
Abstract
Abstract
Background:
An understanding of normal fluctuation of lymphedema over time is important to identify real change, whether it is from response to treatment or worsening of the condition. The weather is another factor that possibly influences lymphedema but has had minimal investigation to date. The purpose of this study was to determine the extent to which breast cancer-related lymphedema (BCRL) fluctuated over a 6-month period and the influence of temperature, humidity, and barometric pressure.
Method and Results:
Women with unilateral BCRL (n = 26) and without BCRL (n = 17) were measured on nine occasions over 6 months using a standardized protocol. Measures included self-reported arm swelling, arm volume, and extracellular fluid with bioimpedance. Daily weather data were obtained for analysis of effects on lymphedema. Neither arm volume nor extracellular fluid varied significantly for women with lymphedema; coefficients of variation were 2.3% and 3.7%, respectively. Women without lymphedema had even less fluctuation, with coefficient of variation of 1.9% for arm volume and 2.9% for ECF. Correlation of weather and lymphedema data showed that temperature was the only aspect of the weather to have any effect on BCRL, with the maximum temperature on the day before measurement slightly affecting ECF (r = 0.27, p < 0.001), arm volume (r = 0.23, p < 0.001), and self-reported swelling (r = 0.26, p < 0.001). For women without lymphedema, the weather did not affect any measure.
Conclusions:
Established BCRL is relatively stable over a 6-month period. Temperature was the only aspect of the weather found to impact lymphedema.
Introduction
L
Establishment of normal fluctuation of lymphedema over time is important to identify real change, whether it is from response to treatment or worsening of the condition. 8 We previously studied women with BCRL and identified minimal fluctuation over a 1-month period. 8 Clinically, however, women with established lymphedema are often reviewed every 6-months at the time when they are measured for new compression garments. 9 This study replicates this period of follow-up.
Another aspect of lymphedema behavior that has had minimal investigation to date is response to the weather. Hot weather and climates have been suggested as potentially exacerbating lymphedema.10–12 Physiologically, heat increases blood flow so a resultant increase in lymph production might be expected, 1 and women with BCRL have reported hot weather as an exacerbating factor. 13 Limited research has found that the season can affect treatment outcomes, 14 and a recent study of women without lymphedema has reported seasonal variation in arm volume. 15 However, the effect of heat and cold on lymphedema remains controversial. 16
The primary aim of this study was to determine the extent to which extracellular fluid, arm volume, and self-reported swelling fluctuated in women diagnosed with BCRL lymphedema compared to women without BCRL. Secondary aims were to determine if aspects of the weather, namely heat, humidity, and barometric pressure, influenced BCRL.
Methods
Ethical approval
This study was approved by the Human Research Ethics Committee of the University of Sydney. Informed consent was obtained from each participant prior to participation in the study.
Participants
Women who had previously received a diagnosis of unilateral arm lymphedema secondary to treatment for breast cancer (n = 26) and women without a history of lymphedema or breast cancer (n = 17) were recruited via media releases and advertisements in lymphedema support group newsletters. Women were excluded if they had a pacemaker or other inbuilt stimulator, or if they were pregnant, as this would contraindicate the use of bioimpedance. Women with clinically-diagnosed lymphedema were eligible to participate if they had not had any treatment for lymphedema in the previous 6 months other than self-management.
Participant characteristics are outlined in Table 1. Ethics approval was granted by the Sydney University Human Research Ethics Committee and all participants provided written consent before commencing this study.
Mean (standard deviation) are shown.
Measurement procedures
All women were measured over a 6-month period according to the following schedule: once per week for 4 weeks and then once per month for a further 5 months, for a total of 9 measures over a 6-month period. Continuous recruitment of women into this study over a 3-year period resulted in women being measured during all seasons.
Women with lymphedema who were wearing compression garments were asked to remove these 2 hours before each measurement session to allow their lymphedema to stabilize. Participants were measured at the same time of day on each occasion to minimize any effect of increased swelling as the day progressed and within a few minutes of arriving to minimize any effect from the research laboratory air conditioning.
At the initial assessment, medical and surgical history, current medication, height, weight, and arm dominance was ascertained. All women were assessed by the same experienced lymphedema practitioner. Lymphedema stage was determined by assessing reduction of swelling with elevation, pitting with pressure, and the presence of fibrotic and skin changes.
At the beginning of each of the measurement sessions women were also questioned regarding factors that may influence body fluid levels such as food and fluid intake for the day, changes in medication, exercise and, if applicable, menstrual cycle. Measurement was then completed in the order outlined below.
Self-report
Before any physical measurements, women with lymphedema were asked to indicate how swollen they perceived their affected arm to be on that day using a 10 cm visual analogue scale (VAS). The 0 cm anchor of this scale indicated “not at all” and the 10 cm anchor “extremely so”. Participants were instructed to mark the line at a point corresponding to how swollen their arm felt. The distance of this mark was measured after the assessment and recorded in centimetres.
Arm volume
Arm volume was measured using an opto-electric perometer (Perometer 350S, Juzo) according to a previously published standardised protocol. 8 Briefly, participants were positioned in sitting with their arm in 90 degrees of abduction, palm down on the perometer hand rest, and the tip of their middle finger touching the end of the hand rest. In this position, the perometer commences measurement from 5.3 cm from the tip of the middle finger, therefore capturing some hand volume. The distance between the tip of the middle finger to the ulna styloid was measured for each participant. Peroplus software™ was used to remove this hand volume, thereby standardizing the starting point for arm volume measurement as the ulna styloid.
Customized Peroplus software™ was used to calculate total limb volume from the ulna styloid to the maximum distance measureable along the arm towards the axilla. This distance varied between women due to difference in arm length and also body shape. As has been previously reported, trunk size and shape can prevent measurement of the upper part of the arm with a perometer for some women.8,17 We measured both the affected and unaffected arm of the women with lymphedema and the dominant and non-dominant arm of the women without lymphedema.
Extracellular fluid
Extracellular fluid (ECF) in the arm was measured using a single frequency bioimpedance analysis (SFBIA) instrument (Model XCA, ImpediMed Ltd., Brisbane, Australia) designed specifically for measurement of unilateral arm lymphedema. 18 The protocol for assessing ECF of the arm with the SFBIA device has been previously described. 18 Briefly, participants' jewelry was removed and they relaxed in supine on a non-conductive wooden bed, with their arms positioned in slight abduction by their side. The skin was cleaned with an alcohol wipe prior to the application of surface electrodes, the placement of which was standardized by use of bony anatomical landmarks of the hand, wrist, and foot.19,20 The tetrapolar electrode arrangement, by using the equipotential principle, enabled the standardization of the length of arm measured. 19 The impedance, in ohms, was determined for each limb and then expressed as an inter-limb bioimpedance ratio between the affected and non-affected arm of women with lymphedema, and the dominant and non-dominant arm of women without lymphedema.
The reliability of the perometry and bioimpedance measurement has been established in previous studies.8,21,22 Regular calibration checks were performed on both devices throughout this study in accordance with the manufacturer's recommendation.
Weather data
Daily weather data for the 3-year period over which the study occurred was supplied by the NSW Climate Services Centre of the Bureau of Meteorology from the records of local weather stations. These data included minimum, maximum, and average daily temperature, relative percent humidity, and barometric pressure. Data were matched with the day of measurement and, because of the possible effect of the weather in the days preceding measurement, data from 1 and 2 days before the day of measurement were also used in data analysis.
Data analysis
Perometer arm volume data were expressed as an inter-limb ratio of affected limb to unaffected limb for women with lymphedema, and dominant to non-dominant limb for women without lymphedema, enabling direct comparison with the ECF data. For analysis of self-report data, the raw VAS scores of perceived swelling of the affected arm were used.
The coefficient of variation of each individual participant's data across the nine measures was determined for each of the three measurement approaches (i.e., ECF, arm volume, and self-report of swelling). An independent samples t-test was then used to assess whether the coefficient of variation differed between the two groups, women with and without lymphedema, for ECF and volume methods. Self-report data were not visually normally distributed; therefore an independent sample Mann-Whitney U test was used to determine if there was a difference between the two groups for the co-efficient of variation of self-report.
In order to estimate whether differences between time points were statistically significant for volume, ECF, and self-reported swelling, a linear mixed model with an autoregressive covariance matrix was used for each of these outcome measure. This covariance structure allows data closer together in time to be more correlated than data points further apart. The interaction between time and group was included to allow the groups to change differently over time and to obtain least significant difference (LSD) post hoc comparisons of group within time. The first, fifth, seventh, and last measures were used in these analyses.
To determine if weather influenced lymphedema, data were analyzed using Pearson's correlation. Volume, ECF ratio, and self-report data from each of the measurement sessions were correlated to temperature, humidity, and barometric pressure on the day of measurement and 1 and 2 days before the measurement session. Interpretation of Pearson's r used the classification proposed by Domholdt: 23 r = 0 to 0.25 little if any correlation; 0.26–0.49 low correlation; 0.50–0.69 moderate correlation; 0.70–0.89 high correlation; 0.90–1.00 very high correlation.
Analysis was undertaken with IBM SPSS Statistics software version 22. For all tests, significance was set at p < 0.05.
Results
Participants with lymphedema were aged 62.5 (7.7) (mean (SD)) years with a BMI of 29.7 (9.1) kg/m2 and women without lymphedema were aged 52.6 (7.2) years with a BMI of 25.9 (3.3) kg/m2. There was a statistically significant difference between the two groups with regards to age (p < 0.001) but not BMI (p = 0.107). Ninety-two percent of women with lymphedema and 87% of women without lymphedema were right-hand dominant (Table 1). All women with lymphedema had compression garments, however compliance with use varied.
Lymphedema was well established, having been present on average for 7.1 (7.7) years prior to commencing this study. Lymphedema severity in the group ranged from Stage I in which swelling eases with elevation to late Stage II in which no reduction with elevation occurs, and fibrotic and adipose tissue proliferate. 2 The mean time since breast cancer surgery for these women, involving axillary lymph node dissection (ALND) and either a mastectomy or wide local excision (WLE), was 10 (8.1) years. All nine measurement sessions were attended by 59% of the women with lymphedema, and 47% of women without lymphedema (Table 2).
There was little variation in the measures over the 6-month measurement period for women with lymphedema with the exception of self-report, which fluctuated markedly (Fig. 1). Mean (SD) coefficients of variation of volume and ECF ratio measures in women with lymphedema were 2.3% (0.9)% and 3.7% (1.6%), respectively, and 1.9% (1.0%) and 2.9% (1.5%) for women without lymphedema. The two groups were not significantly different in the coefficient of variation of arm volume ratios as measured by perometry (0.36 (−0.24 to 0.96; p = 0.3)), but were significantly different in the coefficient of variation of inter-limb ECF ratios (1.1 (95% CI: 0.3 to 1.9; p = 0.01)).
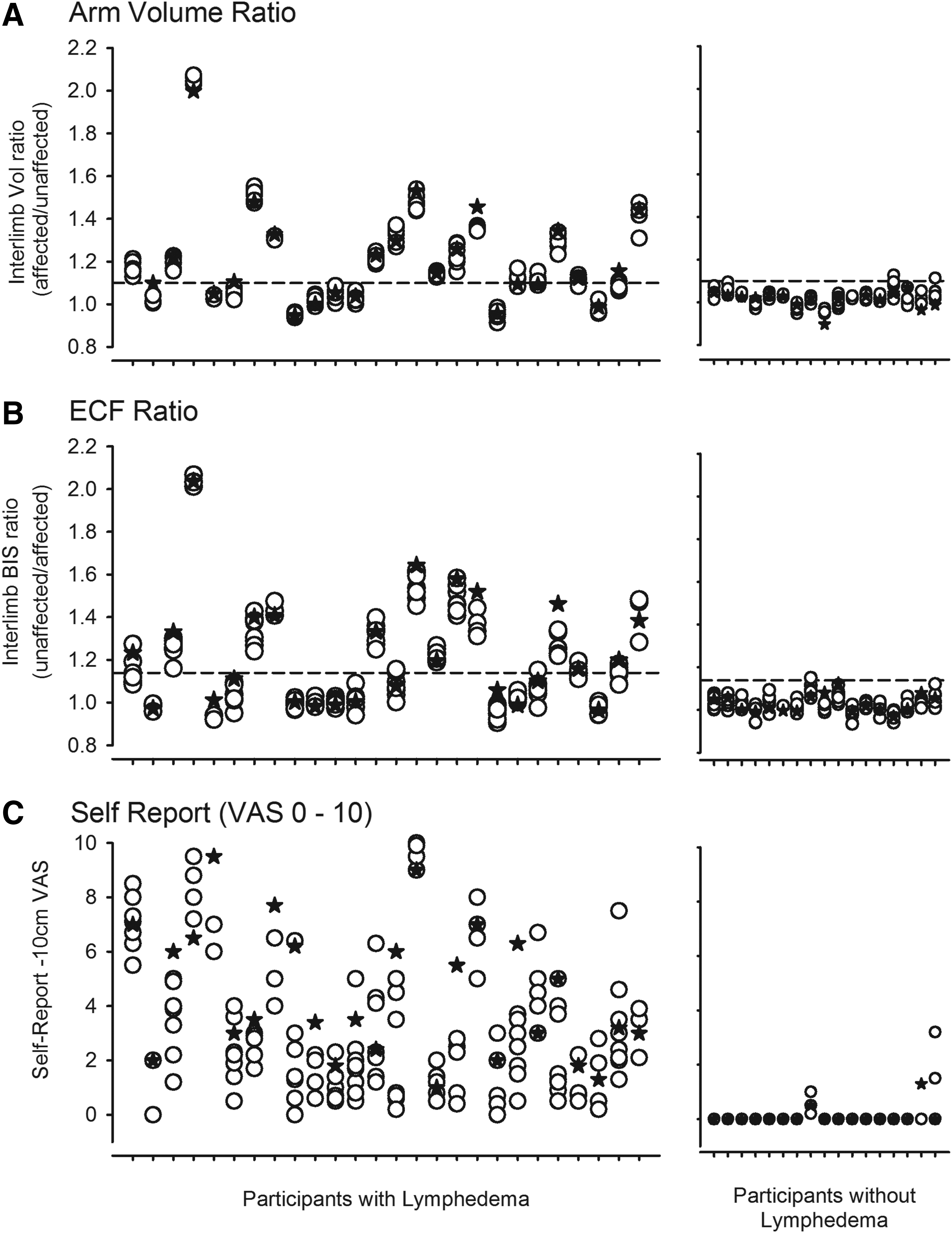
Representation of the nine measures over 6 months for each participant for arm volume, extracellular fluid, and self-report. Measure 1 is represented by a filled star; measures 2–9 are represented by open circles. Weekly measures for the first month. The order of participants is consistent among graphs.
As the self-report data were not normally distributed, the median (IQR) coefficients of variation for women with and without lymphedema and women were determined. The coefficient of variation for women with lymphedema was 52.5% (24.8%–68.5%) and for women without lymphedema was 0.0% (0.0%–0.0%). The two groups were significantly different (Mann-Whitney U test: p < 0.001).
Linear Mixed Models (LMM) analysis of inter-limb arm volume ratios revealed a significant difference between the two groups (Group: F (1, 40.8) 9.129; p = 0.004) but not over time (F(3, 92.9) 1.034; p = 0.381). There was a trend for the two groups to behave differently over time, (F(3, 92.9) 2.522; p = 0.06) but it did not reach significance. The mean between group difference at baseline was 0.251 (0.073) and 0.199 (0.074) at the last measurement (Fig. 2A).
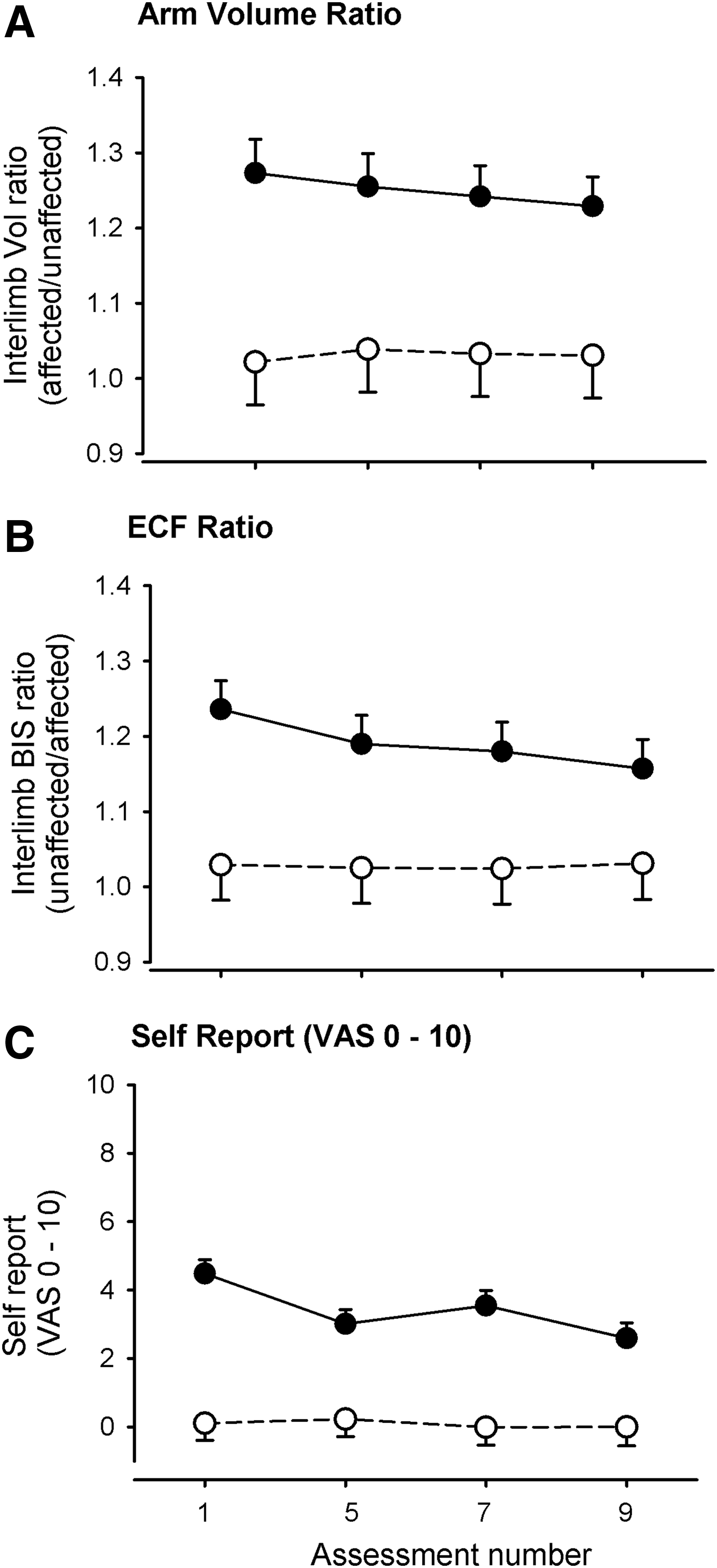
Change in measures of lymphedema over time. Participants with lymphedema are represented by filled circles and those without lymphedema by open circles. Means and standard error, derived by the linear mixed model, are shown.
LMM analysis of the inter-limb ECF ratio revealed significant differences between the two groups (F (1,40.4) 7.643; p = 0.009) and over time (F(3,98.1) 2.811; p = 0.043). At the initial assessment the ECF ratio was 1.236 (0.038) in the lymphedema group and 1.029 (0.047) in the group without lymphedema. Although there was a trend for the groups to behave differently over the 6-months, it did not reach significance at p < 0.05 (Group × time; F (3,98.1) = 2.571; p = 0.059). The difference between the two groups decreased over the measurement period as a result of the ECF ratios for women with lymphedema decreasing (Fig. 2B). The between group difference at the first measure was 0.207 (0.060) and 0.126 (0.062) at the last measure.
Analysis of self-report data revealed that overall the two groups were different (F(1, 39.1) 36.515; p < 0.001), and that they behaved differently over time (Group × Time: F(3, 93.3) 4.878; p = 0.003). Reflecting the decrease in physical measures of lymphedema, women in the lymphedema group rated their arm as less swollen over time, whereas women without lymphedema changed minimally and not significantly (Fig. 2C). The mean difference between measure 1 and measure 9 for women with lymphedema was 1.892 (p < 0.001) and for women without lymphedema was 0.105 (p = 0.863). At baseline, the between group difference was 4.379 (0.639) and at the final assessment was 2.592 (0.717).
Correlation of meteorological data and measures of lymphedema showed that neither humidity nor barometric pressure affected lymphedema (Table 3). Using Domholdt's criteria, 23 temperature had a low correlation with ECF (r = 0.27; p < 0.001), and self-reported swelling (r = 0.26; p = 0.001) and little correlation with arm volume (r = 0.23; p < 0.001) (Fig. 3, Table 3). No aspect of the weather was found to have any effect on the ECF, arm volume or self-reported swelling of women without lymphedema.
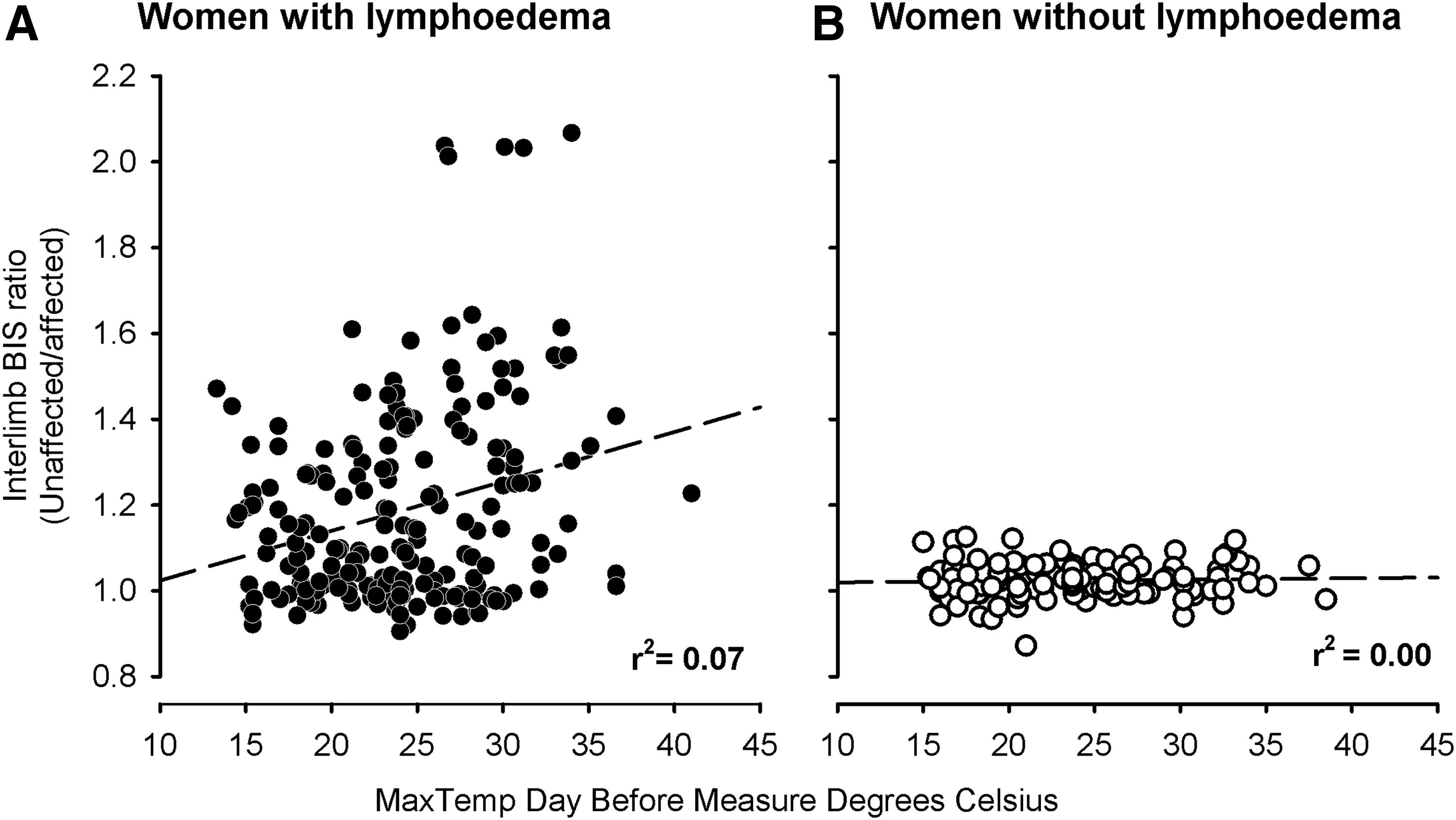
Effect of the maximum temperature on the day before measurement on ECF ratio.
Correlation is significant at the 0.01 level (two-tailed).
Discussion
These results indicate that established lymphedema in the self-management phase of treatment is relatively stable over a 6-month period. This supports current clinical practice in which women with BCRL are advised to be reviewed twice yearly for measurement of replacement compression garments unless an infection or other exacerbating event occurs. The stability of arm volume and ECF in women with established lymphedema also suggests that clinically, if changes are noted, they are more likely to reflect true change as opposed to normal fluctuation. It is acknowledged that variation in ECF, arm volumes and self-report over the nine measures would have included some technical error of measurement. Previous research has, however, established that this is minimal for each of the physical measurement methods used. 8
The trend seen towards slight improvement in ECF and arm volume over time for the participants with lymphedema may have been due to the effect of attending regularly for assessment as participants in the study. Regular attendance may have been sufficient stimulus to remind women to comply with their self-management program including wearing their compression garments regularly. At the end of each measurement session, women were informed about their results. Some reported becoming more active because now they could assess whether any lifestyle changes exacerbated their lymphedema. Evidence is growing for the benefits of exercise for women with lymphedema, 25 and an increased confidence to be active may have contributed to the trend towards improvement.
Our results showed greater fluctuation in ECF as measured by bioimpedance over time than in arm volume measures as measured by perometry. The variations in ECF, whilst detectable by bioimpedance, may not have always reached the magnitude required to impact on overall arm volume and be detectable by perometry. Regardless, the variation was minimal in the group with lymphedema, ranging from 1.192–1.123 for ECF ratio and 1.218–1.188 for arm volume ratio.
The variation in self-report in women without lymphedema was unexpected. Analysis of participant history revealed that of those who reported arm swelling, one had sprained her wrist and the others were in the process of having skin cancers removed. Although in these cases their ECF ratio was not affected, musculoskeletal injuries can cause increased ECF and decreased tissue impedance. 26 Since arm injuries can result in perceived as well as actual swelling in women without lymphedema, this potential confounder should be accounted for in control groups.
Women with lymphedema reported a reduction in the severity of swelling over time. This may have been a reflection of physical improvement or due to improved self-efficacy from access to their lymphedema measures. Importantly, it suggests that participation in this research and regular measures did not result in women becoming hypervigilant and distressed by their lymphedema.
The finding of only a low effect of weather on lymphedema may be considered surprising. However, Sydney, Australia, where this research occurred, has a temperate climate with an average yearly maximum temperature over the last 154 years of 21.7°C and an average yearly minimum temperature of 13.8°C. 27 The results of this study may therefore not be applicable to women living in climates that have greater range and extremes of temperature. In addition to investigating the behavior of lymphedema in more varied climates, it would be worthwhile to measure it in extreme weather conditions such as the prolonged heatwave recently experienced in Australia. 28 It has been suggested that extreme weather conditions such as this may become a more frequent occurrence as a result of climate change, with wide-ranging implications for health conditions. 29
The finding that barometric pressure had no effect on lymphedema is less surprising, given that aircraft cabin pressures, which are much lower, have been previously found not to impact extracellular fluid ratios. 30 The lowest instance of weather-related barometric pressure is a severe cyclone at approximately 930 hPa, 31 whereas aircraft cabin pressure is much lower, around 800 hPa.32,33 It would therefore appear unlikely, as supported by our results, that barometric pressure changes would have any effect on lymphedema.
The limitations of this study include the small sample size and the fact that not all women completed all nine measurement sessions. Although lymphedema may, in some patients, predominantly affect the hand, our measures of extracellular fluid and arm volume commenced at the wrist. Fluctuations distally in the hand would have been undetected. Bioimpedance measurement of hand extracellular fluid was not conceived at the commencement of this study; however recent research34–36 describes methods of assessing hand extracellular fluid and volume which could detect fluctuations in hand lymphedema. Participant weight was recorded initially but not at each measurement session. Weight lost or gained weight over the course of this study would have potentially impacted arm measures, although this was mitigated by comparison of data in the affected arm with that of the unaffected contralateral control arm.
Conclusions
Established lymphedema appears to be stable over a 6-month period, supporting the appropriateness of twice yearly clinical review for women in the self-management phase of treatment. The trend towards slight improvement with more frequent monitoring such as occurred in this study suggests, however, that there may be value in providing regular feedback to women. Temperature was the only aspect of the weather found to have an, albeit low, impact on lymphedema. Further research in more varied climates and more extreme weather conditions is indicated.
Footnotes
Acknowledgments
SC was supported by a National Breast Cancer Foundation (Australia) doctoral scholarship and by the RT Hall Foundation. SLK was supported by a National Breast Cancer Foundation (Australia) career research fellowship. The NSW Climate Services Centre of the Bureau of Meteorology is acknowledged for the provision of weather data. Professor Jennifer Peat is acknowledged for statistical advice and assistance.
Author contributions: SA Czerniec contributed to study conception and design, data collection, analysis and interpretation of data, and manuscript preparation. LC Ward contributed to study conception and design, analysis and interpretation of data, and manuscript preparation. SL Kilbreath contributed to study conception and design, analysis and interpretation of data, and manuscript preparation.
Author Disclosure Statement
Authors S. Czerniec and S. Kilbreath have no competing financial interests. Dr Ward consults to ImpediMed Ltd. ImpediMed had no involvement in the design, undertaking, or manuscript preparation of this study.