
Abstract
Abstract
Background:
It has previously been shown that the lymph drainage rate in both upper limbs is greater in women destined to develop breast cancer-related lymphedema (BCRL) than in those who do not develop BCRL, indicating a constitutive predisposition. We explored constitutive differences further by measuring the maximum lymphatic pump pressure (Ppump) and the rate of 99mTc-Nanocoll transport generated by the contractile upper limb lymphatics before and after breast cancer surgery in a group of women who were followed for 2 years to determine their eventual BCRL or non-BCRL status.
Methods and Results:
Ppump and tracer transport rate were measured by lymphatic congestion lymphoscintigraphy in the ipsilateral upper limb in 26 women pre- and post-breast cancer surgery. BCRL occurred in 10/26 (38.5%) cases. Ppump in the women who later developed BCRL (40.0 ± 8.2 mmHg) was 1.7-fold higher than in those who did not develop BCRL (23.1 ± 10.8 mmHg, p = 0.001). Moreover, the rate of lymph tracer transport into the forearm was 2.2-fold greater in the women who later developed BCRL (p = 0.052). Surgery did not significantly reduce Ppump measured 21 weeks postsurgery, but impaired forearm tracer transport in pre-BCRL women by 58% (p = 0.047), although not in those who did not develop BCRL.
Conclusions:
Women destined to develop BCRL have higher pumping pressures and lymph transport, indicating harder-working lymphatics before cancer treatment. Axillary lymphatic damage from surgery appears to compromise lymph drainage in those women constitutively predisposed to higher lymphatic pressures and lymph transport.
Introduction
B
A striking recent finding was that women who later develop BCRL have higher lymph drainage rates in both upper limbs, in both the muscle (22%–29% higher) and subcutis (22%–50% higher), before any swelling is evident, compared with women who do not later develop BCRL. 7 The raised lymph drainage rates were observed at 7 months postsurgery, so they could have been either a systemic effect of the cancer treatment or an inherent constitutive property. To resolve this point, a recent prospective study examined breast cancer patients before the cancer surgery. Quantitative lymphoscintigraphy was performed before surgery and the patients followed for 13 months postsurgery. In 7 out of 38 patients (18%) who developed BCRL, the preoperative lymph removal rate constant k was 16% higher than in patients who did not later develop BCRL. 8 These findings, along with those of Stanton et al.6,7 and Mellor et al., 5 indicate that there are constitutive, preoperative bilateral differences in lymphatic physiology in BCRL-destined patients.
Lymphatic drainage involves active contractile pumping, both in animal models9–12 and human limbs. 13 To assess lymphatic collector vessel pump function in the upper limbs of women with established BCRL, pump function was quantified as the maximum pressure (Ppump) generated in the collector lymphatics when lymph flow was blocked by inflating a cuff around the upper arm (lymphatic congestion lymphoscintigraphy [LCL] 14 ). Ppump was found to be significantly impaired in the lymphedematous upper limb by 38% relative to healthy control subjects. Moreover, there was a strong negative correlation between Ppump and the magnitude of the swelling, that is, the weaker the pump, the greater the swelling.
To bring together many of the findings reviewed above, we proposed the following working hypothesis. 15 In pre-BCRL patients, the work of lymphatics is already high due to their raised fluid load. After axillary surgery, lymphatic pump failure may then develop in a manner analogous to cardiac failure following a chronically raised afterload (hypertension). Lymphatic afterload is probably increased chronically by axillary lymphatic damage during surgery and radiotherapy, since nodal excision raises lymph outflow resistance in sheep. 16 The chronically increased work by the lymphatic muscle fibers leads eventually to reduced lymphangion contractility, as in hypertensive heart failure; animal studies show lymphatic failure at increased distending pressures.10,17,18 The resulting decline in lymph drainage rate leads to edema in the drainage territory of the failing lymphatics. The chronic pump failure hypothesis offers a rational explanation for the variable delay in onset of BCRL, since a variable period is likely to be required for overload failure to reach a critical point. Pump failure can also offer a rational explanation for the regionality paradox15,19; if the constitutionally weakest lymphatic collector vessels fail first, swelling will be localized to their drainage territory, that is, hand, forearm, or upper arm.
In light of the constitutive preoperative differences in lymph flow in lymphedema-destined breast cancer patients, the question arose as to whether these patients might also have constitutive differences in lymphatic pump function before pump failure. The present study evaluates this possibility by measuring maximum lymphatic pump pressure Ppump, plus several secondary measures of lymphatic transport rate, in the ipsilateral upper limb of women recently diagnosed with breast cancer. The study was carried out on the ipsilateral upper limb before and after axillary lymph node surgery, and the patients were then followed for 2 years to see who did and did not develop BCRL.
Materials and Methods
Patients
Twenty-six women, aged 53 ± 12 (standard deviation [SD]) years and newly diagnosed with breast cancer, were recruited from the Breast Clinics at St George's Hospital, London; The Royal Marsden Hospital, Sutton, Surrey; and Croydon University Hospital, Croydon, Surrey, UK. The study was approved by the National Research Ethics Service Committee (reference 09/H0701/112) and by the Administration of Radioactive Substances Advisory Committee (ARSAC) (certificate number 295/3230/25986). Procedures were carried out in accordance with the Declaration of Helsinki (2013) of the World Medical Association. All patients gave written informed consent.
Details of the breast cancer and its treatment are summarized in Table 1. Patients underwent mastectomy or wide local excision and axillary lymph node clearance (ANC) surgery or SLNB, as recommended by the multidisciplinary team. All patients received adjuvant radiotherapy. Baseline upper limb assessment and LCL were performed before axillary surgery (the presurgical visit) and repeated 21 ± 15 (SD) weeks after surgery (the postsurgical visit). Diagnostic assessment for BCRL (without LCL) was performed at 13.0 ± 2.8 months and 25.0 ± 4.7 months postsurgery, and also shortly after BCRL onset in the BCRL patients. In six patients, the postsurgical LCL was not performed because the patients were unavailable or declined, but these patients were nevertheless followed to see whether or not they developed BCRL. Height was measured presurgery and weight was recorded on all visits to calculate body mass index (BMI). The breast cancer patients who later developed BCRL will be referred to as “pre-BCRL” patients, and the patients who did not develop BCRL as “non-BCRL” patients. The ipsilateral upper limb of the pre-BCRL patients was the dominant side in 40% of cases and the nondominant side in 60%; in the non-BCRL patients, the ipsilateral upper limb was the dominant side in 44% of cases and the nondominant side in 56%.
Pre-BCRL group: the patients who later developed breast cancer-related lymphedema; non-BCRL group: the patients who did not develop BCRL.
ANC, axillary lymph node clearance surgery; BCRL, breast cancer-related lymphedema; DCIS, ductal carcinoma in situ (*high-grade); ER, estrogen receptor status (positive [+], negative [–]); ICC, invasive cribriform carcinoma; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; LN, lymph node, with the number positive for cancer in brackets; M, mastectomy; NR, not recorded; SLNB, sentinel lymph node biopsy; WLE, wide local excision.
All patients received adjuvant radiotherapy.
Died.
Assessment of the upper limb for lymphedema
The upper limbs were assessed both by clinical criteria and by volume measurement. The clinical features of BCRL are evident at an early minor stage that is not readily demonstrated by whole-upper limb volume measurement, because these volumes can change with change in body mass after cancer treatment (see Results). For this reason, the diagnosis of BCRL was made clinically, rather than on upper limb volumes per se. A Lymphedema Practitioner independently confirmed the diagnosis of BCRL in every patient. Clinical assessment was performed as previously described. 20 Briefly, BCRL was considered to be present if any of the following were detectable: (i) decreased visibility of subcutaneous veins on the ventral forearm and dorsal hand; (ii) smoothing or fullness of the medial elbow and distal upper arm contours; (iii) increased skin and subcutis thickness if the tissues are pinched between finger and thumb; and (iv) pitting edema upon application of thumb pressure for 60 seconds. In addition, the thickness of the posterior axillary fold (PAF) was assessed by the “pinch test.” 21 Patients with ipsilateral PAF thickening also had upper limb edema. In addition to the clinical assessment, the volume of each upper limb was measured between the ulnar styloid process (wrist) and anterior axillary fold (proximal upper arm) using an optoelectronic limb volumeter (Perometer 350S; Pero-System Messgeräte GmbH). 22
Lymphatic congestion lymphoscintigraphy
LCL was performed as described, 14 with minor changes (below). To check the efficacy of tissue compression by the upper arm congestion cuff, preliminary experiments were performed, in which antecubital venous pressure (Pv) was compared directly with the applied cuff pressure (Pcuff) in the upper limb of six healthy participants. The participant reclined on a bed with the forearm at heart level. A cannula (Venflon 18G) was inserted into the antecubital vein and connected through fine bore tubing containing heparinized saline to a calibrated pressure transducer (SensoNor dome transducer and BPM-832 pressure amplifier; Linton Instrumentation). Pv was displayed on a computer-based data recording system (PowerLab 4/30 and LabChart, ADInstruments; PMS Ltd.). A standard blood pressure (BP) cuff around the upper arm was inflated in a series of steps over the range 22–46 mmHg. Pv increased in parallel with the increases in Pcuff, although with absolute values 2.9–3.1 mmHg less than Pcuff. These results showed that the congesting cuff pressures were transmitted to the deeper tissues with minor attenuation, in accordance with the routine use of congesting cuffs to measure arterial BP.
For the LCL study, the patient lay supine on a bed and the brachial artery BP was measured by auscultation from the contralateral upper limb using a mercury sphygmomanometer and a Riva-Rocci congestion cuff (AC Cossor & Son Ltd.). For two patients with particularly big upper limbs, the larger alternative cuff size was used and the standard size for all others. The cuff was secured around the ipsilateral upper arm with the tubing at the top and the cuff bladder centered anteriorly. The cuff was wrapped closely and evenly around the limb and the overlap fastened down with adhesive tape. The sphygmomanometer was then reattached to the cuff. The upper limb was supported so that the forearm was horizontal and at heart level. The gamma camera (Argus Epic; MIC Ltd.) (128 × 128 matrix, low-energy general purpose collimator) was positioned above the ipsilateral upper limb for ventral viewing, with the forearm, upper arm, axilla, and adjacent part of the trunk within the field of view. Patients acclimatized to their surroundings for 45 minutes, including 20 minutes while lying down before the tracer injection and scan. The ambient laboratory temperature was 24.0 ± 0.6 (SD)°C (n = 26) on the presurgical visit and 23.8 ± 0.6°C (n = 20) postsurgery. Skin temperature, recorded from the ipsilateral forearm (YSI 4600 Digital Thermometer; Henleys Medical Supplies Ltd.), was 29.6 ± 1.3°C presurgery and 29.5 ± 1.5°C postsurgery.
The cuff was inflated to 60 mmHg (or 50 mmHg if the diastolic BP was <60 mmHg), using the sphygmomanometer. After 2 minutes of congestion, 50 μL of 99mTc-Nanocoll (GE Healthcare) of activity 8.4 ± 1.6 MBq (n = 26) was injected intradermally between the second and third metacarpal heads of the ipsilateral hand, using a microneedle of outer diameter 0.2 mm (Unimed SA). The effective dose was 0.03 mSv. The injections were performed consistently and by the same operator throughout, taking on average 52 ± 13 seconds (n = 26) to complete. The injected activity was 8.1 ± 1.5 MBq and the duration of the injection was 57 ± 16 seconds for the pre-BCRL group and 8.6 ± 1.6 MBq and 49 ± 11 seconds for the non-BCRL group (n = 10 and 16, p = 0.41 and 0.18, unpaired t-tests). Lymphatic density is higher in the dermis than subcutis, so dermal injections provide rapid access of the tracer to the upper limb collector lymphatics for gamma camera imaging.23–25 Lymphatic vessels are not readily imaged following intramuscular administration of radiotracer in the upper limb. 26 99mTc-Nanocoll was used as the lymphatic tracer instead of Technescan HIG (human IgG), used formerly, 14 because Technescan HIG had been withdrawn from the market by the sole manufacturer. Radiochemical purity of the 99mTc-Nanocoll was ≥95%.
Following injection, dynamic imaging was performed at a frame rate of 2.5 minutes for 70 minutes. The cuff pressure (Pcuff) was held at 60 mmHg for 10 minutes, a period long enough to demonstrate trapped tracer unable to pass beyond the lower border of the cuff. Pcuff was then deflated in 10 mmHg steps every 10 minutes until Pcuff = 0 mmHg. In a further static image acquired after completion of the dynamic sequence while the patient remained in position, outline representations of the forearm, cuff, and shoulder regions were traced onto the camera face using a 57Co pen marker (High Technology Sources Ltd.); the regions thus delineated were used to create templates for the region of interest analysis of the dynamic images (see below). The syringe activity was measured before and after injection using the gamma camera, to calculate the injected activity. No blood samples were collected.
Measurement of lymphatic function
Three regions of interest (ROI) were analyzed, namely the forearm (ROI1), the subcuff region of the upper arm (ROI2), and the axillary-supraclavicular region (ROI3) (Fig. 1). The counts from each 2.5-minute acquisition were plotted against time for each ROI. At high cuff pressures, the tracer was transported into the forearm and on toward the lower border of the cuff, but was unable to move more proximally because the lymphatic pump was unable to generate sufficient pressure to overcome the cuff pressure. As cuff pressure was reduced, there came a point at which lymphatic pressure was high enough to force tracer under the cuff and into the axilla.

Lymphatic congestion lymphoscintigraphy performed before axillary surgery on the ipsilateral upper limb of a patient who later developed breast cancer-related lymphedema. Three regions of interest (ROI1 [the lowermost ROI], forearm; ROI2, subcuff; and ROI3, axilla) are superimposed and the number of minutes elapsed since the injection are shown.
Primary measure of lymphatic function, Ppump (mmHg)
Ppump was defined as the Pcuff at which radioactivity in ROI3 (axilla) first exceeds the background level (the lymphatic pump pressure). 14
Secondary indices of lymphatic transport
The secondary indices of lymphatic transport, derived using fractional counts (local counts divided by injected activity), were (1) the rate of rise of 99mTc-Nanocoll activity in ROI1 during the initial 2.5–10.0 minute period of trapped lymph (dA/dtROI1, min−1); (2) the maximum 99mTc-Nanocoll count in ROI1; and (3) the rate of rise of 99mTc-Nanocoll activity in ROI3 over the virtually linear 20-minute segment of the counts-versus-time plot after Ppump exceeded Pcuff (dA/dtROI3, min−1). Linear transport occurred at 35–55 minutes for the pre-BCRL group and 42.5–62.5 minutes for the non-BCRL group. All activities were corrected for physical decay of the radionuclide with standardization to time of injection.
Statistical analysis
Results are presented as the mean ± SD in the text and as the mean ± standard error of the mean (SEM) in the tables and figures. The normality of data sets was tested using the D'Agostino-Pearson Omnibus test. Student's paired or unpaired t-test was used to compare differences between groups, or the Mann–Whitney test in the case of non-Gaussian distribution (comparison of Ppump in the pre-BCRL and non-BCRL groups). The foregoing together with linear regression and two-way analysis of variance (ANOVA) were as implemented in GraphPad Prism version 6 (GraphPad Software). Differences were considered significant if p ≈ 0.05 or less.
Results
Clinical, surgical, and morphometric data
Incidence of BCRL and cancer treatment
BCRL was diagnosed clinically in 10/26 women (38.5%), with onset at 7 ± 4 months (0–12 months) postsurgery. BCRL developed in 7/14 (50.0%) patients undergoing mastectomy, 3/12 (25.0%) patients undergoing wide local excision, 9/20 (45.0%) patients undergoing ANC, and 1/6 (16.7%) undergoing SLNB. The number of lymph nodes removed in the pre-BCRL group, 16.0 ± 9.3 per patient, was not significantly different from non-BCRL, 13.3 ± 10.5 (p = 0.52, unpaired t-test). The number of removed nodes that were positive for cancer was again similar in the two groups (4.5 ± 3.5 pre-BCRL versus 3.3 ± 4.2 non-BCRL, p = 0.46).
Upper limb volumes
Before surgery, both the ipsilateral and contralateral upper limb volumes for the pre-BCRL group were greater than for the non-BCRL group, by 22.1% (p = 0.055, unpaired t-test; Table 2) and 21.5%, respectively (p = 0.054). Surgery had no statistically significant early (i.e., at mean 21 weeks) effect on upper limb volume in either the pre-BCRL or non-BCRL group (Table 2; p = 0.31 and 0.48 for pre-BCRL ipsilateral and contralateral upper limbs, respectively; p = 0.80 and 0.64 for non-BCRL, paired t-tests). The above analysis hides a significant difference, however; after surgery, ipsilateral volume was significantly greater than contralateral volume in the pre-BCRL patients (p = 0.040), due to small divergent changes; there was a small increase in ipsilateral volume (not itself statistically significant) and a small fall in contralateral volume (not itself statistically significant), resulting in a significant difference between the upper limbs (Fig. 2). Over 2 years, ipsilateral upper limb volume tended to increase with time in the pre-BCRL group, as expected, but not in the non-BCRL group or contralateral upper limbs in either group. In some cases, the increase in ipsilateral upper limb volume was very small, especially at the time of diagnosis, emphasizing the importance of using clinical criteria to diagnose early BCRL. 20
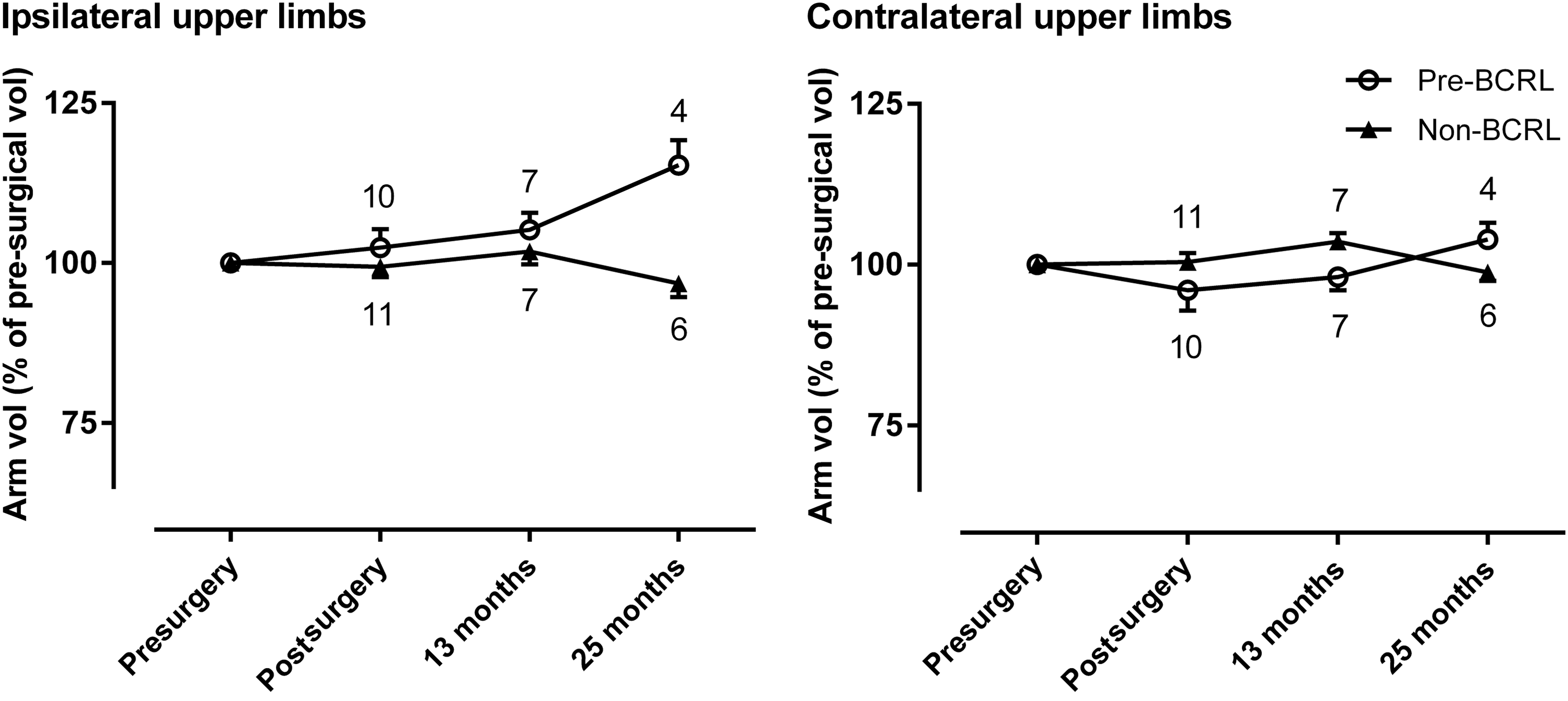
Changes in ipsilateral and contralateral upper limb volume following axillary surgery for the pre-BCRL and non-BCRL patients relative to their presurgical volumes ( = 100%). Mean ± SEM, with the number of patients shown above each point. The postsurgical measurement was at 21 weeks. BCRL, breast cancer-related lymphedema.
Number of patients in each group shown in brackets; values are mean ± SEM. In both groups, neither the ipsilateral nor the contralateral limb changed significantly in volume by 21 weeks postsurgery.
p, comparison of the pre-BCRL and non-BCRL groups (unpaired t-test).
p, comparison of the ipsilateral and contralateral upper limbs (paired t-test).
BCRL, breast cancer-related lymphedema.
Body mass index
Before surgery, the pre-BCRL group's mean BMI (29.5 ± 5.0 kg/m2) was 17% higher compared with the non-BCRL group (25.2 ± 3.7 kg/m2) (p = 0.059), in keeping with their 22% greater upper limb volumes. Higher BMI is a known risk factor for BCRL1,27; our data indicate that upper limb volume is also a risk factor. BMI did not change significantly up to 25 months postsurgery (p = 0.94 for time points, two-way ANOVA).
Tracer movement along the lymphatic system of the upper limb
Representative images from a dynamic scan of a pre-BCRL presurgical patient are shown in Figure 1. The radiotracer entered the hand and forearm lymphatics rapidly, in some cases while the injection was still in progress (<1 minute). After the injection was complete, the tracer traversed the distance from the hand depot to the distal border of the cuff (mean distance 30.4 cm) at a velocity of 7.2 ± 4.3 cm/min (n = 26). Up to 3 (mean 1.6) lymph tracks were imaged in the forearm during presurgical LCL and 1–4 (mean 1.7) tracks during the postsurgical LCL. Dermal rerouting of lymph drainage was not evident in any patient either pre- or postsurgery. Tracer accumulated at the distal border of the congestion cuff until the pressure in the cuff was lowered sufficiently to allow tracer to pass under the cuff (ROI2) and into the axilla (ROI3).
Comparison of lymphatic function in the pre-BCRL and non-BCRL patients before surgery
Ppump before surgery
Maximum lymphatic pump pressure in the pre-BCRL and non-BCRL groups was compared at the presurgical time point to test the hypothesis that there is an early constitutive difference in lymphatic pumping in pre-BCRL women. Individual Ppump values are plotted in Figure 3. Ppump in the pre-BCRL group (40.0 ± 8.2 mmHg) was on average 73% higher than Ppump in the non-BCRL group (23.1 ± 10.8 mmHg, n = 10 and 16; p = 0.0007, Mann–Whitney test). A bimodal distribution of Ppump has been reported previously in healthy individuals. 14 It is interesting to note that when the Ppump values of both pre- and non-BCRL groups are pooled, a bimodal distribution is evident (Fig. 3, right array). This raises the possibility that two human populations, with high and low Ppump, respectively, account for the bimodality in the data of Modi et al. 14
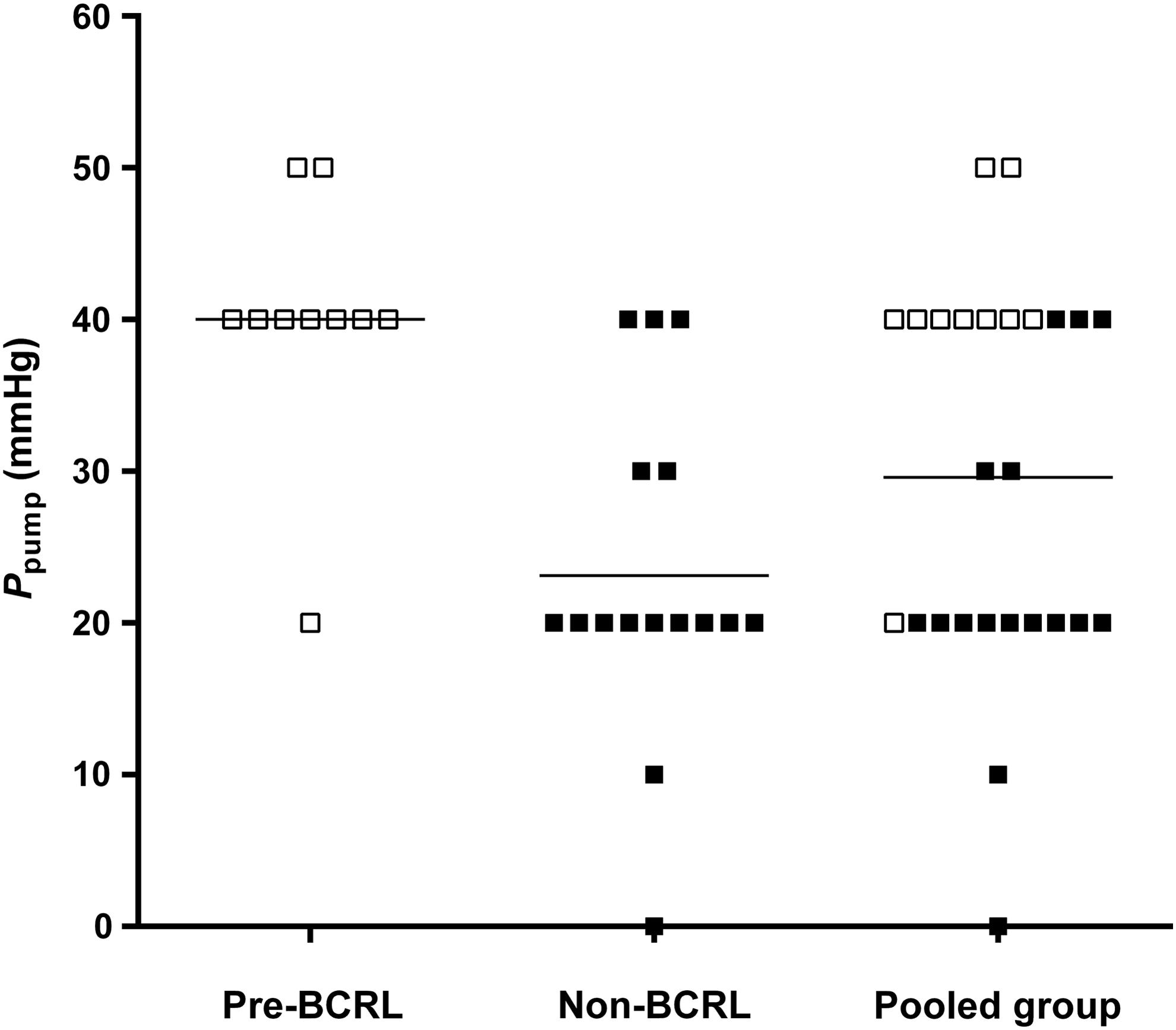
Lymphatic pump pressure (Ppump) in collector lymphatics of the ipsilateral upper limb in breast cancer patients measured before axillary surgery. The 10 pre-BCRL and 16 non-BCRL patients are shown separately (left and center arrays). Ppump for the pooled group of the 26 patients (right array) shows a bimodal distribution. The horizontal lines indicate the mean (40.0, 23.1, and 29.6 mmHg, respectively). Ppump was highly significantly greater in the pre-BCRL patients than the non-BCRL patients (p = 0.0007, n = 10 and 16, Mann–Whitney test).
Lymphatic transport dynamics before surgery
There were large differences in the lymphatic transport of 99mTc-Nanocoll between the two groups before surgery. These are illustrated in Figure 4A, B, which shows the time courses of activity in each of the three ROIs over the duration of the 70-minute scan. Several features distinguished the pre-BCRL from the non-BCRL group. (i) The rate of rise of tracer activity in ROI1 during the initial trapped lymph phase (2.5–10.0 minutes), dA/dtROI1, was faster in the pre-BCRL patients that in the non-BCRL patients. (ii) The peak accumulated activity in ROI1 during the trapped lymph phase was higher in pre-BCRL than non-BCRL patients. (iii) The rate of rise activity in ROI3 after tracer began to be pumped beyond the cuff, dA/dtROI3, was faster in pre-BCRL than non-BCRL patients. Data analysis (Table 3) showed that dA/dtROI1 for pre-BCRL patients was approximately double than for non-BCRL patients (p = 0.052) and dA/dtROI3 for pre-BCRL patients was 1.55 times higher than for non-BCRL patients (p < 0.0001). All four measures of lymphatic function were thus consistent with a more active lymphatic pump in pre-BCRL patients compared with non-BCRL patients.
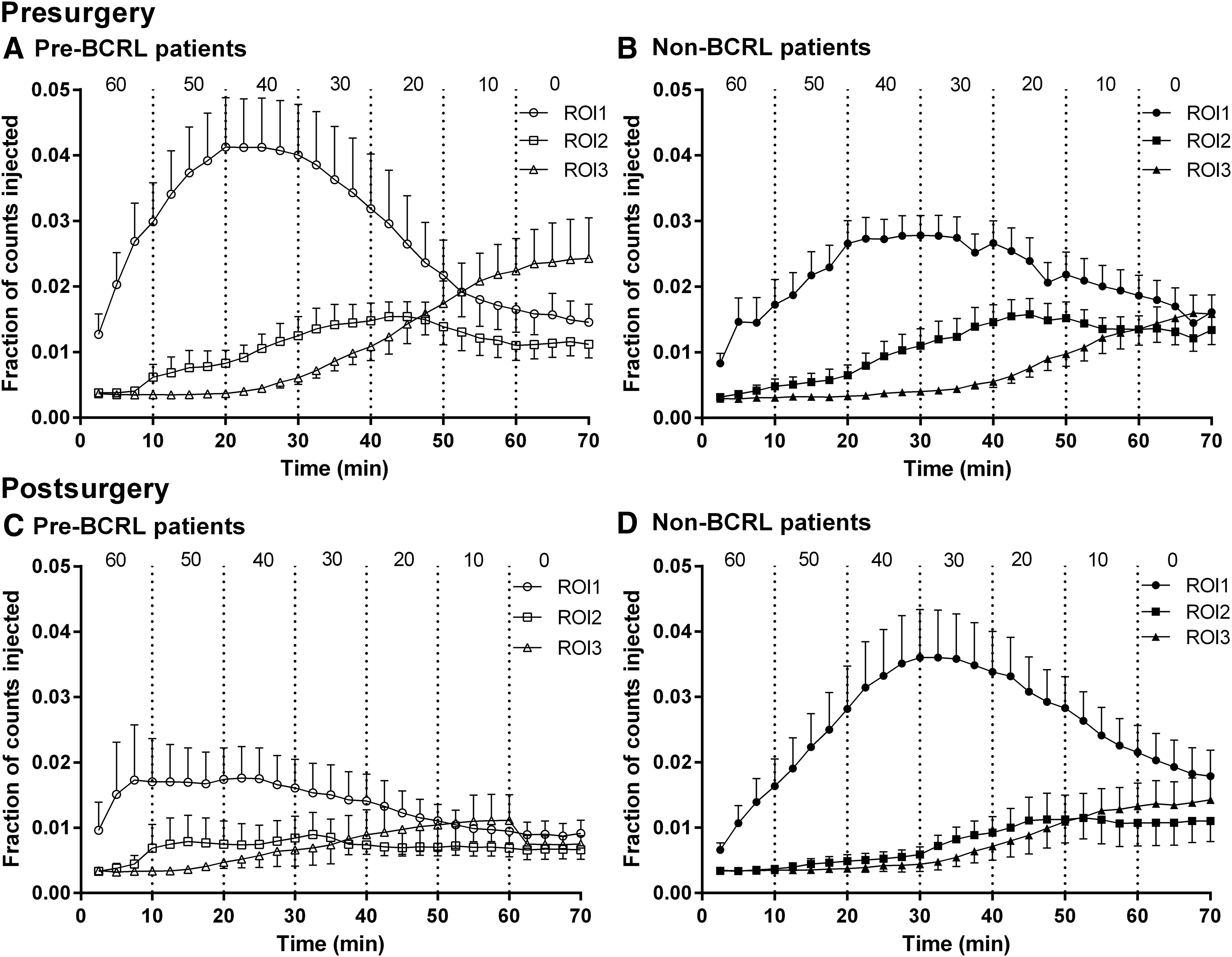
Radioactive counts recorded from three ROIs in the ipsilateral upper limb during lymphatic congestion lymphoscintigraphy and plotted as a fraction of the injected activity (mean ± SEM) against time since injection. ROI1, forearm; ROI2, subcuff; ROI3, axilla. The cuff pressure (Pcuff) in mmHg is shown above each time interval.
Number of patients in each group shown in brackets; values are mean ± SEM.
Ppump, lymphatic pump pressure; ROI, region of interest; dA/dtROI1, rate of rise of fractional count in ROI1 ( × 103) determined by linear regression analysis of mean fractional counts over 2.5–10.0 minutes (pre-BCRL and non-BCRL, ±SE); dA/dtROI3, rate of rise of fractional count in ROI3 ( × 103) by linear regression analysis of mean fractional counts over 35–55 minutes (pre-BCRL) or 42.5–62.5 minutes (non-BCRL) (±SE); Peak countROI1, maximum fractional count in ROI1 ( × 103).
p, comparisons of the pre-BCRL group with the non-BCRL group, before or after surgery (*Mann–Whitney test; comparison of regression slopes for dA/dt; unpaired t-test for the other comparisons). See text and Figure 5 for presurgery versus postsurgery statistical comparisons.
BCRL, breast cancer-related lymphedema.
Comparison of lymphatic function before and soon after surgery
Pre-BCRL patients, before versus soon after surgery
The marginal decline in Ppump from 40.0 ± 8.2 mmHg before surgery to 36.7 ± 10.0 mmHg at 21 weeks after surgery was not statistically significant (n = 9 pairs, p = 0.50, paired t-test). By contrast, the indices of lymphatic transport in pre-BCRL patients were all significantly lower at 21 weeks postsurgery (Fig. 4A versus 4C, Fig. 5). During the trapped-lymph phase, dA/dtROI1 postsurgery fell to 42% of its presurgery level (p = 0.047, comparison of slopes) and the maximum count in ROI1 fell to 51% of the presurgery level (p = 0.025, n = 9, paired t-test). When cuff pressure was lower than lymph pressure, dA/dtROI3 postsurgery fell to 27% of the presurgery level (p < 0.0001, comparison of slopes).
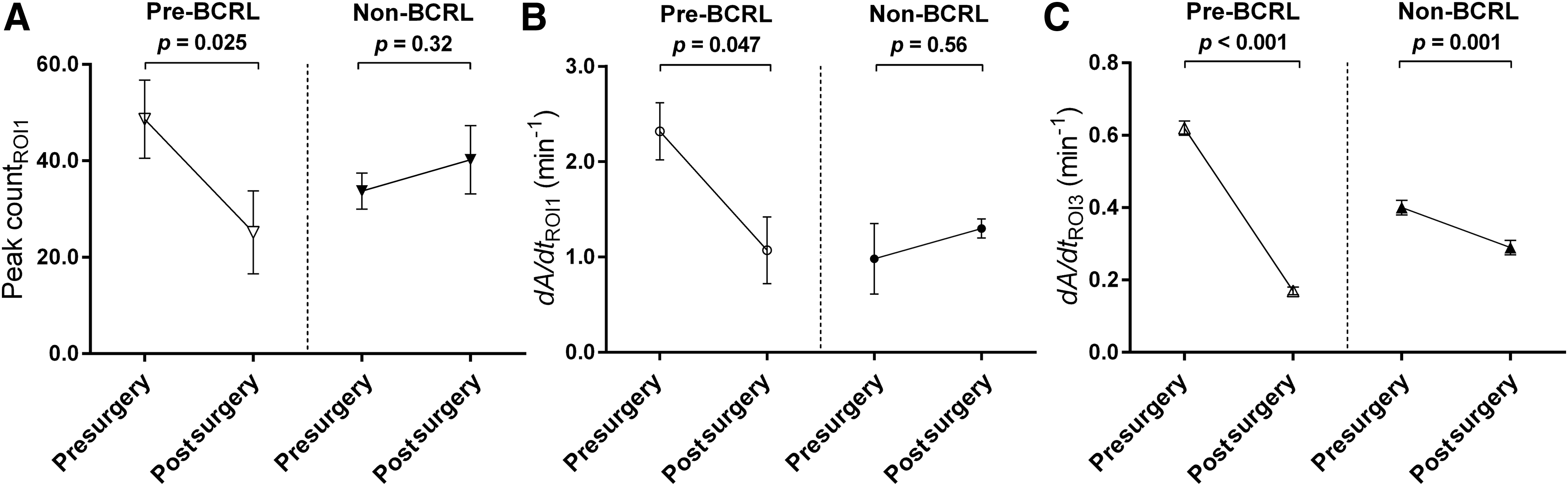
The effect of surgery on 99mTc-Nanocoll accumulation in the ipsilateral upper limb at 21 weeks after surgery in pre-BCRL and non-BCRL patients. Mean ± SEM, all values × 103.
Non-BCRL patients, before versus soon after surgery
Surgery had much less effect on the lymphatic system in non-BCRL patients than in pre-BCRL patients. Ppump was well maintained at 21 weeks after surgery in the non-BCRL patients (presurgery 23.1 ± 10.8 mmHg, postsurgery 24.5 ± 11.3 mmHg; n = 11 pairs, p = 0.78, paired t-test). The two lymphatic transport indices for ROI1 were likewise little changed postsurgery (Fig. 4B versus 4D, Fig. 5); dA/dtROI1 was not reduced (21% increase not significant, p = 0.56) and the maximum count in ROI1 was not reduced (20% increase not significant, p = 0.32, n = 11). dA/dtROI3 declined postsurgery, by 28% (p = 0.0008), but this was a relatively small change compared with the 73% fall in dA/dtROI3 in the pre-BCRL patients (Fig. 5).
Comparison of pre-BCRL versus non-BCRL group patients soon after surgery
After surgery, Ppump for the pre-BCRL group (36.7 ± 10.0 mmHg, n = 9) still exceeded that of the non-BCRL (24.5 ± 11.3 mmHg, n = 11), but the difference was smaller than before surgery (12.1 mmHg; p = 0.022, unpaired t-test). Because dA/dtROI1 in the pre-BCRL group had been greatly reduced by surgery, it was no longer higher than in the non-BCRL group (p = 0.45). The same was true for peak activity in ROI (p = 0.18). In the case of dA/dtROI3, the decrease caused by surgery in the pre-BCRL group was so large that the pre-BCRL value after surgery was significantly lower than in the non-BCRL group (p = 0.0003).
Discussion
The primary aim of this study was to test the hypothesis that women destined to develop BCRL after breast cancer treatment have constitutive differences in upper limb lymphatic physiology. The previous evidence underlying the hypothesis was summarized in the Introduction and included raised lymph flows in pre-BCRL women.7,8 The present data, obtained before axillary lymph node surgery or radiotherapy, support the hypothesis; the results showed highly significant differences in lymphatic pump pressure and lymph tracer transport between those who later developed BCRL and those who did not. Moreover, the data indicate a more active, not weaker lymphatic system in the pre-BCRL women. By contrast, once long-standing lymphedema is present (mean 7.4 years), Ppump is reduced, indicating a weakened lymphatic pump. 14 The second main finding was that although the breast cancer treatment did not cause a significant early (21-week) fall in lymphatic pump pressure, it did cause striking reductions in forearm lymph transport rates in the pre-BCRL patients, with relatively little effect in non-BCRL patients. Thus, whereas a marked fall in pump pressure is a later event in lymphedema development, 14 our new results reveal evidence of impaired lymphatic transport rates within 5 months of treatment.
Upper limb volumes, incidence of BCRL, and risk factors
We applied strict clinical criteria, developed previously, for the diagnosis of BCRL. 20 The diagnosis of early mild BCRL based purely on volume measurement can be confounded by other factors, such as weight change, that affect upper limb size.28,29 The incidence of BCRL (38.5%) is within the range reported in recent studies; meta-analysis of nine prospective cohort studies gives an incidence of BCRL diagnosed by more than one method of 28.2% (mean; range 11.8%–53.5%). 1 Nevertheless, the question arises as to whether 2 years' follow-up is sufficient; DiSipio et al. 1 reported that the incidence of BCRL increases up to 2 years after diagnosis or surgery (24 studies), whereas two questionnaire studies reported an increase beyond 2 years.30,31 Paskett et al. 30 reported that while the estimated prevalence (repeated episodes or continuous swelling) was 23%–29% for any assessment interval, the incidence of episodic swelling increased beyond 2 years (48% at 2 years, 54% at 3 years). Norman et al. 31 reported an increase in cumulative incidence from 30% at 2 years to 41% at 5 years. Data from objective and subjective measures of lymphedema rates can show considerable discordance. 27 In the present study, all cases of BCRL developed within 12 months of surgery and were diagnosed according to strict clinical criteria with confirmation by a Lymphedema Practitioner; no cases were diagnosed in the second year.
The study was not designed to identify risk factors for BCRL, but nevertheless showed that BCRL incidence was 2.7-fold higher in the patients receiving ANC than SLNB. ANC surgery is a known risk factor for BCRL. 27 The number of lymph nodes removed and the number positive for cancer were similar in both the pre-BCRL and non-BCRL groups. Higher BMI is an established risk factor for BCRL,1,27 and BMI was 17% higher in the pre-BCRL than the non-BCRL group; consistent with this was the 22% greater ipsilateral and contralateral upper limb volumes in the pre-BCRL group, indicating that upper limb volume is a related risk factor. It is currently unknown whether presurgical upper limb volume is an independent risk factor for BCRL.
Constitutively raised lymphatic function in the BCRL-destined group
The results in Figure 3 showed that collector lymphatics distal to the cuff in pre-BCRL patients were able to pump lymph to a higher maximum pressure than those in non-BCRL patients. Moreover, the faster dA/dtROI1 and higher maximum activity in ROI1 of pre-BCRL patients indicated a more rapid transport of lymph from the hand depot into the collector lymphatics of the forearm; and the faster dA/dtROI3 indicated a more rapid transport of lymph into the axilla after Ppump exceeded Pcuff. These findings combine to support the hypothesis of constitutively enhanced lymphatic function in women destined to develop BCRL.
LaPlace's law and the raised Ppump
What mechanism(s) might underlie the preoperative difference in Ppump between the two groups? LaPlace's law states that the pressure P generated by tension T in a thin-walled tube of radius R equals T/R. This raises the question of whether the lymphatic smooth muscle contractile force T is greater in pre-BCRL than non-BCRL patients, or whether the collector vessel radius R is smaller. Although we have no direct evidence on this point, increased lymphatic smooth muscle activity (force and/or frequency of contraction) seems the more likely explanation, because the raised dA/dtROI1 and maximum ROI1 activity indicate an increased rate of lymph transport (flow)—a finding broadly in keeping with the raised lymphatic drainage rate constant k in pre-BCRL patients reported previously. 8
Limited evidence against a smaller vessel radius comes from the observation of wider initial lymphatics in the contralateral forearms of women with BCRL compared with the forearms of non-BCRL breast cancer patients 5 ; dilated lymphatic collectors imaged in BCRL limbs (median duration 24 months) by magnetic resonance lymphangiography; 32 and (in early lymphedema) collector vessel ectasia observed in histological sections from secondary lymphedema of the leg. 33 Studies using X-ray lymphangiography have demonstrated dilated lymphatic collectors in BCRL and also following axillary dissection, but in the absence of upper limb swelling.34–36
Possible causes of raised Ppump
Assuming that the high Ppump, along with the other indices, indicates enhanced lymphatic contractile force in pre-BCRL patients, what might cause this? A possible factor is the physiological adaptation of lymphatic smooth muscle, either by hypertrophy or raised contractility, to the chronically high fluid load (preload) in pre-BCRL patients. A high fluid load is indicated by the raised lymphatic removal rate constant k in pre-BCRL patients.7,8 This is supported by the recent report of raised capillary filtration capacity in both forearms of BCRL patients relative to the forearms of matched breast cancer patients without BCRL, 37 although equivalent data from pre-BCRL patients is lacking. In addition, the findings were based on short (3–4 minutes) congestions and are contrary to results based on the classic, longer congestion method. 38 Physiological adaptation of lymphatic smooth muscle to a constitutively high resistance axillary node pathway (afterload) is an additional speculative possibility. In single lymphangions from the rat mesentery, in which input and output pressures were controlled, elevated afterload triggered a time-dependent increase in lymphatic contractility, modulated by change in preload.18,39 Genetic factors have also been related to BCRL susceptibility.40–42
Hypothesis linking raised Ppump in pre-BCRL and subnormal Ppump in established BCRL; potential key role of lymphatic collector vessel smooth muscle work
Not only is Ppump in established BCRL lower than the Ppump of normal healthy subjects but also the severity of the swelling correlates negatively with Ppump indicating that partial failure (weakening) of the collector lymphatic pump over the years contributes to the pathogenesis of BCRL. 14 The new findings in this study raise the question “why would women with intrinsically stronger lymphatic pumps than others be more prone to pump failure after surgery?” The high transport rates in the pre-BCRL patients (Fig. 4A), along with their high lymph flows7,8 offer a rational, although speculative explanation, as follows. The stroke work of a contracting lymphangion = volume of lymph ejected (ΔV) × active pressure increase (ΔP), and the lymphangion work rate = (ΔV/t) × ΔP, that is, lymph flow × ΔP. The high lymph flow in the pre-BCRL population thus imposes a chronically high work rate on the lymphatic smooth muscle. We propose that this may be close to the maximum chronically sustainable work rate. Surgical removal of lymph nodes raises the outflow resistance to lymph in sheep. 16 If the same is true in humans (perhaps exacerbated by the radiotherapy), then the previous level of lymph flow can only be maintained by a rise in ΔP (afterload), further increasing the work rate (ΔV/t) × ΔP. Over a long period, the increased work may cause a partial failure of lymphangion force generation (intrinsic smooth muscle failure) and/or vessel dilatation; the latter reduces the conversion of wall tension into pressure (LaPlace's law) and may impair lymphatic valve competence. The “lymphatic work” hypothesis has as its analogue the chronic failure of a dilated heart resulting from a high preload and raised afterload (hypertension). The majority subset of women that avoid BCRL may do so partly because their lymphatic system normally operates at a lower preload, leaving them with a greater reserve pump capacity.
Additional pathogenic factors may also come into play after pump failure, for instance, degenerative histopathological processes. A recent study described progressive histopathological changes in collector lymphatic vessels harvested from patients affected by lower limb lymphedema after the surgical removal of lymph nodes for gynecological cancers. 33 With increasing disease progression and severity, the characteristics of the normal collector lymphatics were lost. In early stage lymphedema, most lymphatic vessels were normal or showed ectasia, which by LaPlace mechanics will tend to reduce pump pressure, even if contractile force was unimpaired. A minority of vessels had a thickened wall and narrower lumen. Sclerosis was commoner and ectasia less common with increasing severity of lymphedema. Sclerosis of upper limb collector lymphatics would further impair lymphatic pumping and worsen the swelling. Severe sclerosis was observed in superficial lymphatics in the upper limb of a patient with refractory BCRL of 18 years' duration. 43 Inflammatory triggers for the above might be aggravated by the association between obesity and an abnormal inflammatory response, perhaps involving macrophage migration.44,45
Impaired lymphatic transport dynamics in pre-BCRL patients following axillary surgery
Transport into forearm from hand depot
The slight fall in pre-BCRL Ppump at 4.8 months postsurgery was not statistically significant, yet at the same time point, the lymphatic transport into the pre-BCRL forearm was roughly halved; dA/dtROI1 fell by 58%, maximum ROI1 activity by 48%. The contrast between the large fall in hand-to-forearm transport rate and relatively unchanged Ppump could be explained if the more distal contractile lymphatics (i.e., between hand depot and forearm) are weaker than proximal ones close to the cuff, which were still capable of generating a high Ppump. The data in Figure 4A versus 4C may thus be an early clue that distal lymphatics are the weakest link in the chain and begin to fail before more proximal lymphatics.
Transport into the axillary-supraclavicular region
The fall in dA/dtROI3 after surgery was much more pronounced in pre-BCRL (73% reduction) than non-BCRL patients (28% reduction), despite the relatively well maintained Ppump in the pre-BCRL group. The interpretation of dA/dtROI3 after surgery is complicated by the fact that some lymph nodes have been removed from this ROI. The reduced ROI3 transport in both pre-BCRL and non-BCRL groups may be caused partly by increased lymph drainage resistance after axillary surgery; and the greater reduction in the pre-BCRL group may be caused by the slowed delivery of 99mTc-Nanocoll by the markedly impaired forearm transport vessels (transport in series). Other possibilities include more extensive axillary lymphatic trauma from the cancer surgery or radiotherapy, 4 which the study was not designed to explore.
Limitations of present study
To test further the hypothesis of a constitutively different Ppump in pre-BCRL patients, measurements of Ppump and transport dynamics in both upper limbs would have been valuable. This was not feasible in practice because of the demands it would have placed on the patients shortly before their cancer surgery. Ppump data at 2 years, after lymphedema was established, would be useful, to check on the decline in function known to occur over several years. 14 Many aspects of the proposed working hypothesis remain speculative and call for further work. For example, we are not aware of any comparative study of lymphatic smooth muscle structure and function in the distal collectors versus proximal collectors of the human upper limb; and apparently, only one study (in sheep) has examined the effect of node removal on the hydraulic resistance to lymph transport out of a limb.
Conclusions
A disease model for BCRL emerges from the body of evidence presented in this study. Women destined to develop BCRL have constitutively higher lymph loads and higher lymphatic pumping pressures. Breast cancer treatment per se has relatively little effect on maximum lymphatic pressure generation initially, but nevertheless impairs lymph transport in those subsequently developing BCRL. Therefore, axillary lymphatic obstruction is not the sole explanation for BCRL; surgery appears to compromise lymph drainage in those women constitutively predisposed, but much less so in those women with constitutively lower lymphatic pressures and transport. In women destined to develop BCRL, the lymphatic contractile work rate is already high and if this is raised further by increased resistance to axillary drainage following cancer treatment and/or further increase in lymph load, the lymphatics are gradually tipped into chronic failure. This is analogous to high preload and high afterload cardiac failure in systemic hypertension. Reduced lymphatic pump activity then leads to overt clinical edema. The identification of women belonging to an “at-risk” group, with higher lymphatic preloads before cancer treatment, would provide an opportunity for pharmacological intervention aimed at lowering preload; this could in theory prevent BCRL if introduced early enough.
Author's Note
Follow-up is now at least three years since cancer surgery for all patients, and no further cases of BCRL have developed.
Footnotes
Acknowledgments
The authors acknowledge the support of Cancer Research UK who funded this study (grant number C19621/A11009). The authors thank the patients. The authors also thank the Breast Nurses, Research Nurses, and Lymphedema Practitioners (St George's, The Royal Marsden, and Croydon University Hospitals) for their help with recruitment and for helping the patients with lymphedema; Mr Anup Sharma and Mr Dibyesh Banerjee (Breast Unit, St George's Hospital), Ms Nicola Roche (Breast Unit, The Royal Marsden Hospital), and Miss Caroline Pogson (Breast Unit, Croydon University Hospital) for help with recruitment; Dr Susan Heenan (Radiology, St George's Hospital), Clinical Radiology Expert; Andy Irwin (Physics, St George's Hospital), Medical Physics Expert; and Jim Ballinger (Nuclear Medicine, Guy's Hospital) for advice on radiopharmaceuticals; Vernie Ramalingham (Guy's Hospital) for help with the surveillance of patients; and Mick Rogers (MIC Ltd.) for gamma camera technical support.
Author Disclosure Statement
No competing financial interests exist.