatic flow with light skin massage, it was not stroking. Non-elastic bandages were applied and changed daily. All patients were also educated on appropriate skin care, such as avoiding extreme heat, proper skin hygiene, avoiding trauma, and applying moisturizer daily. Both groups were wearing a compression stocking or a multilayer bandage to avoid aggravation of the lymphedema in the shoulder and arm.
Each participant was informed about the study and provided written informed consent.
Progressive resistance exercise
The exercise group performed a series of exercises using a 0.5-kg dumbbell. Participants continued to wear a compression stocking or a multilayer bandage during PRE. The prescribed exercises included (1) dumbbell fly, (2) triceps extension, (3) one-arm bent-over row, (4) biceps curl, (5) dumbbell side raise, and (6) lifting the arms forward (Fig. 1). This procedure was repeated five times twice a day. Every week, the number of repetitions was increased by adding five additional repetitions. The exercise was performed, and the progress was recorded over a total of 8 weeks.
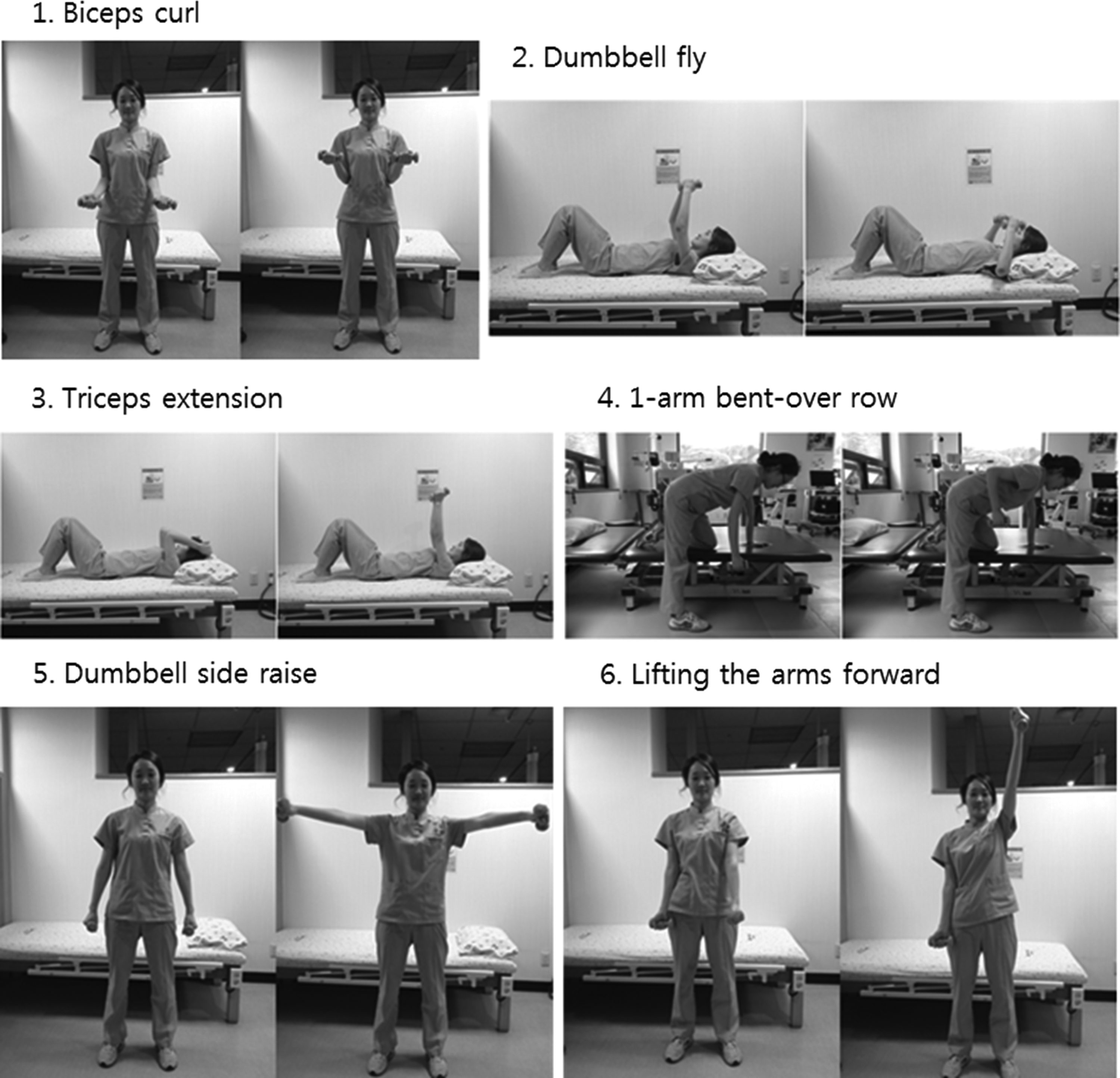
Progressive resistive exercise.
Patients were evaluated at the baseline, 4 weeks, and 8 weeks. (Fig. 2). To ensure that the patient followed the appropriate protocol, each patient was provided with a personalized checklist including images of the exercise. Compliance to the protocol was checked by unexpectedly calling the patient at weeks 2, 4, and 6.
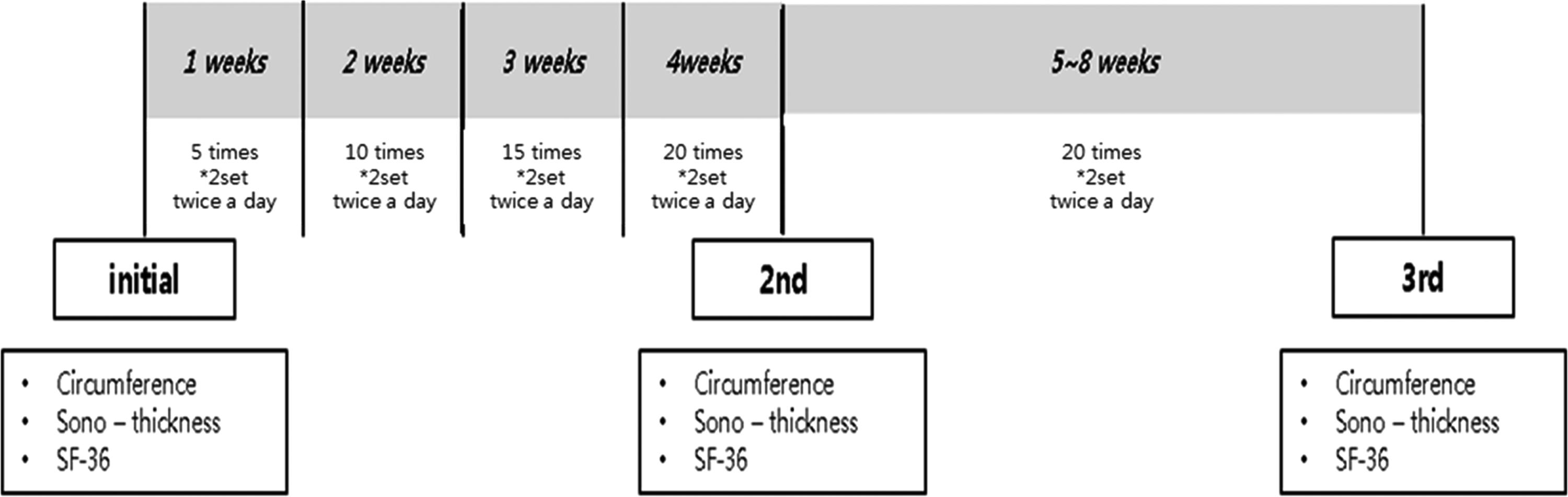
Protocol of progressive resistive exercise.
Main outcome measures
Measurements of all participants at baseline, 4 weeks, and 8 weeks were completed by a physician using standardized methods. Physician was blinded to treatment allocation. Participants were reminded to not reveal their group assignment before measurement and evaluation sessions.
In both affected and unaffected upper extremities, circumference, subcutaneous thickness, and muscle thickness were measured at two points. The two points were defined as follows: 1) proximal part, 10 cm proximal to the elbow point along the line of the humerus and the bicipital groove between the mid-point of the medial and lateral epicondyles; and 2) distal part, 10 cm distal to the elbow point along the line of the radial and ulnar styloid processes between the mid-point of the medial and lateral epicondyles. 20 Upper limb circumference was measured using a tape measure; the thickness of the subcutaneous tissue and muscle were measured using ultrasonography (MyLab™50, Esaote, Italy).
A skilled sonographer measured the thickness of the subcutaneous tissue and muscle of the upper limb. With the patient lying comfortably, the ultrasound probe was placed perpendicular to the upper limb ventral axis. Sufficient gel was applied to ensure that no pressure was exerted over the arm during measurements. Muscle thickness is defined as the distance from the highest point of the boundary of the bone to the highest point of the boundary portion of the fascia. The thickness of the subcutaneous tissue was defined as the distance from the skin to the fascia (Fig. 3).

The thickness of muscle and subcutaneous tissue of the upper limbs M, thickness of muscle; SC, thickness of subcutaneous tissue.
Statistical analysis
Statistical analyses were performed using SPSS 12.0. Statistical significance for the differences between both arms was tested using a paired t-test. Changes in the subcutaneous tissue and muscle thickness, and upper limb circumference were analyzed using repeated-measures ANOVA. Statistical significance level was set at the p value of 0.05 or less.
Results
Subjects categorized into the PRE were 45.4 years old and the non-PRE group were 53.3 years on average. Average BMI was 22.6 and 24.97, respectively. All patients received axillary lymph node dissection with mastectomy. The average time elapsed between surgery and the initiation of treatment for edema removal was 17 and 18 months, respectively (Table 1).
Initial muscle thickness of all participants measured by ultrasonography significantly decreased at affected arm compared to unaffected arm in baseline measurement (Table 2).
Values are presented as mean (standard deviation); *p < 0.05, according to paired t-test.
Upper limb circumference in the PRE group did not significantly change after 4 weeks of exercises; however, both distal and proximal circumferences showed a significant reduction after 8 weeks. These parameters did not significantly change in the non-PRE group (Fig. 4).
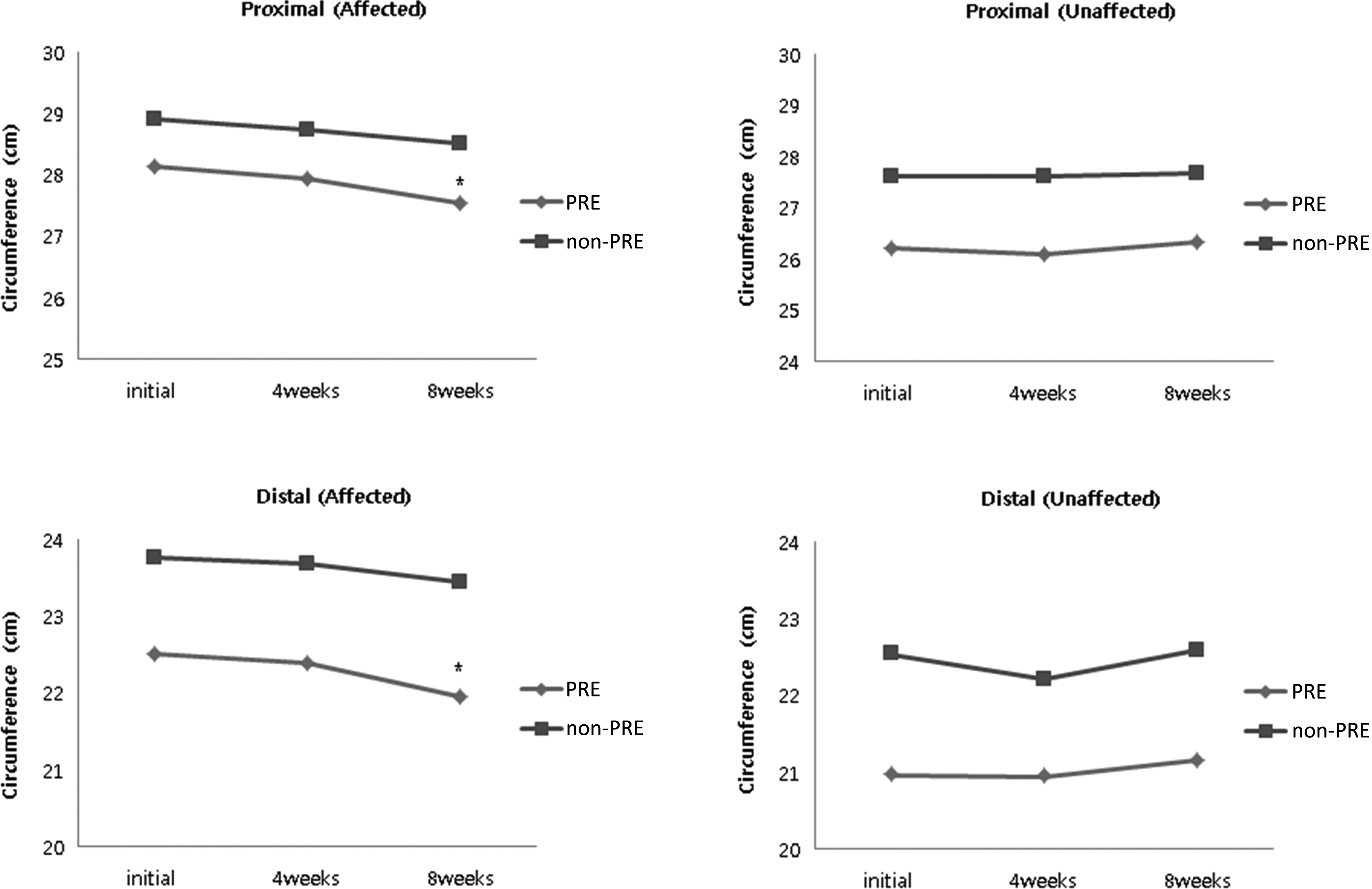
The circumferences of affected limb and unaffected limb by tape measurement. *p < 0.05 by repeated-measures ANOVA.
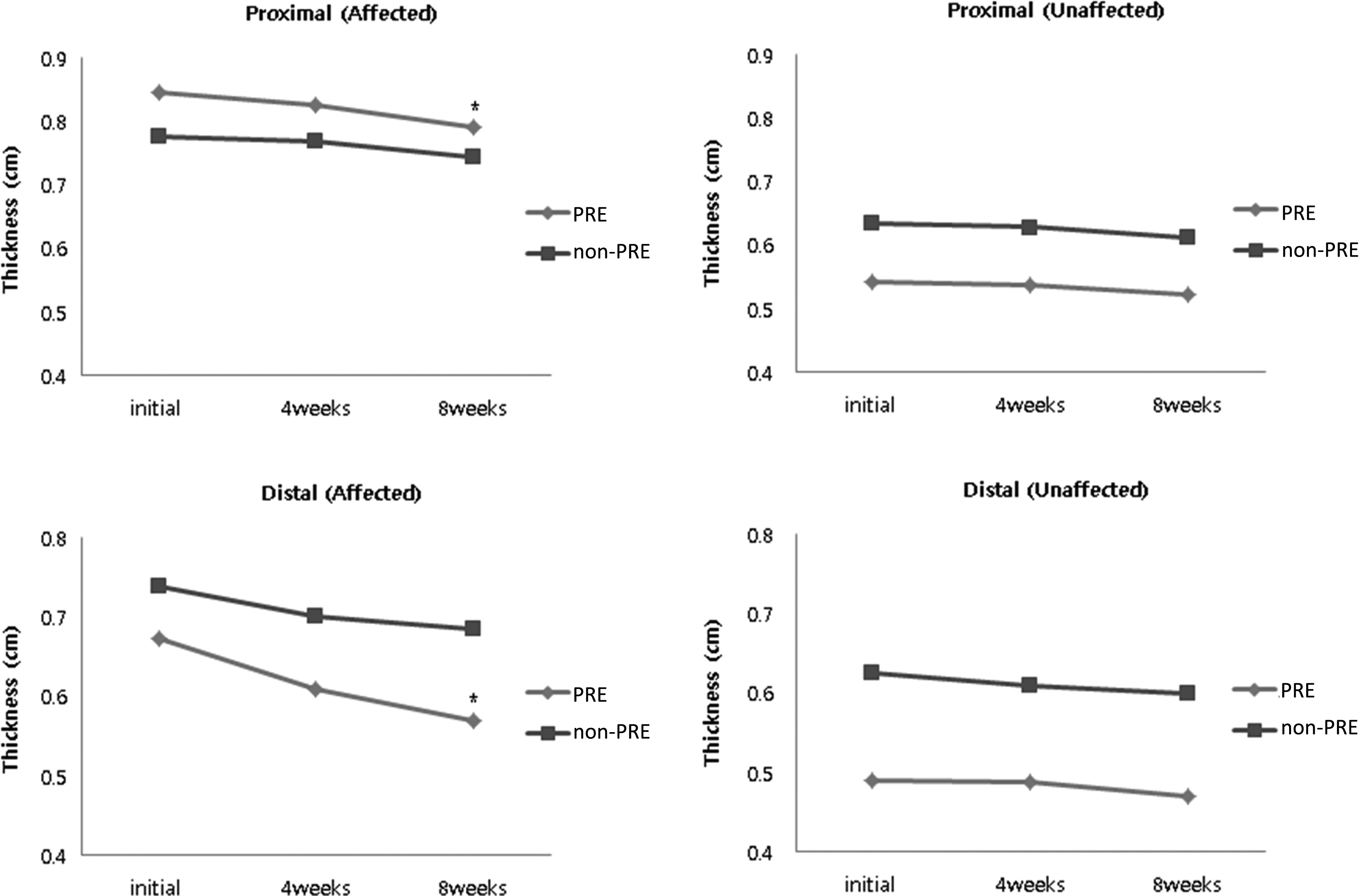
The PRE group showed that the muscle thickness of distal part significantly increased at 4 weeks and 8 weeks, and the proximal part significantly increased at 8 weeks (Fig. 5).
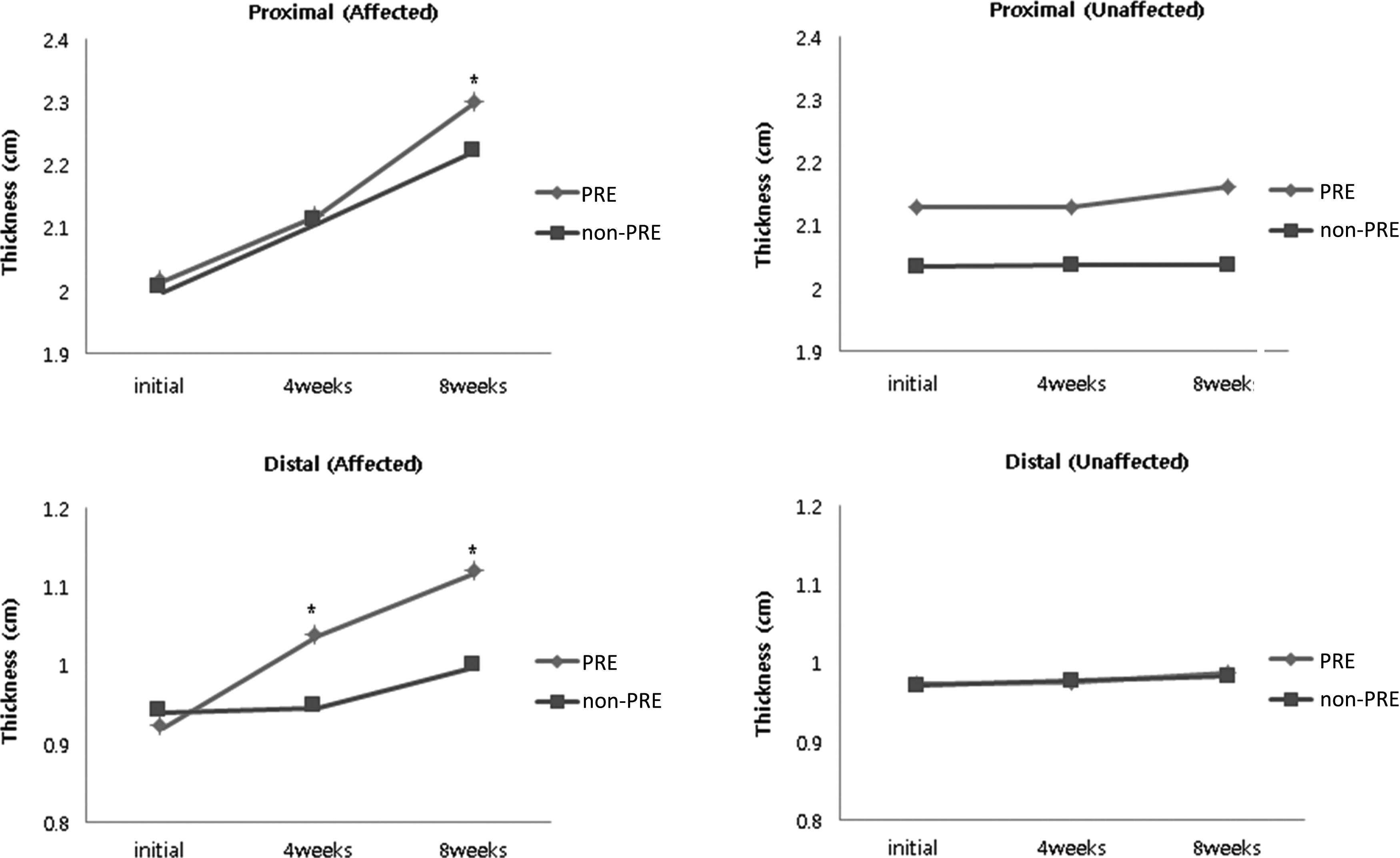
The thickness of muscle of affected limb and unaffected limb by ultrasonography. *p < 0.05 by repeated-measures ANOVA.
The thickness of subcutaneous tissue in the affected upper limb showed a significant decrease after 8 weeks in the PRE group. No significant differences were found in this parameter in the non-PRE group (Fig. 6).
The thickness of subcutaneous tissue of affected limb and unaffected limb by ultrasonography. *p < 0.05 by repeated-measures ANOVA.
Discussion
Most treatments for lymphedema are passive methods such as limb elevation, manual lymphatic drainage, massage therapy, pneumatic compression, and the use elastic compression sleeves. However, lymphatic fluid is circulated through the body by both active and passive actions. PRE can stimulate the skeletal muscle to pump venous and lymphatic fluid, 17 and can also stimulate contraction of the lymphatic vessels, which are controlled by the sympathetic nervous system. In this way, muscle contraction can increase the drainage of lymphatic fluid and the contraction of the lymph vessels. 15 Using a compression bandage during PRE creates a counterforce, providing an additional effect to increase the drainage of lymphatic fluid and to limit vascular permeability, which is affected by vascular pressure.14,21
Exercise is known to be beneficial for cancer patients; it results in clinically meaningful improvements and has positive physical and psychosocial consequences. Upper body resistive exercise is emerging as a particularly important therapy for BCRL patients, mainly due to its potential to improve muscular function and to increase lymphatic drainage by muscle pumping. Several intervention trials involving low to moderate load resistance exercise have been reported in BCRL patients, providing evidence regarding its safety.2,17,22 The effect of the PRE in combination with compression bandage may represent a potential additional treatment to improve lymph circulation.14,23 But, there are no standard method of PRE for BCRL patients.
In the present study, PRE was constructed using the six actions (dumbbell fly, triceps extension, one-arm bent-over row, biceps curl, dumbbell side raise, and lifting the arms forward). PRE is conducted by the method of increasing the number of six actions without increasing dumbbell weight.
In our study, it was confirmed that the muscle thickness of the affected arm was significantly less than the unaffected side. It may be due to direct damage of muscles by surgery or the influence of tissue by radiation therapy or chemotherapy, or other causes that breast cancer patients tend to avoid using the affected arm. It is believed that many patients usually have a considerable fear of resistive exercise and only perform stretching exercise and aerobic exercise such as walking, so that it appears to cause a decrease in muscle mass. However, in previous studies, progressive resistance exercise does not induce deterioration of lymphedema.22,24
In the changes of the circumferences of affected limb by tape measurement in the PRE group, no statistical significance was shown after 4 weeks. But after 8 weeks, there was a statistically significant reduction in circumferences of affected limb statistically significant. This is a result that continuous PRE increases the thickness of the muscle to promote the muscle pumping and accordingly reduce the thickness of subcutaneous tissue. As a result, lymphedema is more improved in PRE groups. So, it is necessary to do long duration of PRE for more effective treatment of lymphedema.
In this study, we found that PRE can reduce the circumferences of affected limb without any adverse effects. The arm volumes of patients with BCRL were decreased in the non-PRE group that received conventional therapy only, as well as in the PRE group. In particular, in the PRE group, there was significantly more proximal volume reduction of lymphedema, as compared with that in the non-PRE group.
In our experiment, we evaluated the therapeutic effects of PRE on skeletal muscle and subcutaneous tissue as measured by ultrasonography. Ultrasonography is less expensive than CT or MRI, easily accessible, safe from radiation exposure, and noninvasive, which means that it can be used as a diagnostic tool for lymphedema and also as a method to determine treatment efficacy.25,26 Ultrasonography is a good tool for measuring the change in thickness of the muscle following PRE, to confirm the treatment effect of lymphedema.
The main limitation of this study relates to the sample size, as the number of participants was small. In addition, ultrasonography measurements are operator dependent, and technical differences in pressure application during subcutaneous volume and compliance measurements may have affected the results. Furthermore, we got the values from only two anatomically defined points during ultrasound. In many studies, the lymphedema is defined as more than 2 cm larger circumference at 10 cm point of distal part and 10–15 cm point from the proximal part of the olecranon or lateral epicondyle.20,27 If lymphedema can be focal and may not have been present at these points, the effect of PRE will not be reflected.
In another limitation, we have not considered the dominant arm in this study. Muscle mass and overall arm volume is influenced by dominance of the arm. But, we have studied the sequential change of affected arm according to PRE compared to non-PRE group. So the confusing effect of dominant arm is expected to be minimal. Systematic research based on a large number of participants over a longer period of time is thus essential to further clarify the possible effects of PRE in treatment of lymphedema.
Conclusions
For the treatment of patients with BCRL, PRE with complex decongestive physiotherapy did not cause additional swelling, and it reduced arm circumference by decreased subcutaneous tissue thickness and increased muscle thickness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.