
Abstract
Abstract
Objective:
Upper limb lymphedema is a common complication after radical mastectomy in patients with breast cancer. In this study, we examined the efficacy of self-manual lymph drainage (MLD) after modified radical mastectomy for the prevention of upper limb lymphedema, scar formation, or shoulder joint dysfunction in breast cancer patients.
Methods:
Breast cancer patients scheduled for modified radical mastectomy were randomly apportioned to undergo physical exercise only (PE group, the control; n = 500) or self-MLD as well as exercise (MLD group; n = 500) after surgery. In the PE group, patients started to undertake remedial exercises and progressive weight training after recovery from anesthesia. In the MLD group, in addition to receiving the same treatments as in the PE group, the patients were trained to perform self-MLD on the surgical incision for 10 min/session, 3 sessions/day, beginning after suture removal and incision closure (10 to 30 days after the surgery). Scar formation was evaluated at one week, and 1, 3, 6, and 12 months after the surgery, respectively. Upper limb circumference and shoulder abduction were measured 24 h before surgery, and at one week, and 1, 3, 6 and 12 months after the surgery.
Results:
Compared to those in the PE group, patients in MLD group experienced significant improvements in scar contracture, shoulder abduction, and upper limb circumference.
Conclusions:
Self-MLD, in combination with physical exercise, is beneficial for breast cancer patients in preventing postmastectomy scar formation, upper limb lymphedema, and shoulder joint dysfunction.
Introduction
B
Consequent to destruction of the axillary lymphatic network, as many as 30%–50% of patients suffer upper limb lymphedema (ULL), that is, the abnormal accumulation of protein-rich fluid within the interstitial space of the ipsilateral upper limb.4,5 Studies have shown that ULL significantly reduces the quality of life of breast cancer survivors and is closely associated with a cluster of physical and psychological symptoms.6–10 Therefore, efforts to prevent and actively treat ULL are crucial for improving the health and life quality of these patients.
ULL can be considered acute or chronic, depending on whether the onset of symptoms is within or after 18 months of surgery. 11 Immediately after surgical dissection, acute ULL is usually transient, reversible, and resolved through multiple decongestive approaches, such as manual lymph drainage (MLD) massage, compression bandage, and physical exercise. 11 Chronic ULL is more severe, accompanied by progressive pain, swelling, recurrent infection, and upper extremity dysfunction. In addition, ULL is recalcitrant to the common effective approaches for treating acute ULL, and its causes are not clear, although some cases may develop from acute ULL. 11
At Sun Yat-Sen University Cancer Center, we are dedicated to improving the quality of life of breast cancer patients after surgical treatment. In this study, we report our observations and experiences using MLD in combination with physical exercise, for the prevention of acute ULL in breast cancer patients after modified radical mastectomy, as compared to physical exercise alone.
Methods
Patients
This study was approved by the Ethics Committee of Sun Yat-Sen University Cancer Center (Guangzhou, China) and written informed consent was obtained from all participating patients. One thousand women with breast cancer and scheduled for modified radical mastectomy at San Yat-Sun University Cancer Center between May 2012 and October 2014 were recruited into this study. These patients were randomly divided into two groups (n = 500/group) to receive either physical exercise alone (PE group) or MLD as well as physical exercise (MLD group).
Treatments
Beginning 24 h before surgery, patients in both groups received education regarding the risk of postsurgical complications and the importance of medical intervention and self-management. Training was repeated after the patient regained consciousness from anesthesia, daily thereafter for 3 days, and on the day of discharge (20–30 min/session).
The postsurgical remedial physical exercises were designed based on the National Lymphedema Network (NLN) Position Papers drafted by the NLN Medical Advisory Committee (http://www.lymphnet.org/le-faqs/nln-position-papers). The physical exercise program began with passive exercise within the first 7 days after surgery, before removal of the drainage tube. Between removal of the drainage tube and the surgical sutures at 7–30 days, the exercises progressed to localized active exercise on the affected upper limb. After removal of the surgical sutures, extensive active exercise involving the affected shoulder was undertaken, with three sessions/day, 15 min/session. All patients continue the remedial exercise for 6 months after the surgery.
In the MLD group, after suture removal and closure of the incision, the patients were trained to perform self-MLD three times per day (early morning, early afternoon, and evening) and for 30 min each session.
Each session was further divided into three sequential steps (10 min/step): to activate lymph vessels, to soften scar tissue, and to stimulate lymph drainage. To activate lymph vessels, the patient lies in bed, breathing deeply, and relaxing completely. Under a light pressure (approximately 25 mmHg), the palm sides of the index, middle, and ring fingers of the hands gently touch and move through the superficial lymph nodes, specifically from the cervical, subclavicular, axillary, subcapsular, and lumbar lymph nodes to the inguinal lymph nodes.
To soften scar tissues, the index, middle, and ring fingers of both hands are laid on the incision and a constant massaging pressure is applied in opposite directions to stretch the incision outward. After 5 seconds, the stretch is released and both hands are moved to a downstream location along the incision. The gentle stretch continues from the incision to the chest and the axillary region, to soften the connective tissue, and to minimize contracture-induced lymphatic obstruction, shoulder dysfunction, and chest constriction, as appropriate.
To stimulate lymph drainage, circular, spiral, or sweeping strokes are applied on the superficial lymph vessels from distal to proximal. Specifically, the lymph is drained from above the chest incision to the ipsilateral and contralateral axillary or subclavicular lymph nodes, from below the chest incision to the ipsilateral inguinal lymph nodes; from the ventral medial upper arm to the ventral lateral upper arm and supraclavicular lymph nodes; from the dorsal medial upper arm to the dorsal lateral upper arm and dorsal axillary lymph nodes or inguinal lymph nodes; and from the hand, forearm, and elbow to the lateral upper arm lymph nodes.
Assessment
Before the study enrollment, all participants completed a questionnaire that collected personal data including name, age, level of education, health insurance, career, marriage status, and family income. Clinicopathological data (tumor pathology and clinical staging) were also obtained.
ULL was assessed for each patient 24 hours before surgery and at 1 week, and 1, 3, 6, and 12 months afterward by tape-measuring the following upper limb circumferences: wrist, 8 cm above the wrist; 8 cm below the elbow, elbow, 8 cm above the elbow, and 8 cm below the shoulder joint. The stage of lymphedema (described below) was determined by postsurgical differences in upper limb circumferences between the surgical and contralateral sides, and objective observation by a trained lymphedema therapist. The stages of lymphedema were defined as follows.
No lymphedema: no difference was noticed on the upper limb circumference between the surgical side and the contralateral side. Stage I, or mild, lymphedema was defined as an upper limb circumference on the surgical side <110% that of the contralateral side. At this stage, the upper limb on the surgical side may appear mildly swollen, which may not be easily noticed. In addition, a temporary small dent may form when the skin is pressed, occurring more frequently in the internal posterior side of the upper limb.
At stage II, or moderate, lymphedema, the upper limb circumference on the surgical side is 110%–180% that of the contralateral side. The limb is obviously swollen, and the swelling may extend from the upper arm to the forearm on the surgical side. When pressed, no pit forms on the skin. There can be changes in the nails or skin such as inflammation or hardening, but upper limb motility is not affected.
At stage III, or severe, lymphedema, the upper limb circumference on the surgical side is >180% that of the contralateral side. Swelling is significant, and the skin takes on a leathery, wrinkled appearance. Superficial venous varicosities may be present in some cases. The edema affects an extensive area and is associated with motility dysfunction of the upper limb.
In addition to assessing the extent of lymphedema, the lymphedema therapist monitored scar formation on the patients using the Vancouver Scar Scale, 12 and shoulder function according to maximum shoulder abduction.
Statistical analyses
The SPSS 13.0 for Windows (SPSS, Inc, Chicago, Ill) was used for statistical analysis. Quantitative data were presented as mean ± standard deviation, and qualitative data were presented as frequency or percentage. The t-test, Chi-square test or Fisher's exact test was used to compare between groups as suitable. A p-value of <0.05 was considered statistically significant.
Results
To investigate the efficacy of MLD in preventing ULL after modified radical mastectomy, we recruited 1000 breast cancer patients and randomly assigned half to undertake physical exercises only, and half to perform MLD as well as physical exercises. Patients in these two groups (PE and MLD, respectively) were comparable in various clinicopathological characteristics, including age, pathological subtypes, differentiation status, tumor-node-metastasis staging, levels of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 (HER2), and lymph node metastasis (Table 1; all p > 0.05). While following the patients of both groups for 3 months, we monitored three main parameters: status of scar formation, extent of lymphedema, and maximum shoulder abduction.
IDC, invasive ductal carcinoma.
Scar formation
No obvious scar formation was noticed on patients from either group at 1 month after the surgery. By the third month after surgery, only 4 patients in the MLD group had developed scar contracture, while 12 had developed scar contracture in the PE group. In the PE group, 48 and 75 patients had scar contracture at 6 months and at 1 year, respectively, while in the MLD group the number remained at 3 to 4 during the same period (Fig. 1; all p < 0.05, MLD vs. PE). This suggests that MLD when combined with physical exercise is effective in preventing scar formation at the incision site.

Percentage of scar contracture during the 1-year follow-up in the MLD and PE and MLD groups. *p < 0.05, MLD vs. PE group.
Upper limb lymphedema (ULL)
Monitoring lymphedema development by measuring upper limb circumferences, we found that at 1 week after the surgery (before the start of MLD treatment), 7 and 8 patients developed mild lymphedema in the PE and MLD groups, respectively. At 1 month after the surgery, no patients in the MLD group, and 5 in the PE group had developed mild lymphedema, and only mild lymphedema was observed in both groups at the 1-year follow-up. However, in the PE group the numbers of patients with lymphedema were 23, 25, and 39 at postsurgical 3, 6, and 12 months, respectively, while at these time points lymphedema was observed in 6, 9, and 8 patients in the MLD group. This implies that MLD combined with physical exercise significantly reduces ULL after surgery, relative to physical exercise alone (Fig. 2; all p < 0.05 for 1 to 12 months, MLD vs. PE).
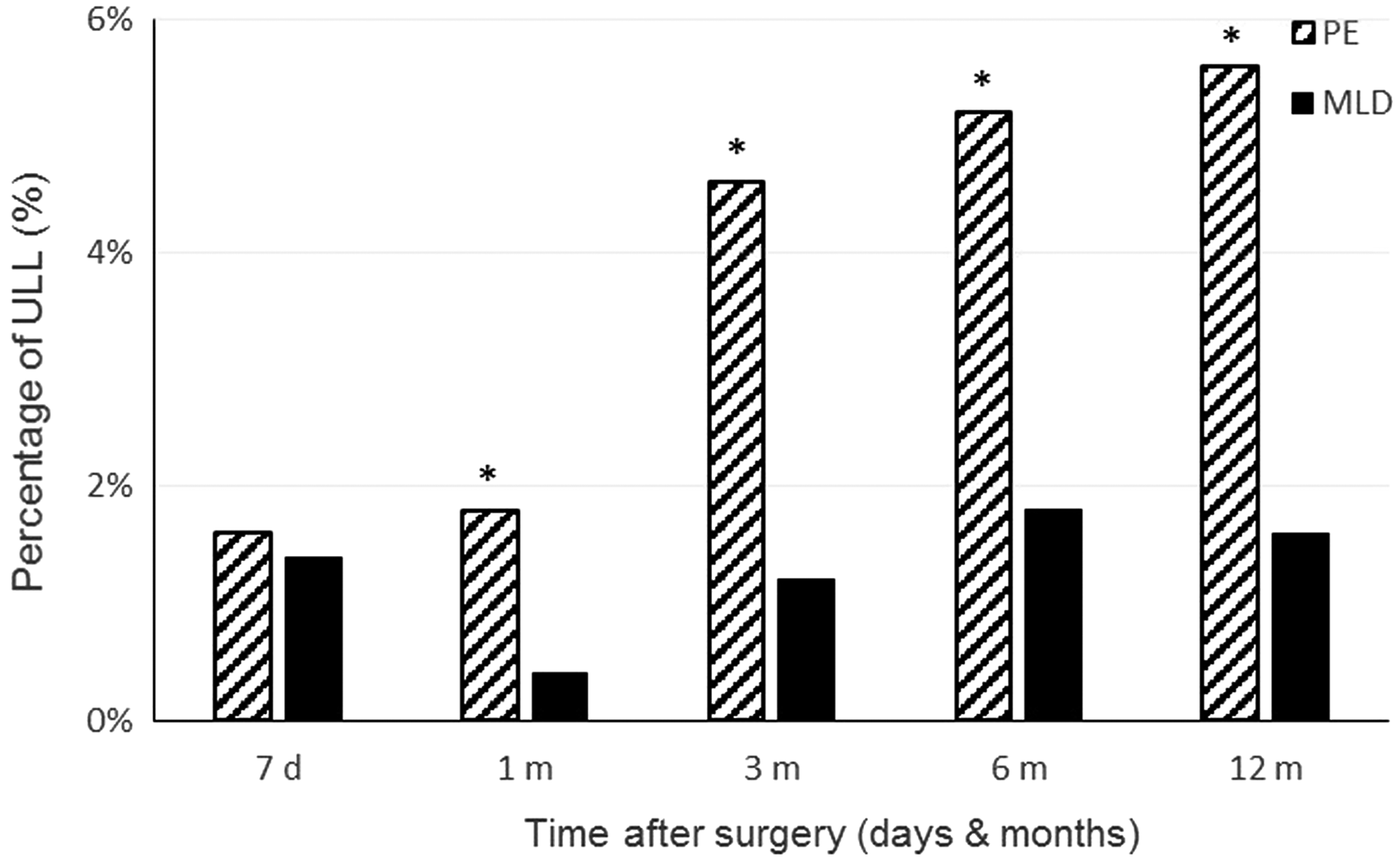
Percentage of ULL during the 1-year follow-up in the MLD and PE groups. *p < 0.05, MLD vs. PE group.
Maximum shoulder abduction
To evaluate upper limb function, we measured maximum shoulder abduction. At 7 days, and at 1, 3, and 6 months after surgery, the numbers of patients who could achieve 45°, 90°, 180°, and 180° shoulder abduction, respectively, in the MLD group were 489, 493, 498, and 500, which at each time point was higher than that of the PE group (476, 465, 452, and 489; Fig. 3; all p < 0.05, MLD vs. PE).

Percentage of patients achieving indicated degrees of shoulder abduction during the 1-year follow-up in the MLD and PE groups. *p < 0.05, MLD vs. PE group.
Discussion
In this randomized study, we evaluated MLD in combination with physical exercise, relative to physical exercise alone, in preventing ULL in breast cancer patients after modified radical mastectomy. We found that patients in the MLD group had less scar tissue formation and ULL, and better shoulder function, during the 1-year follow-up period.
Advances in the early detection and treatment of breast cancer have significantly improved patients' survival. 13 However, the current treatment modalities for breast cancer that include dissection or radiation of the axillary lymph nodes impose the risk of lymphedema, which can lead to morbidities of the upper limb, shoulder, and chest wall, deteriorate patients' quality of life, and increase socioeconomic burden.6–10,14 To ensure the quality of life of breast cancer survivors, it remains crucial to prevent lymphedema as well as other complications.
Lymphedema may occur from months to years after surgery and postsurgical therapy, and chronic lymphedema is often insidious and difficult to treat. 11 Early detection and thus early intervention may prevent a slow progression to a chronic condition. In this regard, patient education to identify early symptoms and signs associated with lymphedema, together with objective measurement of ULL, are essential for timely diagnosis and intervention.
Several means of objectively measuring upper limb circumference have been established, the three most common being water displacement, perometry with infrared laser, and circumferential tape measurement. 15 All of these methods for assessing lymphedema are highly reliable and well correlated, but are not inter-consistent in defining lymphedema15–18 and each has disadvantages. The water displacement method to detect lymphedema is cumbersome and time-consuming, which discourages its use in clinic. The cost of perometry similarly prohibits its practical use. Thus, tape measurement of upper limb circumferences is the method most commonly used. 19
Using the tape measurement method, either the circumferences at different locations along the upper limb or volumes calculated from the measurements can be used to determine lymphedema. It is generally agreed that an inter-limb difference of 2 cm or more at any single location, or a volume difference of ≥200 mL qualifies as lymphedema. 18 In the present study, we used tape measurement and observed significant reduction in the circumference of the sick upper limb after MLD combined with physical exercise, relative to physical exercise alone. This supports the efficacy of MLD for reducing the risk lymphedema in breast cancer patients after modified radical mastectomy.
At present, complete decongestive therapy (CDT) has been proposed as standard care for lymphedema.20,21 CDT is a multi-modality therapeutic program that comprises MLD, short-stretch compression bandaging, lymphatic exercise, skin care, and sometimes intermittent pneumatic compression. 20 The relative contributions of each component to the efficacy of CDT vary with compliance and the pathophysiological status of patients. 22 The best combination of components will not only enhance therapeutic efficacy, but also reduce the financial burden of healthcare on patients. Therefore, we designed this randomized study to compare the efficacy of MLD combined with physical exercise with that of physical exercise alone.
MLD is a light, hands-on technique. It differs from deep muscular or myofascial massage in that it works on superficial lymphatic vessels and tissue fluids in subcutaneous tissues, which is where lymph accumulates after lymphatic destruction. 23 With MLD, the excess interstitial fluid of lymphedema drains into the blood system. A recent study showed that MLD does not increase the risk of breast cancer recurrence in patients with breast cancer-related lymphedema. 24
In the present study, we found that MLD combined with physical exercise was associated with less lymphedema volume relative to exercise alone, and also significantly lessened scar formation at the site of the surgical incision. Concomitant with less scar formation and ULL, MLD was associated with better recovery of shoulder function, as reflected by differences in maximum shoulder abduction between the two treatment groups. Although several studies found that MLD did not add therapeutic benefits when combined with other CDT modalities,25,26 others have suggested the opposite. 27 The results of these studies mainly relied on upper limb volume changes, subjective assessment, or both. Here we propose that other phenotypic and functional parameters should be taken into consideration for future evaluation of the efficacy of MLD.
In summary, herein we present our clinical observations that MLD, when combined with physical exercise, effectively prevents ULL, alleviates scar formation, and stimulates functional recovery. This study justifies future studies on MLD as an essential therapeutic modality in combination with other CDT modalities to treat breast cancer-related lymphedema.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81472469), Sun Yat-Sen Excellent Young Teacher Program (12ykpy15) and the CMB Excellent Young Teacher Program (10-020-201212).
Author Disclosure Statement
No competing financial interests exist.