
Abstract
Abstract
Secondary lymphedema is still a worldwide problem. Symptomatic approaches to lymphedema therapy have been mainly used, with complete decongestive therapy as the cornerstone. Due to a lack of regenerative therapy, researchers have established various animal models to obtain insights into pathomechanisms and to reveal the best therapeutic option. Since the first reproducible and reliable animal model of lymphedema was reported in dogs, the technique of circumferential excision of lymphatic tissue has been translated mainly to rodents to induce secondary lymphedema. In these models, various promising pharmacological and surgical approaches have been investigated to improve secondary lymphedema therapy. Imaging modalities are crucial to detect the extent of lymphatic dysfunction and decide the best therapy. The gold standard of lymphoscintigraphy is currently limited by poor spatial resolution and lack of quantification. Animal models could help to bridge a gap in improving morphological correlation and quantifying lymphatic functionality. This review summarizes the animal models used in lymphatic research and focuses on new therapeutic options and requirements for imaging modalities to visualize the lymphatic system.
Introduction
B
Various surgical approaches have been investigated in lymphedema therapy research. For example, tissue transfer and full-thickness skin flaps have been explored, as well as microsurgical reconstruction techniques. In addition, pharmacological therapy options, such as the application of VEGF-C, hyaluronidase treatment, or stem cell therapy, have succeeded in improving lymphedema. Imaging modalities support the evaluation of lymphatic function in this disease.
Materials and Methods
An investigation was performed using the U.S. National Library of Medicine (NLM) journal citation database (Medline) using PubMed; this free resource was developed and is maintained by the National Center for Biotechnology Information (NCBI) at the NLM (Bethesda, MD). The goal was to identify literature on the topic of lymphedema and animal models using Medical Subject Headings (MeSH).
First search:
1. “lymphedema”[MeSH] and “Models, Animal”[MeSH]—183 items 2. January 1, 1995–August 1, 2015—112 items 3. Language: English—106 items 4. Exclude: filariasis, lymphedema mutation (e.g., Fox-2/SOX18), adipogenesis, articles without therapeutic approach, studies in humans, reviews, primary lymphedema, double hits—35 relevant items
A second search concentrated on surgical approaches in animal models.
Second search* (Table 1):
1. “lymphedema” AND “surgery” AND “rodents”*—106 items
2. January 1, 1995–August 1, 2015—73 items
3. Language: English—68 items
4. Exclude: same criteria as first search—15 relevant items
In conclusion, 50 relevant items were investigated in this review and additional highly relevant literature that was selected by the author was added.
Results and Discussion
Animal models of acquired lymphedema
The first successful lymphedema model was established in 1968. 5 This breakthrough concerned the circumferential excision of a dog's hind limb to achieve both superficial and deep lymphatics. To create an easy, affordable, and practicable animal model, this strategy was translated to rabbits and rodents. Currently, rodents are the most common animal models in lymphatic research, accounting for ∼80% of published models (Fig. 1).
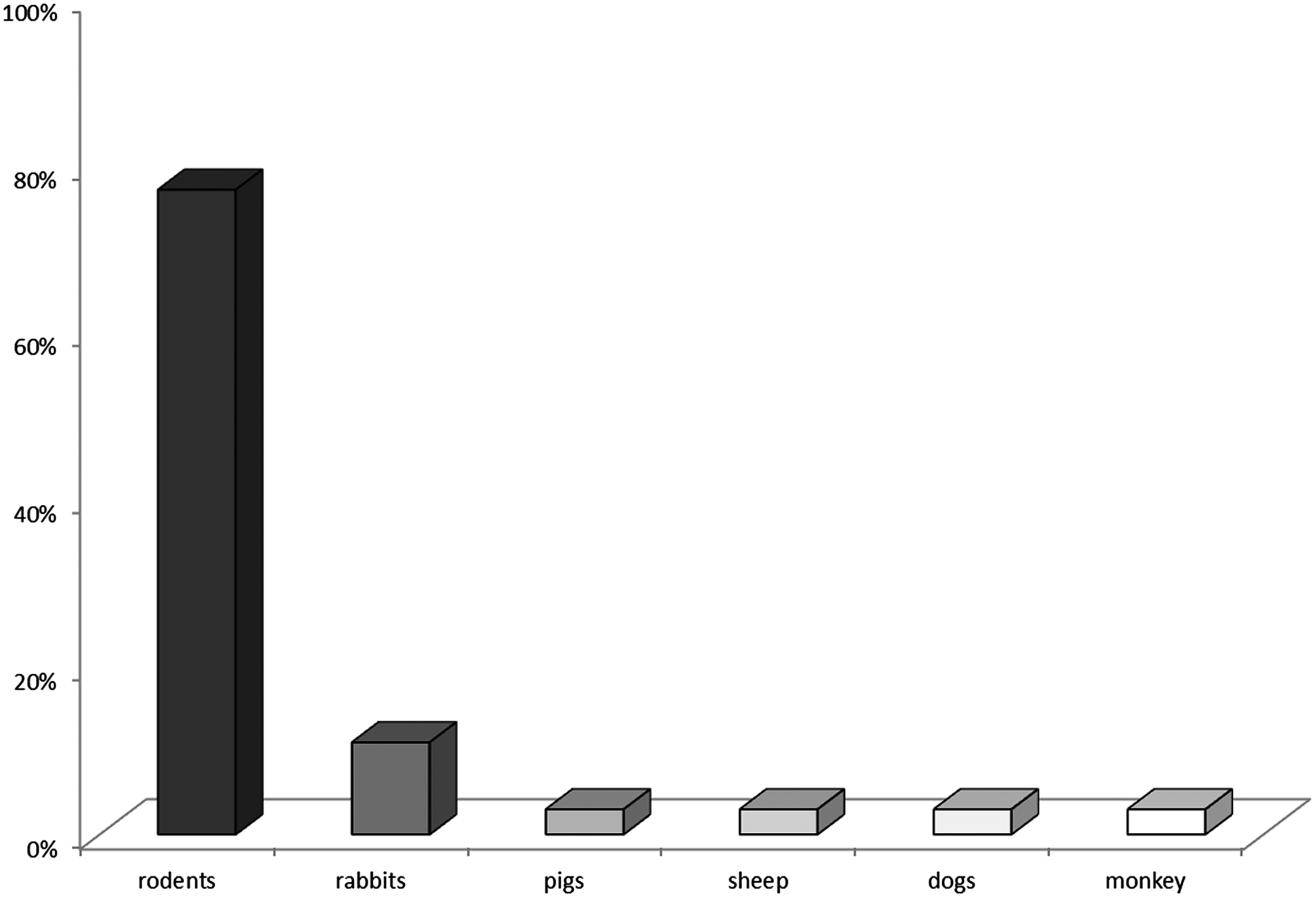
Distribution of species in lymphedema models (n = 35, data from first search).
Rodent models of secondary lymphedema
Circumferential full-thickness skin excision is mostly used to induce secondary lymphedema in rodents. The most popular approaches have been rodent limb8,15 and tail11,12,16 models (Fig. 2). To achieve successful lymphatic obliteration, lymphatics were stained by lymphatic dyes such as methylene blue by subcutaneous or intradermal injection distal to surgical area.9,17 In rodent thighs, the medial neurovascular bundle is saved and dissected by the surrounding tissue. 17 The underlining muscle is destroyed to reach the deep lymphatic system either by ligation or electrocauterization. 17
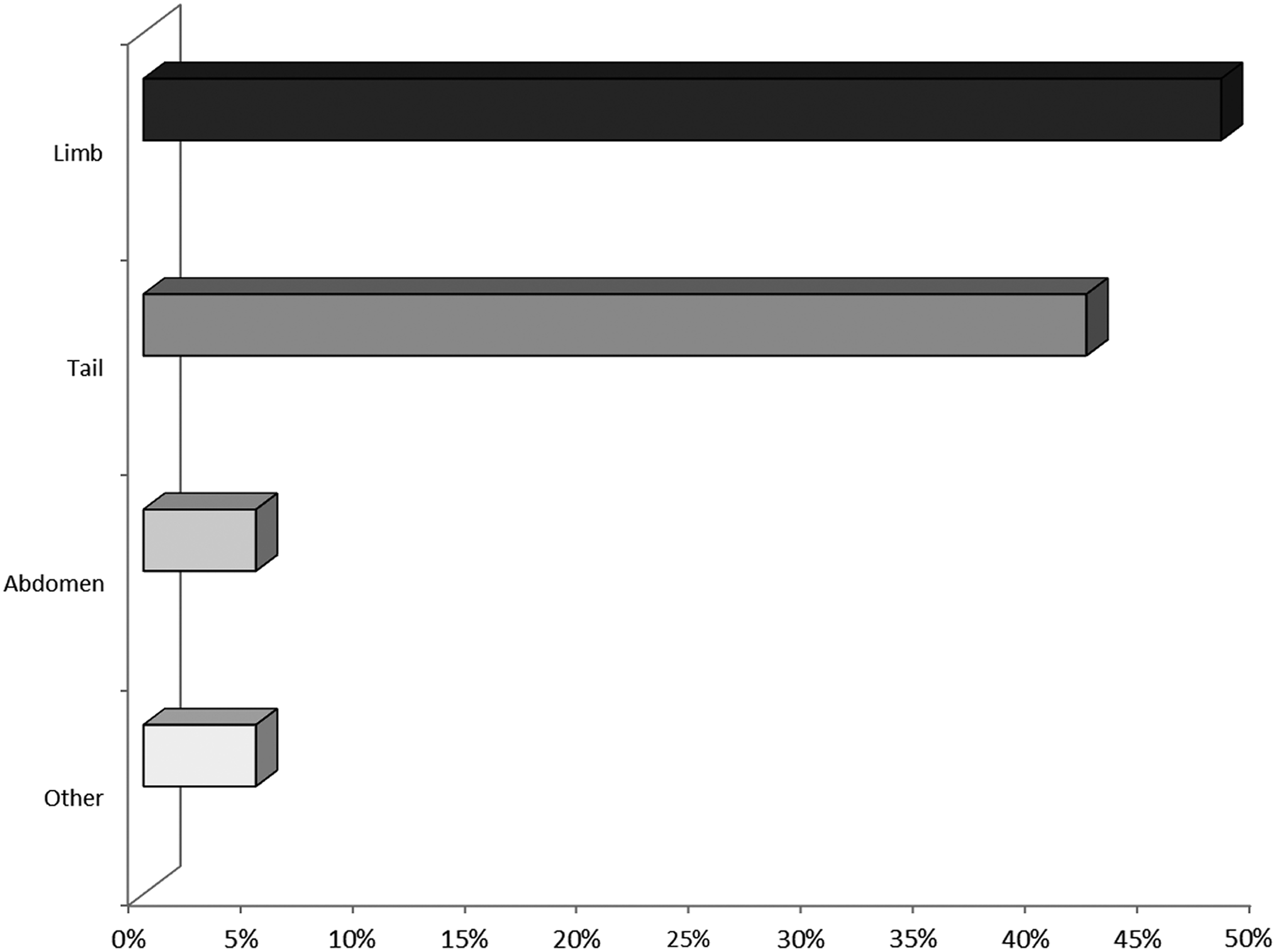
Proportion of various approaches in rodent models (n = 42, data from both searches).
In rodent tail models, circumferential excision is made in a defined distance distal to the base of the tail. 9 The blue-dyed lymphatics were ligated or cauterized and the wound edges are left for secondary wound healing. 9 Care has to be taken to maintain the integrity of the major blood vessels and tendons to prevent necrosis. 18
In some cases lymph node dissection was added to lymphatic obliteration, 15 or axillary lymph node dissection (ALND) was used as an animal model for secondary lymphedema. 19 For ALND, the incision is made through the dermis and the axillary lymph nodes were excised with prestaining lymphatic dye as described before. 19 Because rodents in particular experience highly potent endogenous lymphatic regeneration and radiotherapy in cancer treatment increases the lymphedema risk by ∼10-fold in humans, 20 it can be used in addition to surgery to establish peripheral lymphedema for a period of 4–8 weeks. 16 The mechanism of action might be destruction of the remaining lymphatics or suppression of spontaneous regeneration of lymphatic vessels. 17
The main advantage of rodent lymphedema tail models is that these present a standardized, relatively easy method to induce lymphedema. The clinical relevance in rodent models is high in macroscopic and histological changes. Secondary lymphedema in humans provokes tissue swelling, fat deposition exaggerated inflammation, fibrosis, and hyperkeratosis. 21 In most of the animal models, increased tissue swelling and histological changes like fat deposition, increased epidermal thickness, and indication of fibrosis occur. The main difference in rodent models for secondary lymphedema is the stage of disease. In humans, secondary lymphedema does not recover naturally 22 and occurs most frequently months to years after surgery and radiotherapy. 6 In rodents, achieved secondary lymphedema often recovers after a short period of time 22 or gets necrotic. 17
Rabbit model
Thus, circumferential excision is although used in rabbit's thighs, 15 the most frequently used model in rabbits is the ear model.6,7,22 When circumferential excision is used in a rabbit ear model, the skin on the rabbit ear base, including superficial and deep lymphatic vessels, is removed until only the neurovascular pedicle is left.6,7,24 Fu et al. described a restrictive technique of sparing the perichondrium and cartilage while forming a “skin bridge” containing the central neurovascular bundle. 24 To prevent the reconnection of lymphatics, the excised wound was left to undergo secondary granulation, whereas the edges of the skin were sutured inversely to the perichondrium. Using this technique, stable lymphedema could be achieved within 2 months. Similar to rodents, rabbit models show compensation mechanisms, but lymphedema was mentioned to achieve for at least 12 months. 15 Typical tissue changes such as fibrofatty tissue deposition, greater skin thickness, hypercellularity, and fibrosis were achieved in rabbit lymphedema model.6,7 However, in contrast to human secondary lymphedema, tissue modifications occurred already 2 weeks after surgery and recovered naturally. 6
Large animal approaches
As lymphatic drainage is dependent on muscular activity, body position, breath movements, and capillary permeability, researchers have created large animal models of lymphedema to improve similarity to the human disease pattern. Lymph node dissection is mostly used to induce lymphedema in these models. The advantage of large-animal hind limb models is the single system of lymphatic drainage in the extremities; thus, no circumferential excision is needed. Tobbia et al. were able to maintain limb lymphedema for at least 16 months in sheep using the technique of removal of the popliteal lymph node in combination with ligature of affiliated vessels. 25 In pigs, researchers showed the potential of regeneration after vascularized lymph node transfer and removal of all lymphatic vessels connected to the superficial inguinal lymph node within 2 months. 26 In each group, lymphatic vessel function was significantly improved at 2 months. 26 Thus, similarities to human lymphedema are achieved; chronic stages cannot be displayed. Moreover, Wu et al. created a rhesus monkey lymphedema model by ALND and radiation treatment. The authors established stable lymphedema within 24 months in primates with characteristics of human chronic lymphedema. 27
In summary, circumferential excision in addition to lymph node dissection might currently be the most promising technique for inducing lymphedema. Due to vast endogenous regeneration, it is difficult to establish chronic lymphedema in rodents. Improvements have been achieved with the addition of radiotherapy in surgically treated areas. In large animal models, lymph node dissection without circumferential excision or radiotherapy is a successful approach; however, the experimental setups needed to yield results similar to those in the clinic are very time consuming and labor intensive, and the late effects have to be proofed.
Pharmacological Therapy Options
The most common pharmacological approaches are listed in Figure 3.

Pharmacological treatment of secondary lymphedema.
VEGF-C in secondary lymphedema therapy
Intensive molecular research performed in the last few decades has revealed important new lymphatic markers, such as the lymphatic-specific growth factor VEGF-C 8 and its tyrosine kinase receptor VEGF-R3, which are specific to lymphatic tissue in adults (Fig. 4). 28 However, the lymphatic-specific hyaluronan receptor LYVE-1 is used to differentiate between vascular and lymphatic vessels. In lymphedema therapy, VEGF-C has shown positive results in reducing edematous volume in the rabbit ear, 7 the rodent tail8,29 and limb models,23,30,31 and a pig model. 26 In addition, anti-VEGF-R3 antibody application was found to influence lymphangiogenesis in the mouse tail 11 and a mouse forelimb model. 19
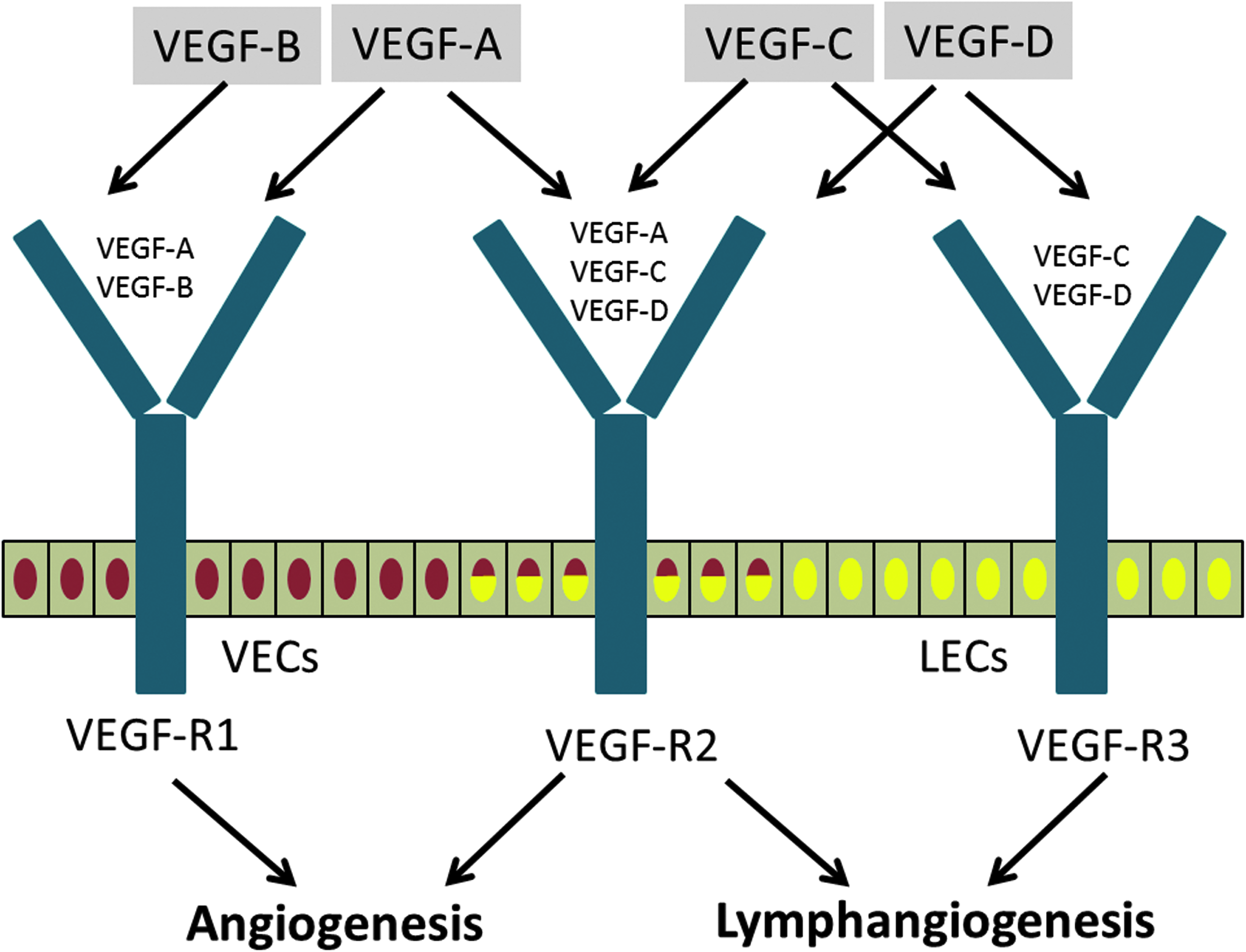
Molecular pathways in angiogenesis and lymphangiogenesis. Red cell nuclei: VECs, yellow cell nuclei: LECs, yellow and red cell nuclei: VECs and LECs. LECs, lymphatic endothelial cells; VECs, vascular endothelial cells.
Combined anti-VEGF-R2 and anti-VEGF-R3 application before surgery and every 5 days postsurgery inhibited resolution of acquired edema. 11 Hence, there are many experimental setups for the concentration and application periods. VEGF-C-based approaches to lymphedema therapy are summarized in Table 2.
PBS, phosphate buffered saline; POD, postoperative day; VEGF, vascular endothelial growth factor.
Stem cells in secondary lymphedema therapy
As bone marrow stromal cells (BMSCs) differentiate into lymphatic endothelial cells (LECs), they may ameliorate lymphatic edema. 15 Therefore, BMSCs or VEGF-C was administered to rat hind limbs 3 months after circumferential excision and lymph node dissection. 15 The group treated with combined BMSCs and VEGF-C showed the best regeneration, as measured by volumetry, VEGF-C quantification, and LYVE-1-positive vessel counting. 15 Similar results were observed for the application of a VEGF-C hydrogel and human adipose-derived stem cells (hADScs) to mouse hind limbs (Table 2). 32 More LYVE-1-positive vessels were observed after 4 weeks in the group treated with combined VEGF-C and hADScs compared with the other groups. 32 In the case of transplantation of LECs, LEC application exhibited better results than application of human dermal microvascular endothelial cells (HDMECs) or placebo based on tail measurements in a rat tail model. 9
Hyaluronidase in secondary lymphedema treatment
To reduce lymphedema, various setups, including hyaluronidase treatment, were established. 33 The authors hypothesized a higher-than-physiological hyaluronan level in a lymphedematous extremity, whereas the protein level was irregularly low. 33 Furthermore, the scientists suggested that macromolecules such as hyaluronan inhibit cell traffic and support cytokine release. In a mouse tail model, hyaluronidase treatment decreased lymphatic dilatation, increased the number of neutrophils, increased the number of VEGF-R3- and LYVE-1-positive vessels, and resulted in lymph flow similar to that in the control group. 33 Hyaluronidase gel application resulted in improved outcomes by reducing the tissue fluid content and fostering edema resolution 18 (Table 4).
Growth factors, cytokines, and enzymes in secondary lymphedema therapy
As hepatocyte growth factor (HGF) regulates the motility, growth, and morphogenesis of many cell types, an external HGF supply increases aortic endothelial cell proliferation and migration. In lymphedema models, HGF application caused a decrease in rat tail thickness and the promotion of lymphatic vessel formation independent of the VEGF pathway 34 (Table 3). Pro-inflammatory cytokines, such as interleukin 8 (IL-8), are assumed to stimulate lymphangiogenesis by serving as inflammatory stimuli. 35 A transgenic mouse model that expresses human IL-8 in the skin was used to detect the impact of this cytokine. IL-8-transgenic mice exhibited a faster reduction in their tail volume after lymphedema than wild-type mice did and showed more LYVE-1-positive cells. The authors concluded that IL-8 may promote the proliferation of LECs and tube formation and migration by LECs without VEGF signaling 35 (Table 4). In addition, matrix metalloproteinases such as MMP-9 may play a significant role in matrix changes during acquired lymphedema. Therefore, transgenic MMP-9-null mice were used to investigate the pathophysiological context. 36 In these knockout mice, the collagen density was lower than in the wild type, and greater tail swelling was noted. Interestingly, LEC proliferation began before VEGF-C upregulation. 36
hADScs, human adipose-derived stem cells; HDMECs, human dermal microvascular endothelial cells; LEC, lymphatic endothelial cells; RT, radiotherapy.
HGF, Hepatocyte growth factor; IL-8, Interleukin-8.
NSAIDs in secondary lymphedema therapy
Nonsteroidal anti-inflammatory drugs, such as ketoprofen, ameliorates tail lymphedema in mice in comparison to sham surgical controls. 37 Histopathological changes such as inflammatory response, hyperkeratosis, and epidermal thickness were significantly reduced in NSAID treatment group. 37 In addition, ketoprofen leads to an increase of pro-lymphangiogenic factors (esp. VEGF-C incl. receptor and LYVE-1). 37 These results indicate that NSAIDs might ameliorate lymphedema symptoms and histopathological changes by inducing pro-lymphangiogenic factors.
To summarize the most important pharmacological therapy options, the main focus has been on VEGF-C application in combination with stem cell therapy or local application of lymphatic endothelial precursor cells. Interestingly, VEGF-C-independent therapies such as hyaluronidase treatment, growth factor therapies, treatment with matrix remodeling factors, or cytokine application improved lymphedema in animal models, which led to the conclusion that VEGF-C is not the only factor responsible for LEC differentiation in wound-healing lymphangiogenesis.
Surgical Therapy Options
The most common surgical techniques are shown in Figure 5.
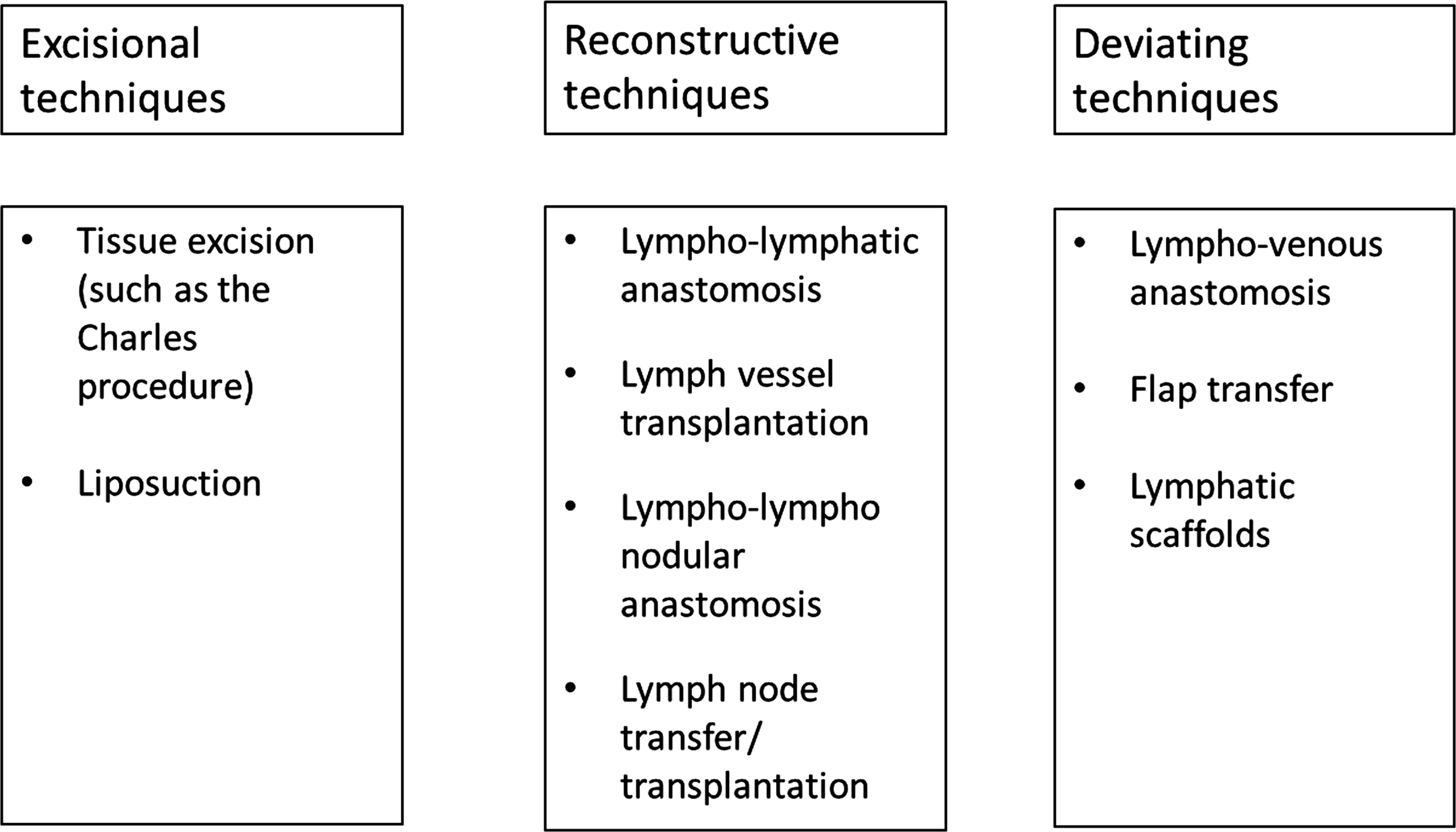
Surgical treatment of secondary lymphedema.
Excisional techniques
The previously prevalent method of radical excision of tissue (the Charles procedure) has been replaced by more tissue-restrictive techniques and is only currently used in the worst cases of chronic status. 3 The disadvantages of excisional techniques in lymphedema therapy are massive tissue trauma, subcutaneous morbidities, painful recovery, and failed reconstruction. 3 Pathological subcutaneous fat accumulation additionally occurs in chronically affected edematous limbs in humans. Liposuction can be performed to reduce this accumulation by removing the extra fat enrichment. However, liposuction without surgical intervention cannot restore the flow in the lymphatic system, so lifelong wearing of compression garments is required to avoid recurrent volume increases. 3
Reconstructive techniques
Lympho-lymphatic anastomosis and lymph vessel transplantation
Lympho-lymphatic anastomosis or lymph vessel transplantations are the most frequently used reconstructive technique of lymphatic vessels in humans. Within these techniques, lymphatic vessels get reconnected to other intact lymphatic vessels to gain new lymphatic drain. Lympho-lymphatic anastomosis could be either transpositions or avascular transplantations. 38
Lympho-lympho nodular anastomosis
In animal models, several reconstructive techniques have been explored. Lympho-lympho nodular (LLN) anastomosis in a rat peritoneal model produced good results in comparison with the endogenous potential to regenerate lymphatics.39,40 After 8 weeks, new connections occurred between the left and right sides after an LLN procedure without anastomosis. The researchers determined that lymphatic drainage through the connected efferent lymph node was 100% reconstructed, whereas endogenous regeneration led to 25% restoration.
Vascularized lymph node transfer
To resolve massive tissue damage using flap techniques, isolated vascular lymph node transfers were tested in rats. The vascularized cervical lymph node transfers involved five to six lymph nodes from the rat neck and showed promising results. 41
In a pig model, vascularized lymph node transfer may improve lymphatic regeneration, especially with the application of VEGF-C. 26 Similar to the case for flap transfers, the length of the vascular pedicle in vascularized lymph node transfer is the determining factor for successful transplantation. However, the microsurgical preparation of major venous and arterial vessels is demanding, time consuming, and risky; so its clinical relevance is controversial.
Avascular lymph node transfer and fragmentation
Since Rothkötter and Pabst reported the viable regeneration of lymph tissue after avascular lymph node fragment transplantation in pigs, 42 many researchers have tried to replicate this result. The autotransplantation of avascular lymph node fragments showed promising results in rat hind limbs, and these results were exceeded with platelet-rich plasma application. 43 The combination of avascular lymph node transfer and VEGF-C has been explored in rodent hind limb 31 and mouse forelimb 23 models. The major advantage of avascular lymph node transfer is that no vascular pedicle is needed, and transplanted segments show functional recovery. 31 However, further research is needed to investigate which fraction of lymph nodes should be transplanted.
Deviating Techniques
Lympho-venous anastomosis
To investigate lympho-venous anastomosis, several researchers compared various approaches using acquired lymphedema models. Kinjo et al. used a dog retroperitoneal model to compare lymphatic node-to-vein anastomosis with lymphatic vessel-to-vein anastomosis, lymphatic vessel-to-isolated-vein anastomosis, and connection to isolated venous segments. 44 There was no patency of lymphatic node-to-vein anastomosis after day 5, and the overall patency decreased in all groups over time. Vessel-to-isolated-vein anastomosis was the best technique in this surgical setting, with a 180-day patency rate of 71%. Nevertheless, the major problem in lympho-venous anastomosis is high venous blood pressure and the resultant risk of clotting of the incoming bloodstream. 39
Flap transfer in lymphedema therapy
Since flap transfer was established for lymphedema therapy, various techniques have been used in animal models. A long-pedicled rectus abdominis mucocutaneous tissue flap containing lymph nodes showed the best results in comparison with control and in situ-replaced groups in a rodent tail model. 45 Full-thickness skin transferred from transgenic LYVE-1-knockout mice showed spontaneous reconnection with recipient vessels and supported full regeneration in a tail skin graft after 6 weeks. 46
Nevertheless, high tissue trauma in transplanted areas and the pedicle length of the vascularized fraction limit the use of this technique.
Lymphatic scaffolds
Vascular scaffolds were newly discovered in lymphatic regeneration. Biodegradable synthetic scaffolds serve as temporary matrix to reconstruct new lymphatic vessels. Dai et al. investigated polyglycolic acid (PGA) scaffolds with endothelialization by human LECs subcutaneously transplanted in nude mice. 47 Six weeks after implantation, biodegradable PGA matrices were degraded while layers of LECs were ordered in the inner vessel walls of silicone tubes. In cell-free scaffolds, no LEC-positive layers could be detected. 47 Staining and polymerase chain reaction with lymphatic-specific marker were positive in LEC matrices and absent in cell-free scaffolds. 47 Nonbiodegradable scaffolds have been successful in cardiovascular research and promising use in lymphatic reconstruction. 48 Kanapathy et al. assumed a nanocomposite polymer (polyhedral oligomeric silsesquioxane poly(carbonate-urea) urethane [POSS-PCU]) as auspicious lymphatic scaffold as it has been successful in cardiovascular approaches. 48 Wong et al. used the rat epigastric artery model for investigating acellular dermal matrix (AlloDerm) and in a cardiovascular setting found histological evidence for lymphatic vessel formation. 49
In conclusion, reconstructive techniques are currently the most promising techniques to rebuild the lymphatic drainage, resulting in a significant decrease in the lymphedema volume. However, further research is needed to compare various techniques to standardize surgical secondary lymphedema therapy, and lymphatic scaffolds have to be investigated application-oriented to rebuild absent lymphatic vessels.
Animal Models in Additional Therapy
Shock wave therapy in secondary lymphedema treatment
Because low-energy shock wave (SW) therapy was recently found to ameliorate ischemia-induced myocardial dysfunction, 50 researchers have been anxious to apply this method to lymphedema therapy. The mechanism of low-dose SW therapy might be the development of cavitation (the formation of vapor bubbles in flowing liquid), 22 which may induce shear stress. This process would result in increased cell membrane permeability and could lead to upregulation of the expression of genes such as VEGF-A. 50 SWs were applied to acquired lymphedema in various experiments, but the total energy flux density differed among all setups (Table 5). After lymphedema was induced in the rabbit ear, SW therapy achieved significant volume decrease in the treated groups. 6 The amounts of VEGF-C and VEGF-R3 and the density of lymphatics were significantly increased in the therapy group after 4 weeks. Similar results were obtained in rat tail 22 and mouse hind limb 51 models. Interestingly, the combination of SWs and local application of VEGF-C produced the best results compared to the results in the other groups. 51
In conclusion, SW therapy was very effective in improving angiogenesis and lymphangiogenesis. The upregulation of important VEGF-family factors led to a volume decrease and the rebuilding of lymphatic structures. The disadvantages of SW treatment included no long-term results and an indication that a VEGF-C overdose may induce lymphatic dysfunction, such as hyperplasia. 51
Modulating diet in secondary lymphedema
Obesity in patients leads to decreased clearance of interstitial macromolecules compared with lean patients 52 and in severe cases with BMI >59 to spontaneously develop lymphedema. 53 Obesity models in animals could help to bare pathological mechanism in secondary lymphedema. In mouse tail models, diet-induced obesity was investigated after lymphatic injury of circumferential excision. 21 Six weeks postoperatively, obese mice showed clinical relevant changes, including fat deposition, fibrosis, and exaggerated inflammation in comparison to lean mice.21,54 In addition, lymph nodal uptake of lymphoscintigraphy agent was significantly reduced in obese mice, especially after lymphatic injury. 21
Lymphangiography in Secondary Lymphedema
The most common procedures for lymphangiography are listed and evaluated in Figure 6.
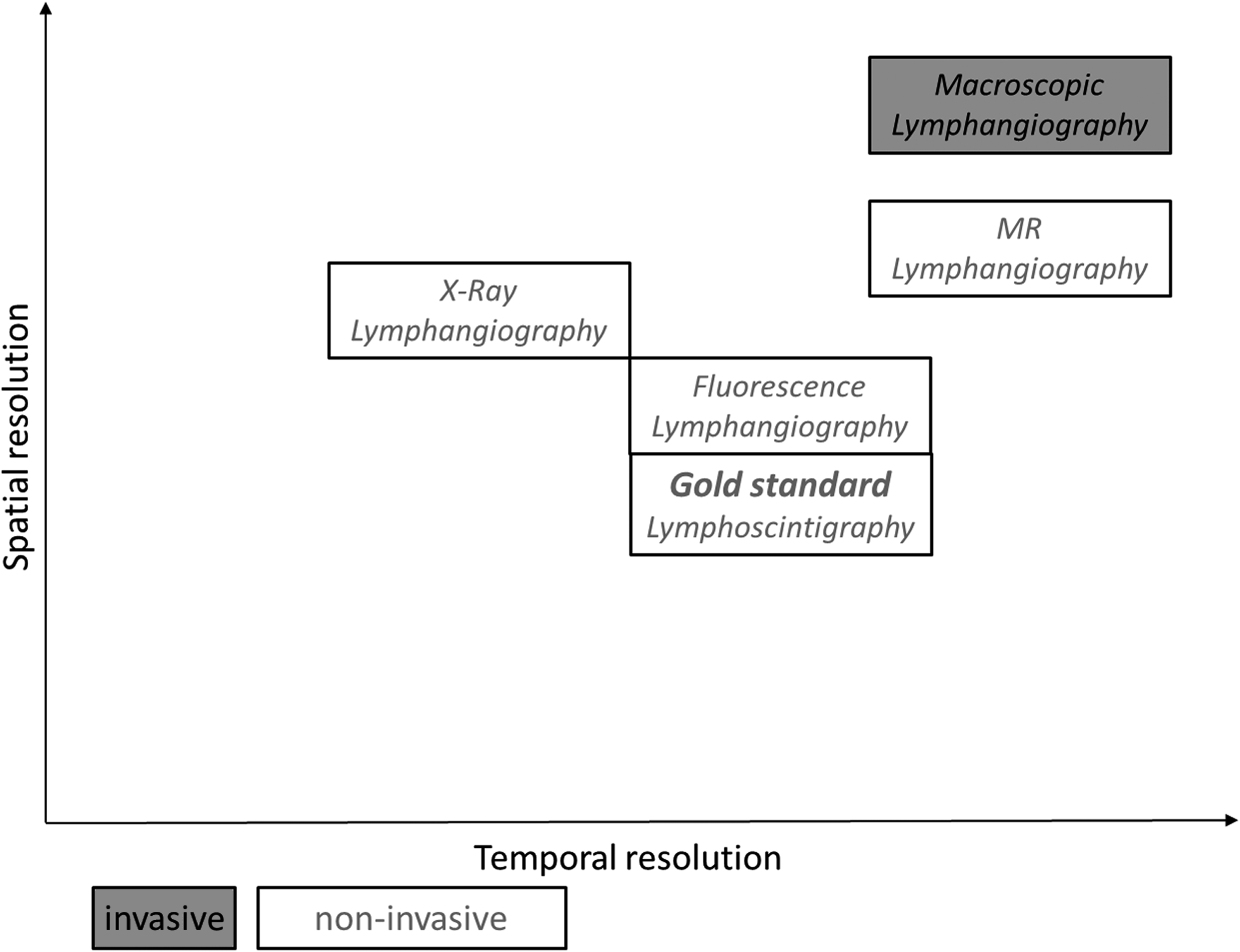
Assessment of lymphangiography methods in secondary lymphedema.
Macroscopic lymphangiography
Various lymph effluent dyes have been tested. Subcutaneous or intradermal injection of special dyes leads to staining of the draining lymphatics. Patent blue, a triphenylmethane dye, is used for food coloring and for staining sentinel lymph nodes in humans. In animals, blue staining of lymphatics was deployed in rat tail models, 34 rodent hind limbs,10,31 and pig hind limbs. 26 An alternative dye is methylene blue. This phenothiazine is typically used in antidote therapy after nitrite intoxication, facilitating metabolism from met hemoglobin to hemoglobin. In animal studies, it was used in rodent tail8,12 and rabbit ear 24 models. Another lymph effluent dye is Evans blue, which was utilized in rodent forelimb23,30 models. All blue staining dyes are utilized for macroscopic evaluation of lymphatic vessels and lymph nodes in draining areas. Quantification using blood sampling after a defined time of agent application and spectrophotometric analysis has also been performed for evaluation.26,30
X-ray lymphangiography
In X-ray lymphangiography, iodine-containing contrast agents such as iopamidol have been used to examine lymphatic flow after subcutaneous application in rabbit ears. 24 Lipiodol, an ethiodized oil-based contrast agent for X-ray imaging, was also used in a pig hind limb model through direct cannulation of lymphatic vessels. 26 The disadvantages of X-ray lymphangiography are poor morphological correlation and low spatial and temporal resolution in addition to ionizing radiation exposure. Furthermore, Isovue, an iodine-containing contrast agent, has occasionally produced allergic reactions or hyperthyreosis, and lipiodol has led to irritation of the lymphatic endothelium and requires direct cannulation. Therefore, X-ray lymphangiography is currently obsolete.
Lymphoscintigraphy
Currently, the gold standard in the imaging of lymphatics is lymphoscintigraphy. A very common agent for lymphoscintigraphy is technetium-99m-radiolabeled sulfur colloid (TC-99m). Detection of lymphatic flow has been conducted with gamma cameras based on the radioactive tracer distribution in the lymph nodes.16,17,55 This technique has been used to detect dermal backflow and functional transport through the lymphatics. With this method, even quantification of lymphatic flow in edematous extremities has been possible through radioactivity index measurement after injection of TC-99m. 7 In this case, the measured radioactivity at injection sites was subtracted from the total number of counts. Higher ratios indicate more persistent radioactivity and, therefore, less lymphatic drainage. 7 The disadvantages of this method include poor morphological correlation, low tissue penetration, poor spatial resolution, and ionizing radiation exposure.
Fluorescence lymphangiography
High-molecular weight fluorescein isothiocyanate (FITC)-labeled dextran fluorescence has been used in live microlymphangiography 30 with ex vivo quantification. Furthermore, near-infrared (NIR) indocyanine green (ICG) fluorescence was used to measure liver function and to perform angiographies. 56 ICG exhibits fluorescence after binding to albumin following intradermal or subcutaneous application. 56 Drainage through the lymphatics enables its detection at a wavelength of 760 nm. 56 These measurements are translated into a black-and-white signal. 57 Dermal backflow, as a sign of lymphatic dysfunction, can be detected after new pathways are created. 56 Fluorescent lymphangiography can also be implemented using multicolor NIR optical imaging by visualizing the simultaneous drainage of two separate lymphatic vessels using nanoparticles. IgG-conjugated NIR optical agents have also been administered to measure various peak emission wavelengths. 58 ICG fluorescence makes it feasible to image dermal backflow with good temporal resolution. However, its drawbacks include poor penetration depth 57 and morphological correlation, poor spatial resolution and no possibility of quantification. In conclusion, ICG fluorescence can be used to examine the early stages of lymphedema, before extremity swelling occurs. 56
Magnetic resonance lymphangiography
To improve morphological correlation and spatial and temporal resolution, magnetic resonance (MR) lymphangiography was established. 59 Gadolinium-containing agents were specifically used to visualize lymphatic functionality. Using animal models, Fink et al. showed promising results in illustrating the lymphatic system in rats without acquired lymphedema. 60 After radiation and axillary lymph node dissection, Wu et al. imaged the lymphatic system in rhesus monkey lymphedema using gadolinium-based MR lymphography 27 after intracutaneous injection. The advantages of this technique include good spatial and temporal resolution for the visualization of small lymphatic vessels and clear congruency with the gold standard, lymphoscintigraphy. 61 Gadolinium-containing contrast agents show high skin penetration and direct morphological correlation of lymph nodes and lymphatic vessels. 62
To sum up, lymphangiography plays an important role in diagnosing secondary lymphedema in humans. In addition, analyzing the functionality of lymphatic vessels is crucial for prospects and to estimate the therapy success. Animal models could help to refine lymphangiography methods to enhance spatial and temporal resolution and investigate reliable methods for lymphatic flow quantification.
Conclusion
Rodent tail and hind limb models are most often used in current lymphatic research. However, especially rodent models suffer from high endogenous lymphatic regeneration, and therefore, only acute lymphedema can be mimicked. Large animal models, such as monkey upper limb lymphedema, are promising, but have to be investigated for late effects. Surgical reconstructive approaches in combination with lymphatic-specific growth factor or stem cell therapy represent the most promising current options among secondary lymphedema treatment models. Several auspicious surgical techniques have been evaluated, but further research is needed to compare techniques to standardize the surgical treatment involved in lymphedema therapy. Furthermore, interference with and the side effects of pharmacological therapies must be monitored. Detailed molecular mechanisms must be elucidated to improve the comparability of animal models to human chronic secondary lymphedema. Further research is also required to enhance current imaging models to yield morphologically correlated and highly temporal and spatially resolved images.
Footnotes
Author Disclosure Statement
No competing financial interests exist.