
Abstract
Abstract
Background:
This study aimed to determine the specific fluid distribution pattern in legs with lymphedema (LE) in comparison to normal legs and legs with venous edema (VE) using bioelectrical impedance analysis (BIA).
Methods and Results:
BIA was performed in 47 patients with lymphedema (LE; 63 legs), 33 patients with venous edema (VE; 60 legs), and 33 normal subjects (N; 66 legs). The ratio of intracellular fluid (ICF) resistance (R i ) to extracellular fluid (ECF) resistance (R e ) of a whole leg normalized to the right arm (Ri/Re leg), a surrogate parameter for ECF/ICF, and the R i /R e of the thigh and calf without normalization (R i /R e thigh , R i /R e calf , respectively) were obtained. Increases in Ri/Re leg (N 2.5 ± 0.7, VE 3.9 ± 3.7, LE 3.7 ± 1.5), R i /R e thigh (N 1.8 ± 0.5, VE 3.2 ± 3.8, LE 3.8 ± 1.9), and R i /R e calf (N 2.6 ± 0.6, VE 4.6 ± 1.7, LE 4.4 ± 2.2) were confirmed in VE and LE compared to normal subjects. However, the ratios of R i /R e calf to R i /R e thigh in normal subjects and those with untreated VE/LE were all ∼1.5 (N 1.5 ± 0.3, VE 1.5 ± 0.7, LE 1.6 ± 0.7).
Conclusions:
Fluid content was increased in legs with VE and LE compared to normal subjects, while the mode of gravitational fluid distribution was similar among all legs. Thus, no specific finding for LE was confirmed.
Introduction
B
Generally, the symptoms in legs with venous edema (VE) are evident in the lower part of the leg, but swelling of the thigh can be evident, particularly in secondary LE. In contrast, we previously reported that subcutaneous echo-free space observed with ultrasonography, which indicated local fluid accumulation in subcutaneous tissue, was similarly distributed according to gravity both in legs with VE and LE. 8 Thus, it is unclear whether there is a specific fluid distribution pattern for LE when compared to legs with other types of edema or normal legs. The current study attempted to answer this question.
Patients and Methods
This study was approved by the Institutional Review Board of Yamaguchi University Hospital (Ube, Yamaguchi, Japan). All participants gave informed consent before enrollment. The subjects included in the current study were 33 patients with VE and 47 patients with leg LE who attended our clinic between April 2015 and September 2015. Thirty-three healthy volunteers were also assessed. The diagnoses were made by patient histories, physical examinations, blood tests, chest radiograms, and electrocardiograms, to exclude edemagenic conditions due to systemic diseases. A duplex venous ultrasound was performed to find any reflux in the deep veins, saphenous veins, accessory saphenous veins, and perforators. Subcutaneous tissue ultrasonography8,9 was also performed to find changes in echogenicity that possibly correlated with inflammatory change and echo-free space that indicated accumulation of free fluid. Absence of any abnormal findings in the above examinations was confirmed in normal subjects. In this study, edema found in the legs with primary venous insufficiency, post-thrombotic syndrome, and functional venous insufficiency (FVI) were all regarded as VE. FVI was defined as below:
• No reflux or occlusion in the deep veins, saphenous veins, accessory saphenous veins, or perforators on duplex venous ultrasound • Confirmed severe gait disturbance and/or prolonged sitting due to joint problems, general weakness, obesity, and so on • No other edemagenic conditions, for example, cardiac/hepatic/renal failure
In the current study, LE complicated by apparent venous disorders was excluded. The clinical severity of LE was judged according to the Consensus Document of the International Society of Lymphology 10 as follows:
Stage 0: A latent or subclinical condition in which limb swelling is not yet evident.
Stage I: An early accumulation of fluid that subsides with limb elevation.
Stage II: Tissue swelling that is not reduced by limb elevation alone. Pitting manifests in earlier stage II, but the limb may or may not pit in later stage II as excess fat and fibrosis supervene.
Stage III: Lymphostatic elephantiasis in which pitting can be absent and trophic skin changes such as acanthosis, further deposition of fat and fibrosis, and watery overgrowths have developed.
An asymptomatic contralateral leg with unilateral LE might be regarded as Stage 0 LE because the leg could have reduced lymph transport due to intrapelvic lymph node dissection in secondary LE or possible congenital abnormality in primary LE. However, they were excluded from the analysis because these legs had no edema. Participant characteristics are summarized in Table 1.
p < 0.05 versus normal.
0.05 versus venous edema.
BMI, body mass index; FVI, functional venous insufficiency; PTS, post-thrombotic syndrome; PVI, primary venous insufficiency.
A bioimpedance spectrometer (U-400; Impedimed Ltd, Brisbane, Australia) was used for BIA. All assessments were performed between 11 a.m. and 3 p.m. Assessment within 1 hour after a meal and/or exercise was avoided. Participants were set supine in a room maintained at 25°C, and the skin was degreased using alcohol swabs before the attachment of electrodes. Specially designed electrodes that could be used both for current drive and voltage sensing were attached on the dorsal wrists and the anterior surface of the leg at three levels (ankle, upper edge of the patella, groin) for three protocols as below:
Protocol 1: This was performed in patients with unilateral leg edema and normal subjects only. The impedance in a leg with edema (or the right leg in normal subjects) normalized to the contralateral normal leg (or the left leg in normal subjects) was obtained.
Protocol 2: This was performed in all participants. The impedance in each leg normalized to the right arm was obtained.
Protocol 3: This was performed in all participants. The impedances in the thigh and calf without normalization were separately obtained.
Protocol 1 and 2 were performed using the standard equipotential electrode arrangement. Detailed electrode positions in Protocol 3 are demonstrated in Figure 1.

Electrode positions in Protocol 3. The electrode position at the ankle was the same with that used in the standard equipotential electrode arrangement. At the knee level, the middle of the electrode was placed at the level of upper edge of patella, but it was attached slightly medial to the patella. At the groin level, the electrode was placed just below the crease of the front aspect of the groin. However, in the subjects with small stature, this was sometimes needed to be shifted proximally to keep interelectrode distance >20 cm.
Statistical analyses
The results are expressed as mean ± standard deviation or count, unless otherwise indicated. Simple linear regression analysis was used to study the correlation between R i /R e obtained by different methods and to test the correlation between R i /R e and the sum of R i /R e for the thigh and calf. To test for differences in subject characteristics and differences in R i /R e , R i , and R e in legs with various conditions, the Kruskal–Wallis test was used. The Mann–Whitney U-test was used for multiple comparisons. Statistical analyses were performed using JMP 11.0 (SAS Institute, Cary, NC). A p-value <0.05 was considered significant.
Results
The currently used BIA device was originally designed to calculate R i and R e of a leg normalized to the contralateral leg, which is essentially applicable only to unilateral edema. To obtain R i and R e of both legs, we tried to use the right arm for normalization and to verify whether the method is valid. R i /R e of a leg normalized to the contralateral leg (R i /Re leg (cont)) and that normalized to the right arm (Ri/Re leg (rarm)) were compared in patients with unilateral leg edema (tested leg = diseased leg, n = 37) and in normal subjects (tested leg = right leg, n = 33). A good linear correlation between Ri/Re leg (cont) and Ri/Re leg (rarm) was obtained both in patients with unilateral leg edema (R2 = 0.97, p < 0.0001) and in normal subjects (R2 = 0.84, p < 0.0001) (Fig. 2). The regression lines obtained from these legs were very similar. Accordingly, it seemed reasonable to compare edematous legs and normal legs directly using R i /Re leg (rarm) instead of Ri/Re (cont). Among the current study groups, no significant differences were observed in terms of sex and limb dominance, while significant differences were observed in terms of age, physique, edema laterality, and treatment status, which might affect the results according to a report by Ward et al. 3 However, we decided to use R i /R e leg (rarm) as a guide for fluid volume status regardless of these factors, because these were directly and/or indirectly related to the nature of the diseases.
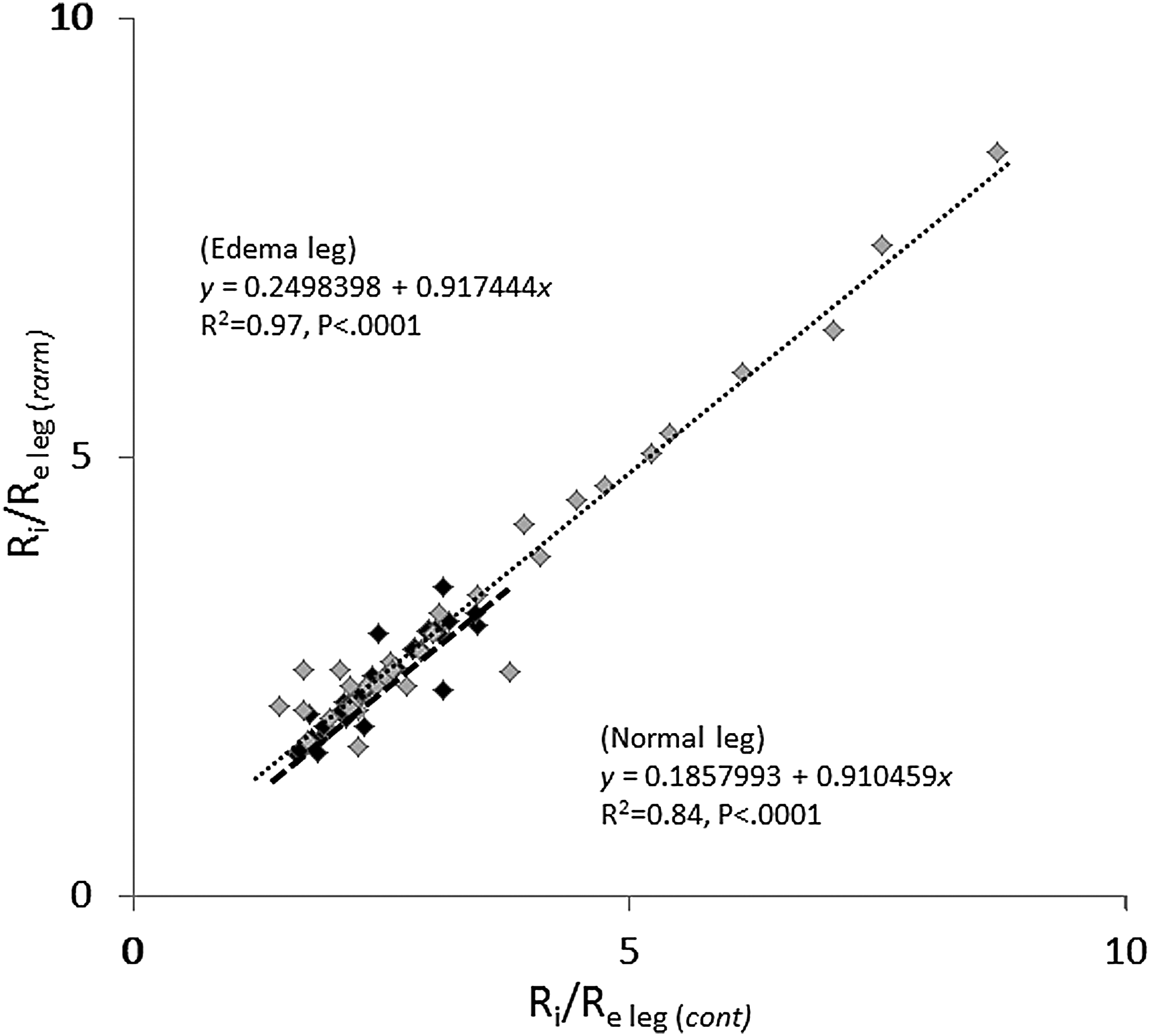
Correlation between R i /R e of a leg normalized to the contralateral leg (R i /R e leg (cont) ) and that normalized to the right arm (R i /R e leg (rarm) ) in patients with unilateral leg edema and normal subjects.
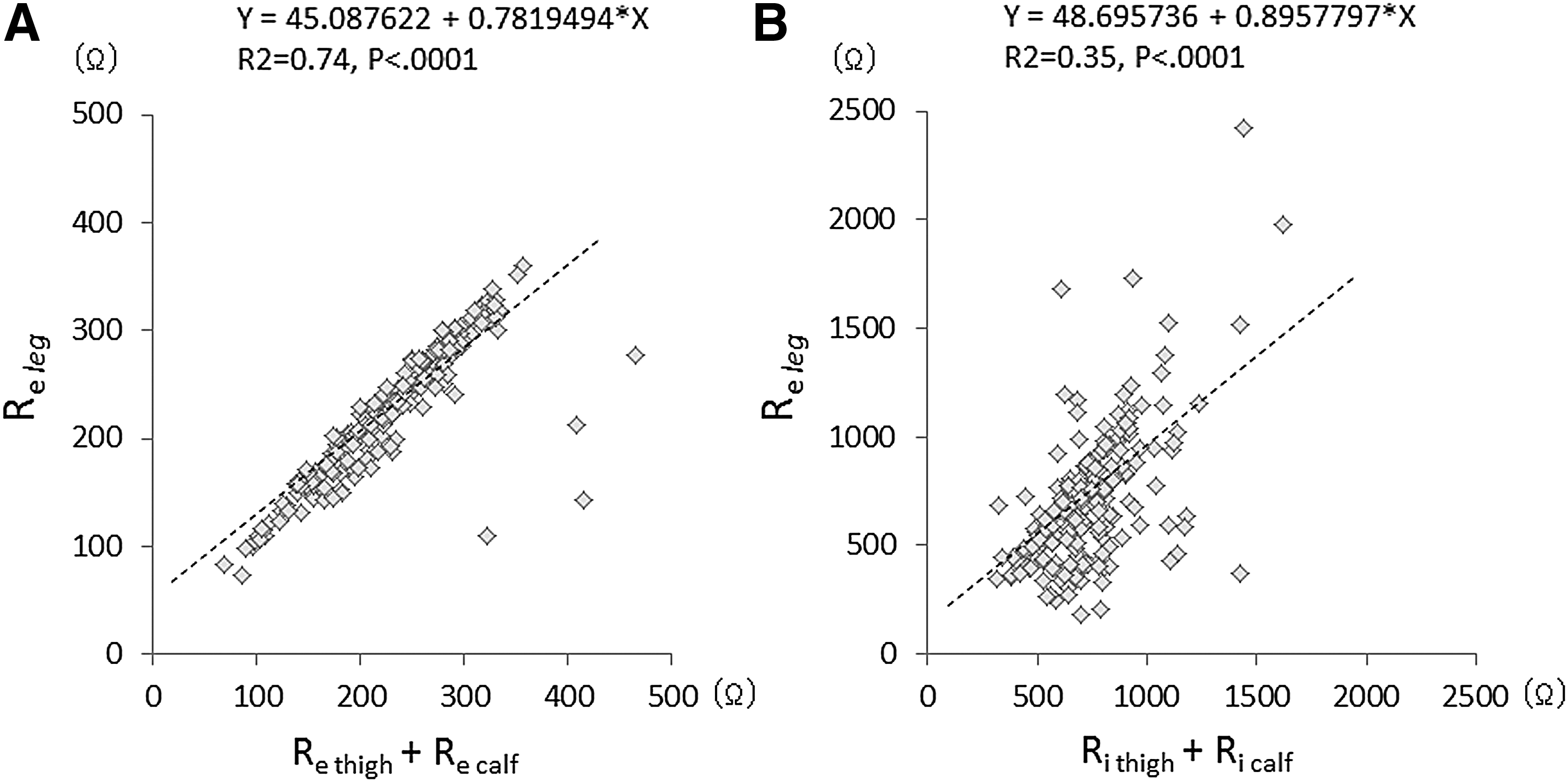
Next, we measured the extracellular and intracellular impedances of thigh (R e thigh , R i thigh ) and calf (R e calf , R i calf ), respectively, and correlated them with those of the whole leg (R e leg , R i leg ). Theoretically, R e leg and R i leg each should be equal to the sum of R e thigh and R e calf , and R i thigh and R i calf , respectively. This was roughly true both in the thigh (R2 = 0.74, p < 0.0001) and calf (R2 = 0.35, p < 0.0001), although a certain range of deviation was observed (Fig. 3). Therefore, it seemed acceptable to divide the whole leg impedance into the impedances of thigh and calf for analysis.
BIA in legs with VE, LE, and normal legs
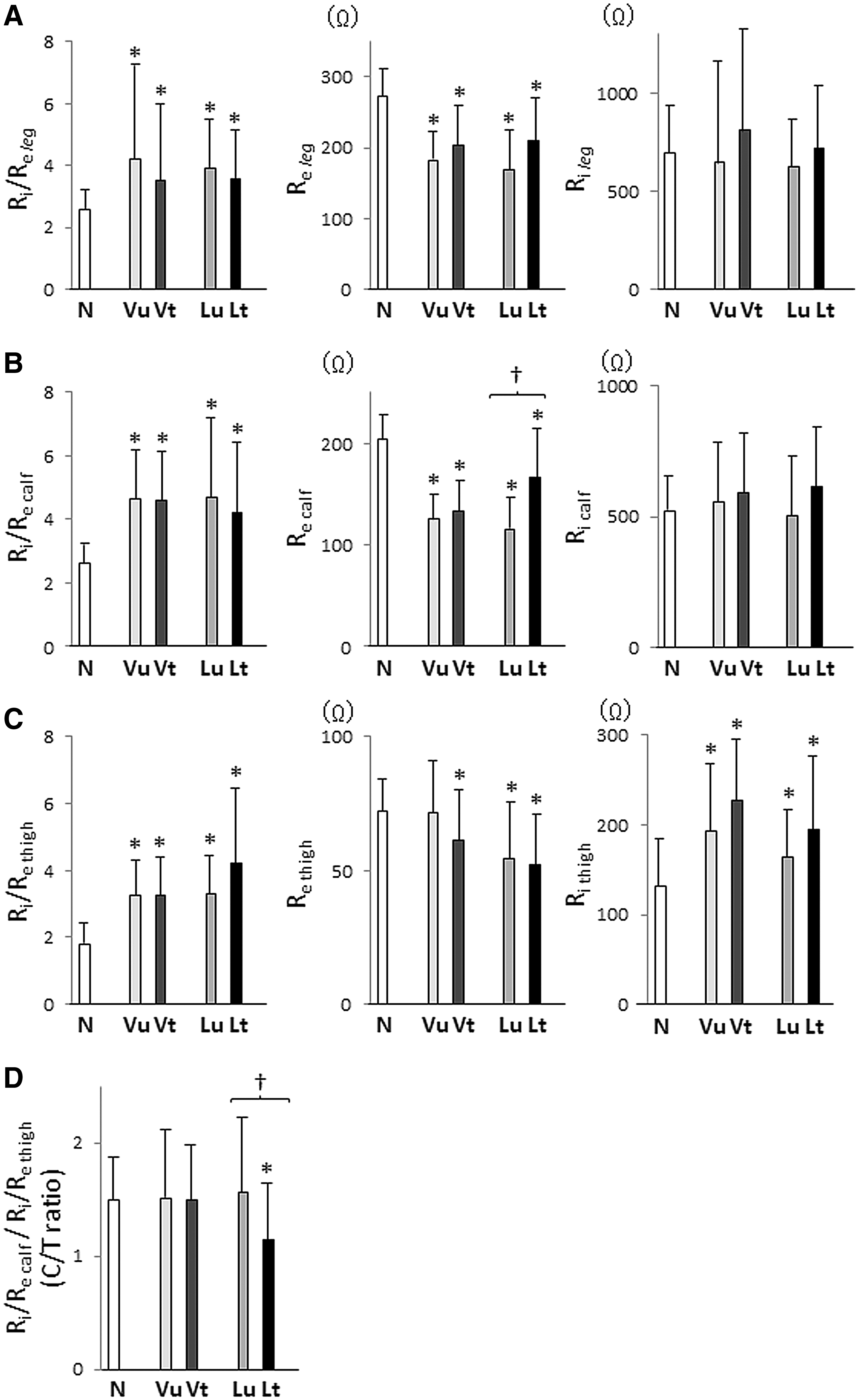
The results showed that R i /R e leg , a surrogate parameter for ECF/ICF of a whole leg, was increased both in VE and LE compared to that in N (N 2.5 ± 0.7, VE 3.9 ± 3.7, LE 3.7 ± 1.5), and this was true regardless of treatment status (Fig. 4A left). Since R i leg was similar among these legs (Fig. 4A right), this increase in R i /R e leg was considered to be caused by a decrease in R e leg (Fig. 4A middle). When the thigh and calf were separately evaluated, the same phenomenon was confirmed in the calf. Namely, R i /R e calf was increased in legs with edema (N 2.6 ± 0.6, VE 4.6 ± 1.7, LE 4.4 ± 2.2); this was true regardless of treatment status (Fig. 4B left), due to a decrease in R e calf (Fig. 4B middle), while R i calf in these legs was similar (Fig. 4B right). In the thigh, an increase in R i /R e thigh was again confirmed in legs with edema (N 1.8 ± 0.5, VE 3.2 ± 3.8, LE 3.8 ± 1.9). However, this was slightly affected by treatment status (Fig. 4C left). R e thigh was decreased in treated VE, and a further decrease was observed in treated/untreated LE (Fig. 4C middle). In contrast to the calf, R i thigh was increased both in VE and LE compared to N (Fig. 4C right). The ratios of R i /R e calf to R i /R e thigh (C/T ratio) were compared and were almost the same in N and untreated VE/LE. A significant decrease in C/T ratio was observed between treated and untreated LE, but this was not the case in VE (Fig. 4D).
Discussion
The increase in R i /R e in the whole leg, thigh, and calf could be demonstrated in VE and LE. Moreover, it was found that C/T ratio was similarly about 1.5 in N and untreated VE/LE. This indicated that distribution of fluid in a leg according to gravity was constant regardless of fluid status in the leg. Accordingly, we could not find any particular feature in LE in terms of fluid distribution pattern.
In the current study, C/T ratio was decreased by treatment in LE, but not in VE. We previously reported that a greater decrease of fluid in the calf, which was confirmed as decreased subcutaneous echo-free space, was found compared to that in the thigh in treated LE. 9 This might be related to hosiery design, with relatively insufficient interface pressure at the thigh that could cause “the toothpaste in the toothpaste tube” phenomenon, in which fluid was squeezed by a higher compression below to a lower compression area above. In contrast, this decrease in C/T ratio was not observed in VE. One possible explanation is the nature of the disease and its treatment. With compression therapy, most VE is resolved; thus, diligent patients did not appear in the clinic because they could manage the symptoms by themselves. Since LE caused persistent leg swelling, the more diligent the patient, the more regularly he/she appeared. Therefore, it was speculated that less compliant patients and/or nonresponders had VE, while more diligent patients had LE.
Interestingly, R i was similarly increased in the thigh with VE and LE. It is known that fluid with a relatively high protein content accumulates in LE 10 and that chronic inflammation is ongoing in legs with LE and VE. 11 These might have changed the electrolyte concentration and/or capacitive resistance of the cell membrane, resulting in a change in the coefficient of resistivity.12,13 Further investigation will be needed to clarify this issue.
Limitations
Since our clinic manages a limited number of patients with leg edema, we could only assess a small numbers of legs, particularly those with untreated LE. However, as LE treatment is gaining popularity, many patients had already started some form of compression therapy before they visited our clinic. A study, including a larger number of patients, will be needed to draw definite conclusions.
Conclusion
BIA demonstrated that fluid content was increased both in legs with VE and LE, compared to N, while the mode of gravitational fluid distribution was similar among all legs. Thus, no specific finding for LE was confirmed using BIA in the present study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.