
Abstract
Abstract
Background:
To investigate the therapeutic effect of far infrared rays and compression bandaging in the treatment of chronic lymphedema with dermatolymphangioadenitis (DLA).
Methods:
Between 2005 and 2013, 106 patients with chronic lymphedema with DLA treated at the Shanghai Ninth People's Hospital were retrospectively reviewed. These patients were divided into an infrared and a bandaging group (80 patients, group 1) and bandaging only group (26 patients, group 2). Outcome measures include DLA frequency, patients' subjective feedback with regards to their symptoms, and the relationship between continuous elastic compression bandaging and relapse of DLA.
Results:
The frequency of DLA in group 1 and group 2 were significantly reduced after treatment (p = 0.000 and 0.004, respectively). Seventy five percent (60) of patients in group 1 and 19% (5) of patients in group 2 suffered no further episodes of DLA during the follow-up period. In group 1, over 90% of patients reported a subjective improvement in their symptoms and the relapse rate was shown to be lower using elastic compression bandaging when higher pressures were applied.
Conclusion:
Heating with compression bandaging can be an effective treatment strategy to reduce DLA and improve the quality of life for those patients with chronic lymphedema associated with DLA.
Introduction
C
DLA is a common and serious complication associated with so-called “filarial” patients as well as nonfilarial lymphedema. It affects the skin, lymphatics, and lymph nodes. The symptoms and signs include circumscribed or diffuse erythema of the affected skin, red streaks running in line with the superficial lymphatics on the medial aspect of the affected limb, tender enlarged inguinal lymph nodes, and high fever, which can in some cases reach 41.5 C°. DLA is usually caused by coagulase-negative Staphylococci with S. epidermidis being the usual dominant organism involved.2–4
Surgical treatment options for lymphedema include lymphatico-venous anastomoses, 5 free lymph node flap transfer, 6 and laser-assisted liposuction. 7 Some of these techniques require the use of microsurgery and may be associated with a small risk of producing donor site lymphedema. Moreover, these methods are more effective when used in the setting of mild lymphedema.8,9 In contrast, conservative treatment modalities can be used on a wide spectrum of cases and are not associated with the morbidity of surgery.10,11 Conservative treatment includes manual lymph drainage, heating and bandage treatment (HBT), intermittent pneumatic compression, single bandage treatment (SBT), as well as medical therapies.1,12,13
HBT was first described by T.S. Chang in 1964. Since then, it has been used for treating lymphedema for over 50 years and more than ten thousand patients have been treated using this modality.14,15 However, to date there are few reports concerning the use of HBT in the treatment of chronic lymphedema of the extremities accompanied by DLA. In this article, we retrospectively compare the therapeutic effect in 80 patients treated by HBT to 26 patients treated by SBT alone between 2005 and 2013 with chronic lymphedema of the extremities associated with DLA.
Patients and Methods
Ethical aspects
This study was approved by the local Ethics Committee of the University. Written informed consent was obtained from each subject before entrance into the study. The research was conducted in accordance with the ethical standards of the responsible committee on human experimentation and the Helsinki Declaration of 1975.
Inclusion criteria
Inclusion criteria was unilateral extremity lymphedema in stages I–III as defined by the International Society of Lymphology (ISL) classification,10,11 associated with an incidence of DLA of greater than one episode per year.
Patients were excluded if they had clinical or radiologic evidence of ongoing malignancy, or had an associated co-morbidity that would preclude daily treatment and follow-up. In addition, those patients with a contraindication to heat and compression bandage therapy, such as untreated infection or vessel thrombosis, as well as those who were unable to provide consent or adhere to the protocol or had extremities of such huge size as to preclude their placement in the cabin of our machine, were excluded from the study.
Patients
One hundred and six patients were enrolled in our study (Table 1), with 29 being male and 77 female. Thirty eight were diagnosed with upper extremity lymphedema, and 68 with lower extremity lymphedema. Twenty four were diagnosed as having primary lymphedema, and 82 with secondary lymphedema. The mean age in our series was 51.34 years (range 14–80) and the mean duration of lymphedema was 18.89 years (range, 1–67). These 106 patients were divided into two groups: group 1 (80 patients) was treated by HBT, whereas group 2 (26 patients) was treated by SBT (Table 1).
Therapeutic intervention
Group 1
Patients received HBT at The Shanghai Ninth People's Hospital, China. We used a specialized cabin for producing far infrared rays (3–1000 μm electromagnetic waves) (Fig. 1). This far infrared ray machine contains six far infrared ray tubes for producing heat and a regulator for controlling the temperature. The patients were treated for 2 hours with the far infrared ray machine at a temperature of 42°C each day for 4 weeks (5 working days per week) for a total of 20 sessions (one course).

A far infrared ray producing machine, made by the Ninth People's Hospital in Shanghai. Patients place their extremities in its cabin for heating treatment.
After each session, a trained therapist would bandage the patient's upper or lower extremity using elastic compression bandages (Hartmann, Germany) from the hand/foot and working proximally to the shoulder/thigh. Bandages were worn for the intervening 22 hours. Patients were also taught self-bandaging techniques to allow for maintenance of bandaging over weekends and to facilitate bathing. All patients received advice concerning skin care, exercise, and the maintenance of a healthy body weight.
Group 2
Patients only received SBT in Shanghai Ninth People's Hospital. This intervention was continued for 4 weeks (5 working days per week) for a total of 20 sessions (one course). Bandages were worn for the whole 24 hours per day, and patients were also taught self-bandaging techniques to allow for maintenance of bandaging over weekends and facilitate bathing. All patients received advice concerning skin care, exercise, and the maintenance of a healthy body weight.
Follow-up
At follow-up, these factors were recorded: 1) Frequency of DLA: The frequency of DLA episodes occurring per year in the patients included in our study was recorded. DLA was diagnosed by clinicians and the symptoms and signs clearly documented in the medical records. 2) Subjective patient feedback: Subjective patient reporting after treatment concerning outcomes such as pain, functionality, and quality of life (evaluated by a questionnaire) were obtained (Fig. 2).16,17 3) The impact of continued compression bandaging on DLA recurrence after the therapeutic period.
The follow-up questionnaire for patients.
Statistical analysis
The change of Frequency of DLA did not fit a normal distribution. The Wilcoxon rank-sum test was therefore used and all data analyses were conducted using SPSS version 19.0 (significance p < 0.05).
Results
Frequency of DLA
The average follow-up time was 4 ± 1.7 years. The mean frequency of DLA in group 1 was 4.3 ± 4 times/year before HBT. After treatment the frequency per year was significantly reduced to 0.6 ± 2.4 times/year (Z = 7.598, p = 0.000) (Table 2, Fig. 3).
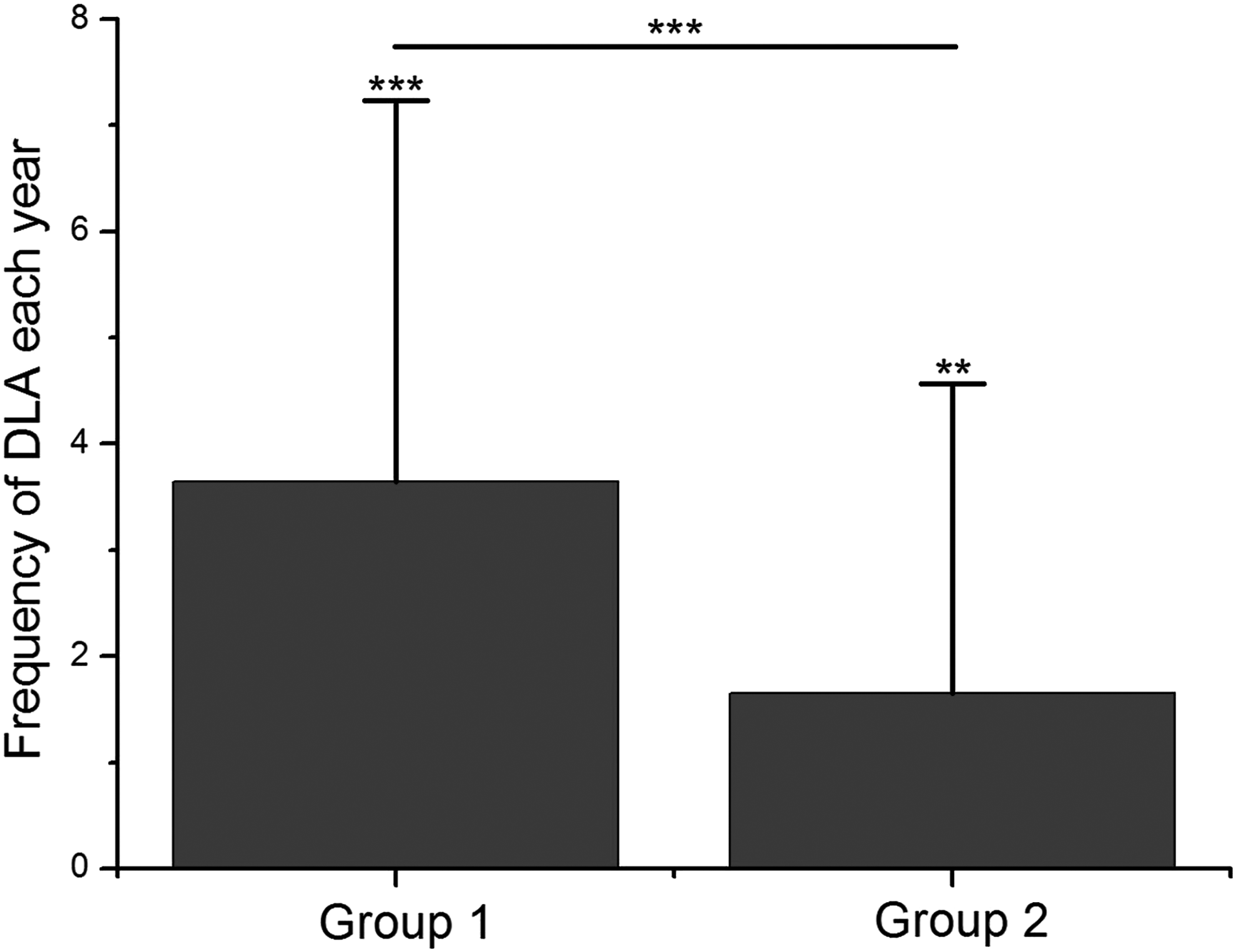
The changes of frequency of DLA after treatment. In group 1 (HBT group) and group 2 (SBT group), the frequency of DLA reduced. The frequency of DLA in group 1 reduced significantly compared with the reduction in group 2. *p < 0.05; **p < 0.01; *** p < 0.001; HBT, heating and bandage treatment; SBT, single bandage treatment.
HBT, Heating and bandage treatment; SBT, Single bandage treatment.
The mean frequency of DLA in group 2 was 3.2 ± 3.2 times/year before SBT. After treatment, the frequency per year was significantly reduced to 1.5 ± 1.2 times/year (Z = 2.866, p = 0.004) (Table 2, Fig. 3).
The frequency of DLA in group 1 was significantly reduced compared with the reduction in group 2 (Z = 3.806, p = 0.000) (Table 2, Fig. 3). In group 1, 60 (75%) patients did not experience any further episodes of more DLA during the follow-up period, whereas in group 2, five (19%) had no further episodes of DLA (Fig. 4).

Distribution of occurrence frequency of DLA (OFD) every year. Vertical axis represents the number of patients accompanying DLA. Horizontal axis represents OFD every year. The blue strip-type shows the distribution of OFD every year before treatment. The red ones express the distribution of OFD every year after treatment.
Subjective patient feedback
In group 1, 95% of the patients reported that they experienced significant improvement in their symptomatology, with 96.25% reporting reduction in pain, and 98.75% reporting improved quality of life (p < 0.05) (Fig. 5), confirming that HBT does produce a subjective improvement in the patients' condition.
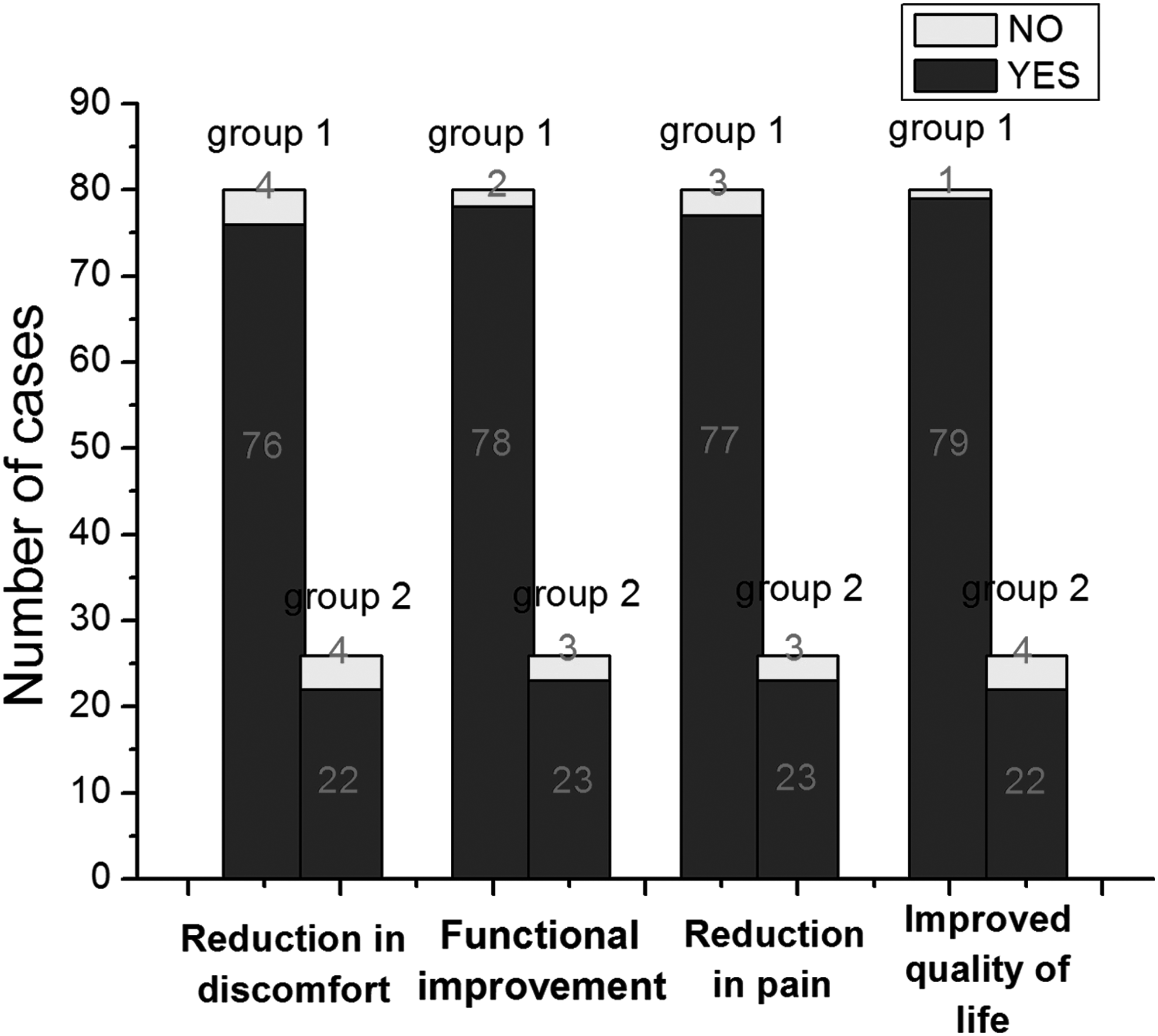
The improvement of symptomatology after treatment. In group 1, 95% of the patients reported that they experienced significant improvement in their symptomatology, with 96.25% reporting reduction in pain, and 98.75% reporting improved quality of life (p < 0.05). In group 2, 84.62% of patients reported an improvement in their symptomatology, with 88.46% reporting a reduction in pain and 84.62% reporting an improvement in quality of life (p < 0.05).
In group 2, 84.62% of patients reported an improvement in their symptomatology, with 88.46% reporting a reduction in pain and 84.62% reporting an improvement in quality of life (p < 0.05) (Fig. 5).
Ongoing compression bandaging to reduce DLA relapse
Among the 80 patients who had undergone treatment by HBT, 12 cases did not continue to use compression bandaging after the 4-week therapeutic period. Subsequently, four (33.3%) from this group experienced a rise in DLA recurrence. Sixty-eight patients continued to use the compression bandaging after the 4-week study period, and of this group, nine (13.2%) patients experienced a rise in the frequency of DLA recurrence (Fig. 6). The difference in DLA recurrence between these two groups is indeed statistically significant (p < 0.001), and this demonstrates the importance of ongoing compression bandaging of the affected extremity.
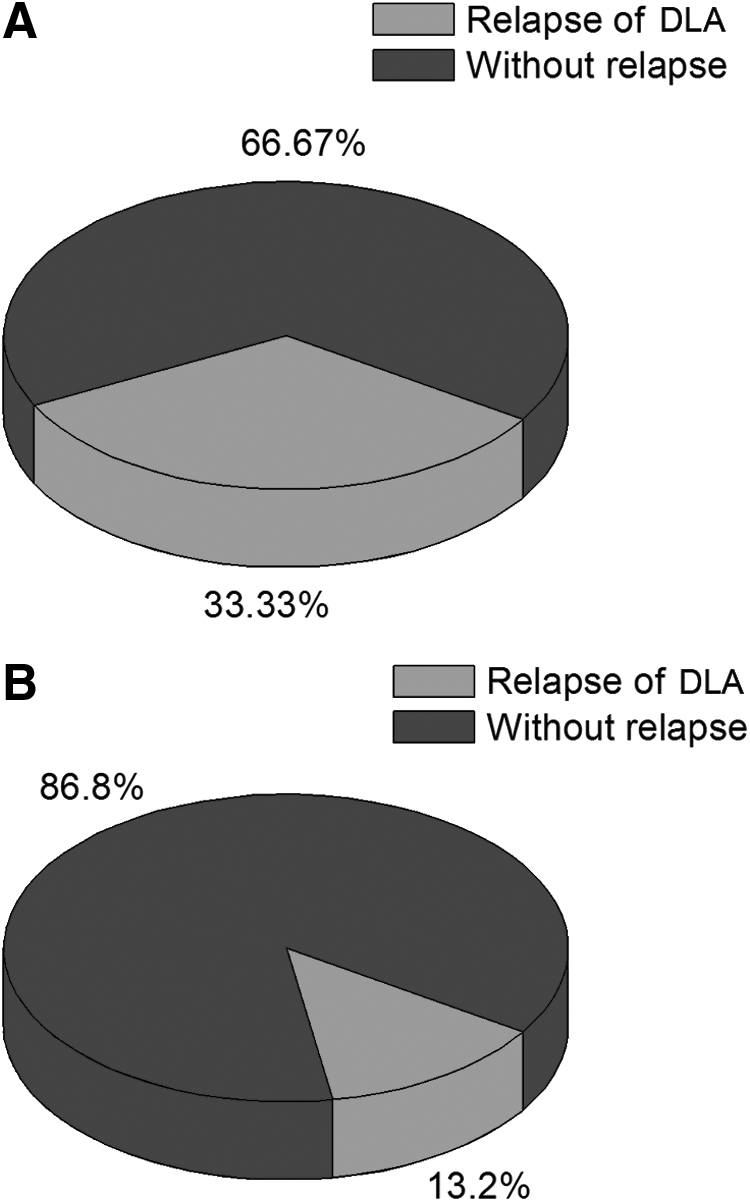
Among the 80 patients who had undergone treatment by HBT, 12 cases did not continue to use compression bandaging after the 4-week therapeutic period. Subsequently 4 (33.3%) from this group experienced a rise in DLA recurrence. Sixty-eight patients continued to use the compression bandaging after the 4-week study period and of this group 9 (13.2%) patients experienced a rise in the frequency of DLA recurrence. The difference in DLA recurrence between these two groups is indeed statistically significant (p < 0.001).
Discussion
The lymphatic system represents the second major circulatory system in our bodies that plays a significant role in the regulation of fluid balance. Its obstruction leads to the accumulation of tissue fluid that can be classified into primary and secondary lymphedema. Primary lymphedema is caused by dysontogenesis of the lymphatic system, 18 whereas secondary lymphedema can result from a myriad of differing pathologies that commonly includes factors such as trauma, infection, surgery, and radiotherapy.19–21 DLA is a common and serious complication of extremity lymphedema. Clinical signs of DLA include circumscribed erythema of the skin around the affected extremity, red streaks paralleling the superficial lymphatics, enlarged painful regional lymph nodes, as well as high fever. 2
Olszewski et al. 22 note that impaired lymphatic drainage and lack of elimination of penetrating bacteria may be responsible for the progression from uncomplicated lymphedema to that associated with recurrent attacks of DLA. Zaleska et al.23–25 confirm that compression of the affected limb can lead to the formation of new tissue channels that can help in reducing the accumulation of lymph fluid. Indeed, Dayes et al. have recently shown that SBT alone was as effective as compression bandaging with decongestive massage therapy with regards to percent reduction in arm volume in a study looking at women with arm lymphoedema after breast cancer surgery. 26
In our research, we found that the frequency of DLA in the SBT group decreased (p < 0.05), which illustrated that SBT could treat DLA patients effectively by leading to formation of new tissue channels and reducing excess lymph fluid, consistent with the current literature.
Far infrared rays represent an invisible portion of the electromagnetic spectrum with the wavelength ranging from 4.0 to 14.0 lm. It has three biological effects on soft tissues: radiation, resonance, and heat, 27 which cause local vessel dilatation and an increase in capillary circulation. Cao et al. have shown that this thermal effect can enhance an organism's immune function. 19 Liu et al. have demonstrated that local hyperthermia can stimulate Langerhans' cells, macrophages, and endothelial cells, which can result in an enhanced reaction to MHC class II antigens and thereby lead to increased cytokine production giving rise to increased activity of macrophages and natural killer cells.28–33
In addition, local hyperthermia can also promote the production of CD4+ T-cells and increase the ratio of CD4+/CD8+ T-cells, potentially strengthening the local immunological environment. Indeed, as the active macrophages clear and hydrolyze the excess proteins in lymphedematous tissue, the colloid osmotic pressure decreases leading to an increased absorption of interstitial fluid back into the systemic circulation. This positive effect of thermal energy on the soft tissues has been demonstrated by Hu et al. who have confirmed that local hyperthermia can also help to increase the microcirculatory blood flow, eliminate chronic inflammation, and promote tissue recovery.34–36
We have demonstrated that the therapeutic effect on DLA in the HBT group is superior to that in the SBT group (p < 0.05). This illustrates the therapeutic advantage that far infrared rays in combination with compression bandaging can have on DLA compared to SBT alone. We postulate that HBT promotes this beneficial outcome by improving the local immunological environment in addition to reducing the build-up of excess lymph fluid that serves as a bacterial culture medium.
In addition, several mechanisms such as the promotion of local lymphatic flow, 37 inhibition of transforming growth factor-b (TGF-b) gene expression, 32 promotion of lymphatic vessel regeneration, 38 and reduction in pain secondary to a reduction in formation of interleukin-6 (IL-6) and endothelin-1(ET-1), 36 have been demonstrated to play a role in the beneficial effect seen with thermal energy in the setting of lymphedema.
Chang et al. 39 demonstrated in 2004 that the volume of lymphedematous extremities could be significantly decreased after one to two courses of HBT. Our study supports this finding. Interestingly, 13 (16.25%) cases saw a rise in frequency of DLA after they had completed the HBT course. The earliest time to relapse was 1.4 years and the mean time was 3.4 ± 2 years. Hence, we advise that patients with chronic lymphedema associated with DLA should receive a course of HBT every 1–2 years, which should help to keep relapses of DLA at bay.
When treatment is completed, continuing use of compression bandaging is a very powerful tool to maintain the therapeutic effects on DLA. In our study, 64 (80%) patients continued to use compression bandaging after the treatment period and the rate of deterioration in this group was 13.2%. The other 16 (20%) patients who were not compliant with continued compression therapy experienced a rate of deterioration of 33.3% (p < 0.05), confirming the positive therapeutic effects of continued compression.
Conclusions
HBT is a useful treatment modality for the treatment of chronic peripheral lymphedema with associated DLA. In our study, the therapeutic benefit of HBT was demonstrated to be superior to SBT alone. In addition, continued use of compression bandaging after the therapeutic period consolidated the positive effects seen with HBT amongst our patients.
Footnotes
Acknowledgment
This research was supported by Natural Science Foundation of China (81272146)
Author Disclosure Statement
None of the authors has financial conflicts or interests to report in association with this article.