
Abstract
Abstract
Background:
Sometimes acquired lymphangiectasia (lymphangioma circumscriptum), the pathological mechanism of which is unknown, accompanies lymphedema. The purpose of this study was to better understand the pathological changes present in acquired lymphangiectasia.
Methods and Results:
We examined the pathological characteristics of acquired lymphangiectasia with lymphedema among patients treated at the University of Tokyo Hospital from March 2008 to December 2015. In total, 16 biopsies from 10 patients were investigated. The average age of the patients was 57.2 years (range 43–69), and all were female with secondary lymphedema. Surgical specimens were fixed in formalin, and tissue sections were stained with hematoxylin–eosin. Additional immunostaining (podoplanin, lymphatic vessel endothelial hyaluronan receptor [LYVE] −1, CD4, CD8, CD20, and CD31) was performed in cases 1–3 and 8–10. Dilation of lymphatic vessels in the papillary dermis was present in all 10 cases. Infiltration of inflammatory cells, most of which were lymphocytes, was also observed in the dermis and the epidermis in all cases, even though there were no clinical signs of inflammation. The infiltrating lymphocytes were mainly CD4+ T cells, and less commonly, CD8+ T cells and CD20+ B cells. The number of three types of lymphocytes was significantly larger in the superficial layer of the dermis than in the deep layer, which may indicate that they oozed out from the dilated lymphatic vessels located in the superficial dermis. CD8+ T cells infiltrated the epidermis in seven of eight specimens. In case 4, coagulated lymphatic fluid inside the lymphatic vessel was observed. Proliferation of collagenous fiber in the dermis and acanthosis were observed.
Conclusions:
Lymphatic dilation and proliferation of collagenous fiber in the dermis were seen in cases of acquired lymphangiectasia (lymphangioma circumscriptum). Constant infiltration of lymphocytes in the dermis and the epidermis may have a relation to frequent cellulitis, which is often seen in lymphedema patients.
Introduction
L
Various clinical investigations have been performed to know the extent of these lesions, 14 although the mechanisms responsible for acquired lymphangiectasia (lymph leakage) have not been elucidated. Moreover, it is sometimes diagnosed incorrectly as a wart or condyloma accuminatum.15,16 To further complicate the situation, the lesions are known by several names, including acquired lymphangiectasia, lymphangioma circumscriptum, lymphorrhea,17–19 and lymphatic fistula.
Treatment for acquired lymphangiectasia also varies greatly. Wide excision, partial resection, ablation by CO2, laser, or electrical scalpel, sclerotherapy, and radiotherapy have all been reported, and recurrence during long-term follow-up is not uncommon.19–23
We previously reported on the pathological characteristics and indocyanine green (ICG) lymphographic findings of acquired lymphangiectasia and demonstrated that dermal backflow of lymphatic fluid is present at the precise point of lymphatic leakage.1,2 This finding indicates that there is communication between lymphatic network and this skin lesion, which seems to be different from congenital one, which is said not to have connection with the lymphatic system. 24
In this report, we have further investigated the pathological aspect of acquired lymphangiectasia and have compared these findings with clinical presentations. The purpose of this study is to better understand the pathological changes present in acquired lymphangiectasia, which will help to characterize its etiology, and select the most appropriate therapy.
Materials and Methods
This retrospective study examined the pathological characteristics of acquired lymphangiectasia with lymphedema among patients treated at the University of Tokyo Hospital from March 2008 to December 2015. The clinicopathological characteristics of patients are shown in Table 1. Diagnosis of lymphedema was based on ICG lymphography25–28 or by excluding medical disorder (heart failure, renal failure, hepatic failure, endocrine abnormality) and venous insufficiency.
As some of the patients underwent excision of the lesions more than twice, 16 biopsies from 10 patients were investigated in total. The average age of the patients was 57.2 years (range 43–69), and all were female. All of the patients had secondary lymphedema. Acquired lymphangiectasia was located in the pubis in nine patients and the thigh in one patient. All patients had a history of cellulitis, and all patients with acquired lymphangiectasia in the pubis had a tendency of experiencing cellulitis more than 10 times. The average duration of lymphedema was 14.8 years (range 6–23). Written consent was obtained from each patient for participation in the study, which was approved by the Ethics Review Board at The University of Tokyo Hospital.
Pathological examinations
Surgical specimens were immediately fixed in formalin, and tissue sections were stained with hematoxylin–eosin. Additional immunostaining (podoplanin, lymphatic vessel endothelial hyaluronan receptor [LYVE] −1, CD4, CD8, CD20, and CD31) was performed in cases 1–3 and 8–10. Immunostaining was performed using the podoplanin mouse monoclonal antibody (413451; Nichirei Biosciences, Tokyo, Japan), LYVE-1 rabbit polyclonal antibody (ab10278; Abcam, Tokyo, Japan), CD4 mouse monoclonal antibody (clone 4B12; Dako, Tokyo, Japan), CD8 mouse monoclonal antibody (clone C8/144B; Dako), CD20 rabbit polyclonal antibody (RB-9013-P; Thermo, Yokohama, Japan), and CD31 mouse monoclonal antibody (M0823; Dako). Podoplanin and LYVE-1 are used to localize to the endothelium of lymphatic vessels.
The numbers of the three types of lymphocytes, CD4+ T cell, CD8+ T cell, and CD20+ B cell, were counted with the pictures of high-power field of optical microscope. The superficial layer of the dermis was defined as depth within 1 mm from papillae dermis, and deep layer of the dermis was defined as depth more than 1 mm from papillae dermis. In each patient, we took 10 pictures of lymphocyte-rich regions for superficial and deep layer of CD4, CD8, and CD20 staining, respectively; 60 pictures were taken for each patient. The number of lymphocytes in superficial and deep layer of the dermis was compared by Student's t-test with a significant level of 0.01.
Results
The findings of pathological examinations are shown in Table 2. Dilation of lymphatic vessels in the papillary dermis was present in all 10 cases (Fig. 1). Lymphatic vessels were also dilated in deep layers of the dermis in 10 specimens from 7 cases. On occasion, dilated lymphatic vessels pushed up the epidermis toward the surface of the skin, with the consequence that the epidermis was thinner and disrupted.

Dilated lymphatic vessels in the papillary dermis ( × 40). Lymphatic endothelial cells are stained positive for podoplanin but negative for LYVE-1. The epidermis became thin.
LD, lymphatic dilation.
Although the dilated lymphatic vessels were positive for podoplanin, six of eight specimens were negative for LYVE-1, which is a specific marker of lymphatic endothelial cells (Table 3 and Fig. 1). In some cases, valves were observed in the dilated lymphatic vessels, indicating that they were the collecting lymphatic vessels (Fig. 2).
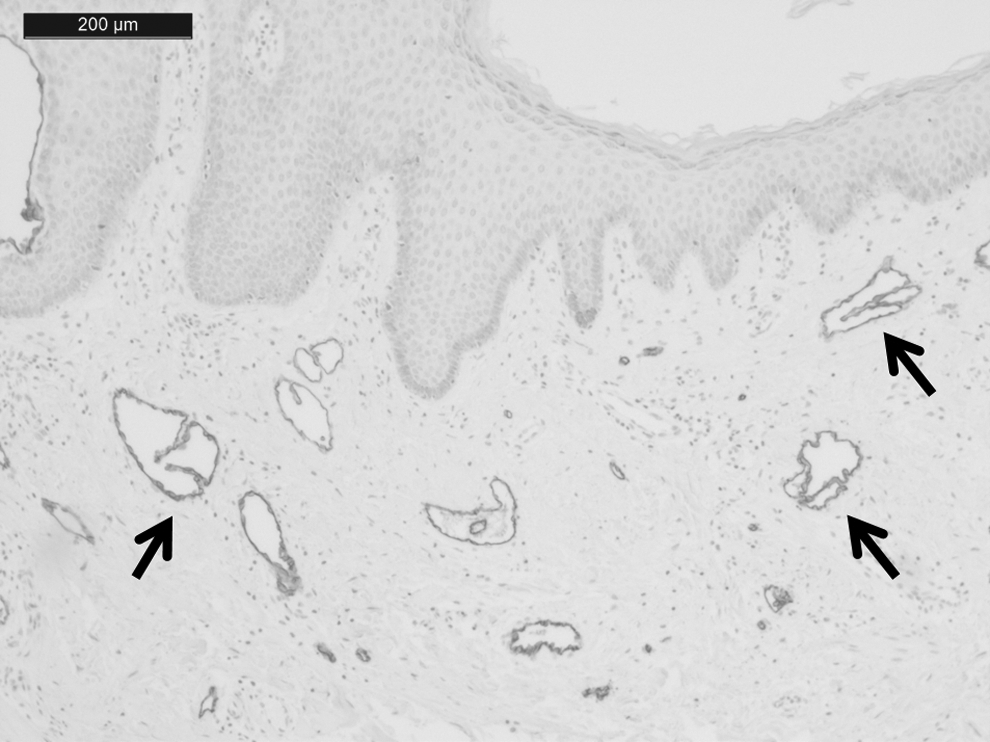
Valves were observed in the dilated lymphatic vessels (arrows), indicating that they were the collecting lymphatic vessels (podoplanin staining, × 100). The lymphatic endothelial cells are positive for podoplanin. The scale bar is 200 μm.
L, around dilated lymphatic vessels; B, around blood vessels; E, epidermal penetration; +, small number; ++, large number, follicular formation.
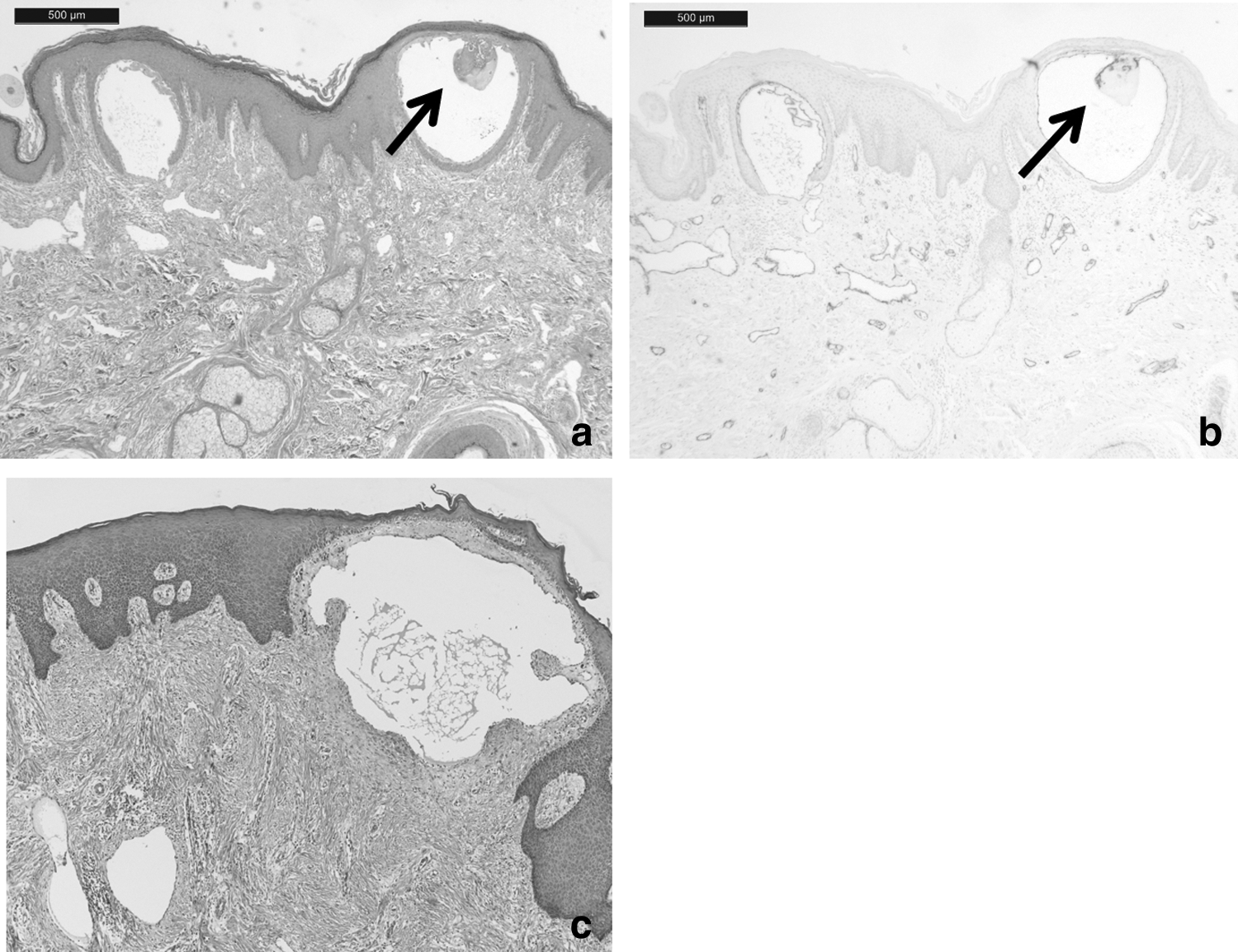
In case 3, coagulated lymphatic fluid inside the lymphatic vessel was observed (Fig. 3a, b), which was likely due to the slow velocity of lymphatic flow in this area. 27 In all cases, proliferation of collagenous fiber in the dermis and acanthosis were observed (Fig. 3c). In addition, hyperkeratosis and parakeratosis were seen in most cases.
Results of pathological examinations.
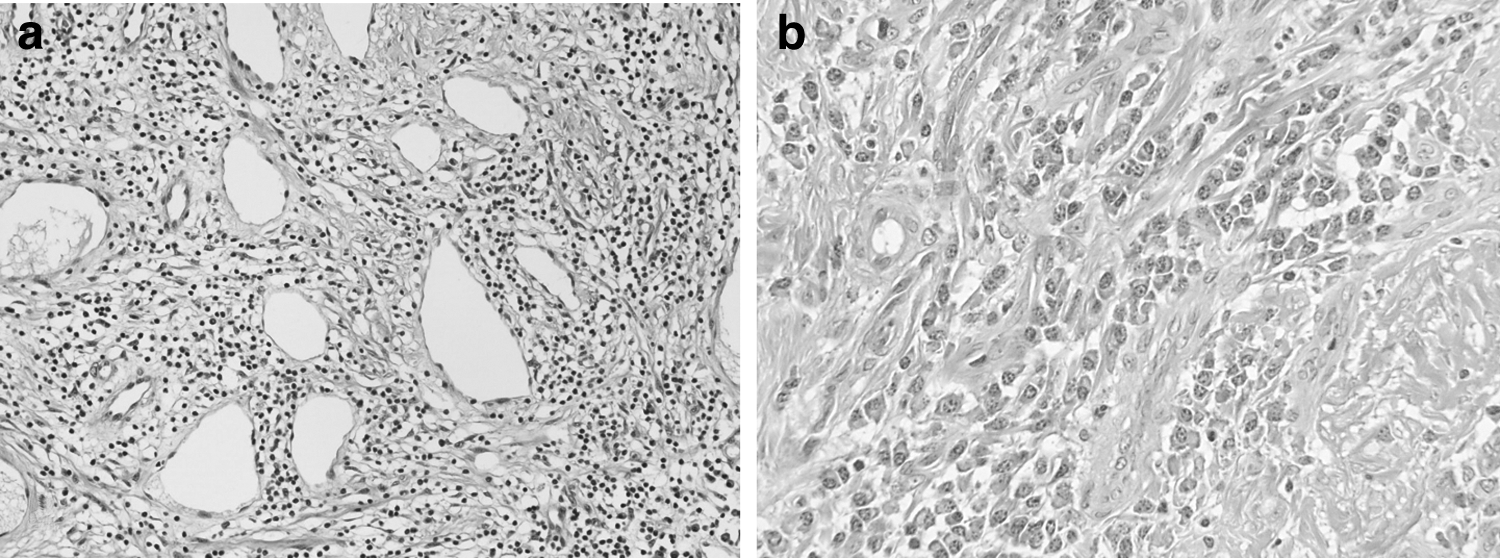
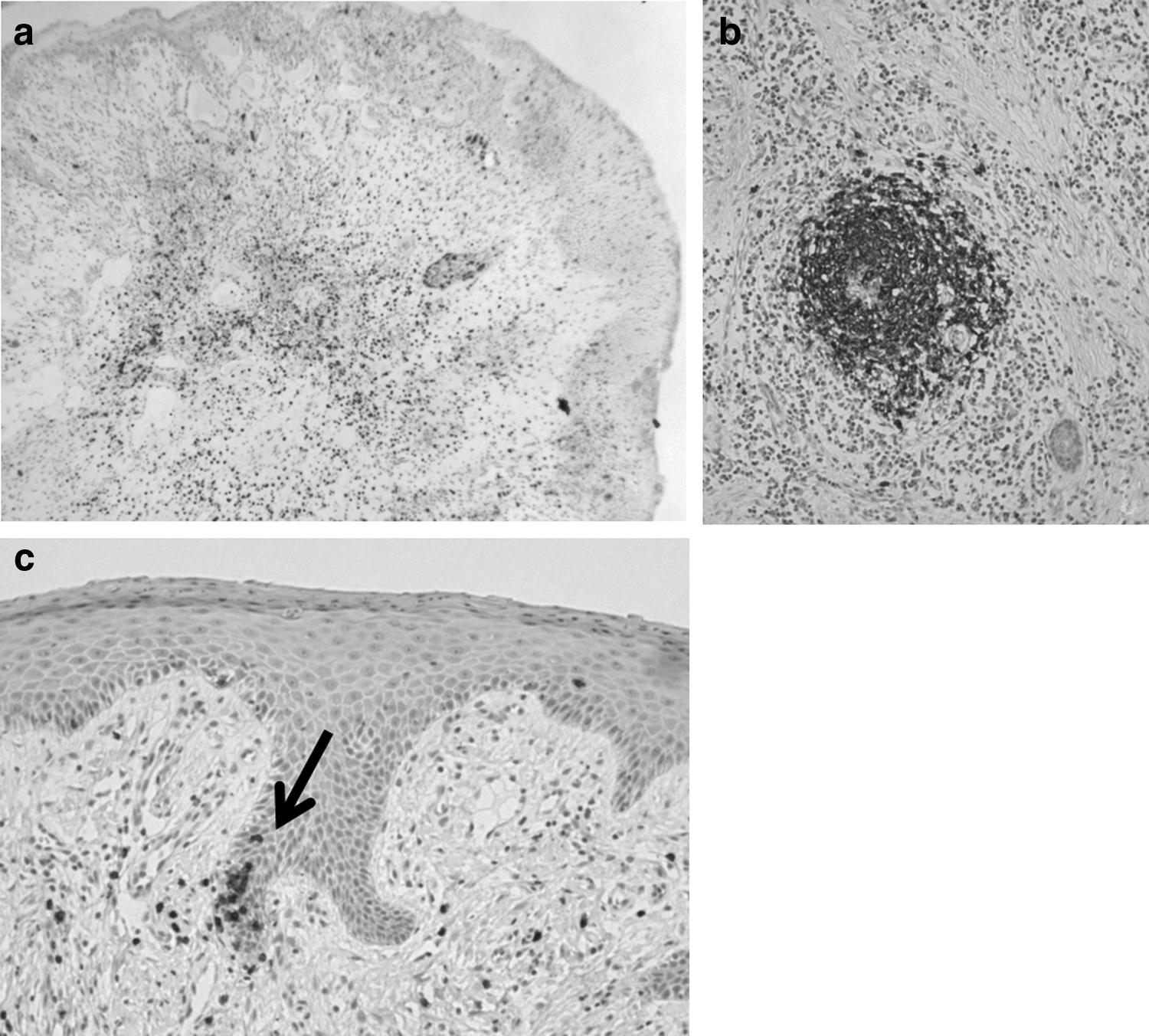
Infiltration of inflammatory cells, most of which were lymphocytes, was observed in the dermis or the epidermis in all cases, even though there were no clinical signs of inflammation (Fig. 4a). Plasma cells, eosinophils, monocytes, and neutrophils also infiltrated in some cases (Fig. 4b). The infiltrating lymphocytes were mainly CD4+ T cells, and less commonly, CD8+ T cells and CD20+ B cells (Table 3). The comparison of the number of three types of lymphocytes is shown in Figure 5. The number of CD4+ T cells was significantly larger than that of CD8+ T cells and CD20+ B cells (p = 1.0 × 10−10 and 0.018, respectively). Also, the number of CD20+ B cells was significantly larger than that of CD8+ T cells (p = 0.0080).
Pathological findings of the dermis around acquired lymphangiectasia.
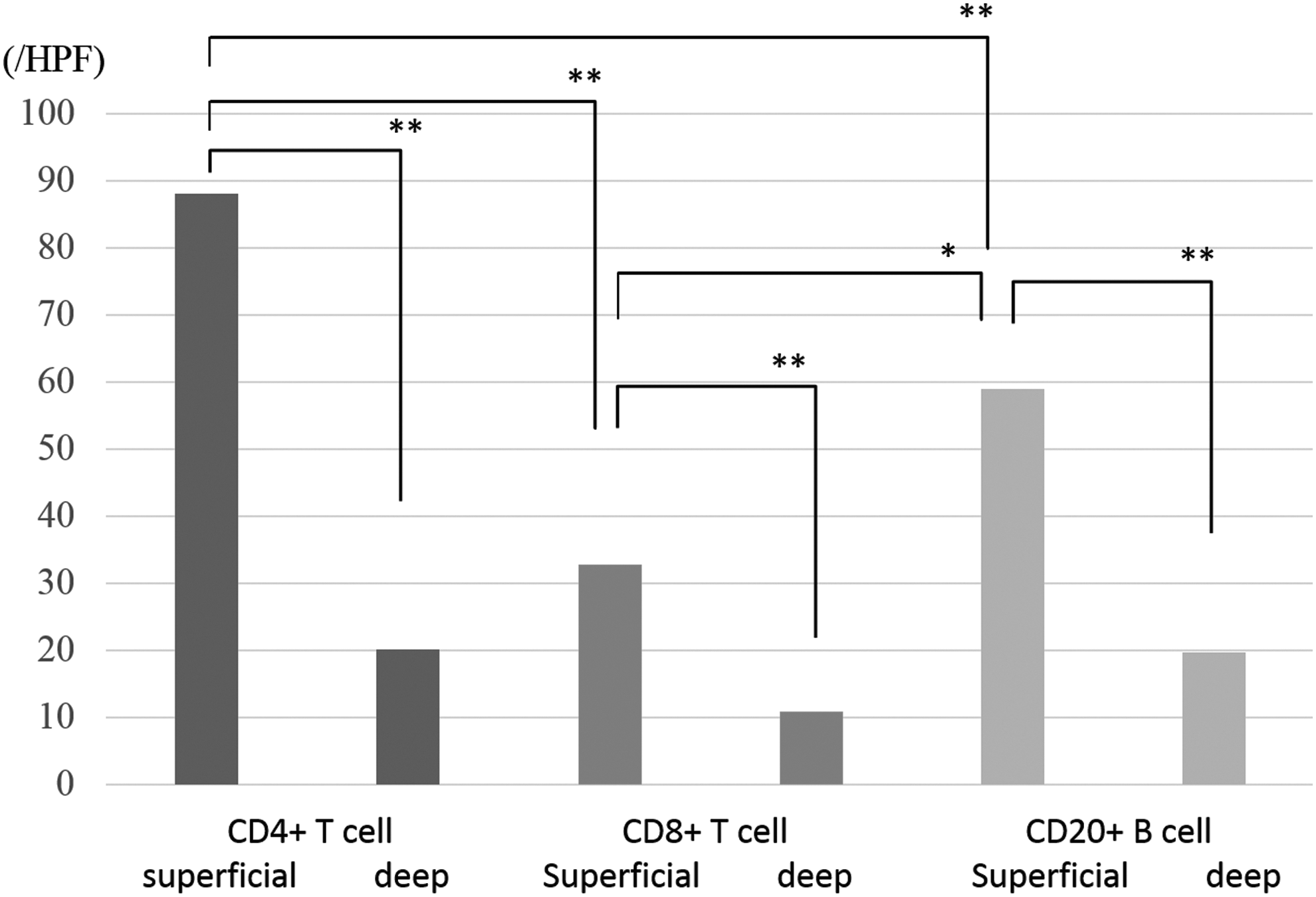
Comparison of the numbers of three types of lymphocytes. The number of CD4+ T cells was significantly larger than that of CD8+ T cells and CD20+ B cells (p = 1.0 × 10−10 and 0.018, respectively). Also, the number of CD20+ B cells was significantly larger than that of CD8+ T cells (p = 0.0080). The numbers of the CD4+ T cells, CD8+ T cells, and CD20+ B cells were significantly larger in superficial layer of the dermis than deep layer (p = 2.6 × 10−14, 8.5 × 10−13, and 0.00089, respectively). *p < 0.05, **p < 0.01, HPF, high-power field.
CD4+ T cells and CD8+ T cells reached a wide distribution around papillary dermis, whereas CD20+ B cells rarely distributed in a wide area and sometimes formed lymph follicles around skin erosions or largely dilated lymphatic vessels (Fig. 6). The numbers of the CD4+ T cells, CD8+ T cells, and CD20+ B cells were significantly larger in the superficial layer of the dermis than deep layer (p = 2.6 × 10−14, 8.5 × 10−13, and 0.00089, respectively). This may mean that lymphocytes distribute around dilated lymphatic vessels in the papillary dermis, leaking out from the bursting lymphatic vessels. In case 2 and 3, lymphocytes aggregated around blood vessels (Fig. 6d).

Immunostaining with CD4, CD8, and CD20.
CD8+ T cells infiltrated the epidermis in seven of eight specimens for which immunostaining was performed (Table 3 and Fig. 6e), while CD4+ T cells infiltrated the epidermis in only one case and CD20+ B cells did not.
CD20+ B cells were often seen forming lymphocyte follicles around skin erosions or in deep layer of the dermis, without regard to location of the dilated lymphatic vessels. They were likely to migrate to react for external stimuli, including bacteria.
Four cases underwent excisional surgery more than twice, and we compared the temporal changes in pathological findings (Table 2). In case 1, dilated lymphatic vessels in the deep dermis were seen only on the first examination, and in case 5, they were seen only on second examination. In case 4, the kinds of inflammatory cells were different. Although the pathological findings varied in each examination, they did not seem to mean that the condition got worse.
Case 1
The patient is a 60-year-old woman who underwent hysterectomy and pelvic lymph node dissection for uterine cervical cancer at the age of 55. Lymphedema occurred in the right leg 1 year later. She started conservative treatment when she was 56 years old. She experienced repeated cellulitis and lymphatic leakage in her pubis, and she consulted our department at the age of 60. She underwent lymphaticovenous anastomosis (LVA) and resection of the skin lesion in her pubis twice.
On ICG lymphography, bilateral dermal backflow was observed in her lower limbs and the skin lesion in her pubis was also enhanced with ICG injected in the foot (Fig. 7).
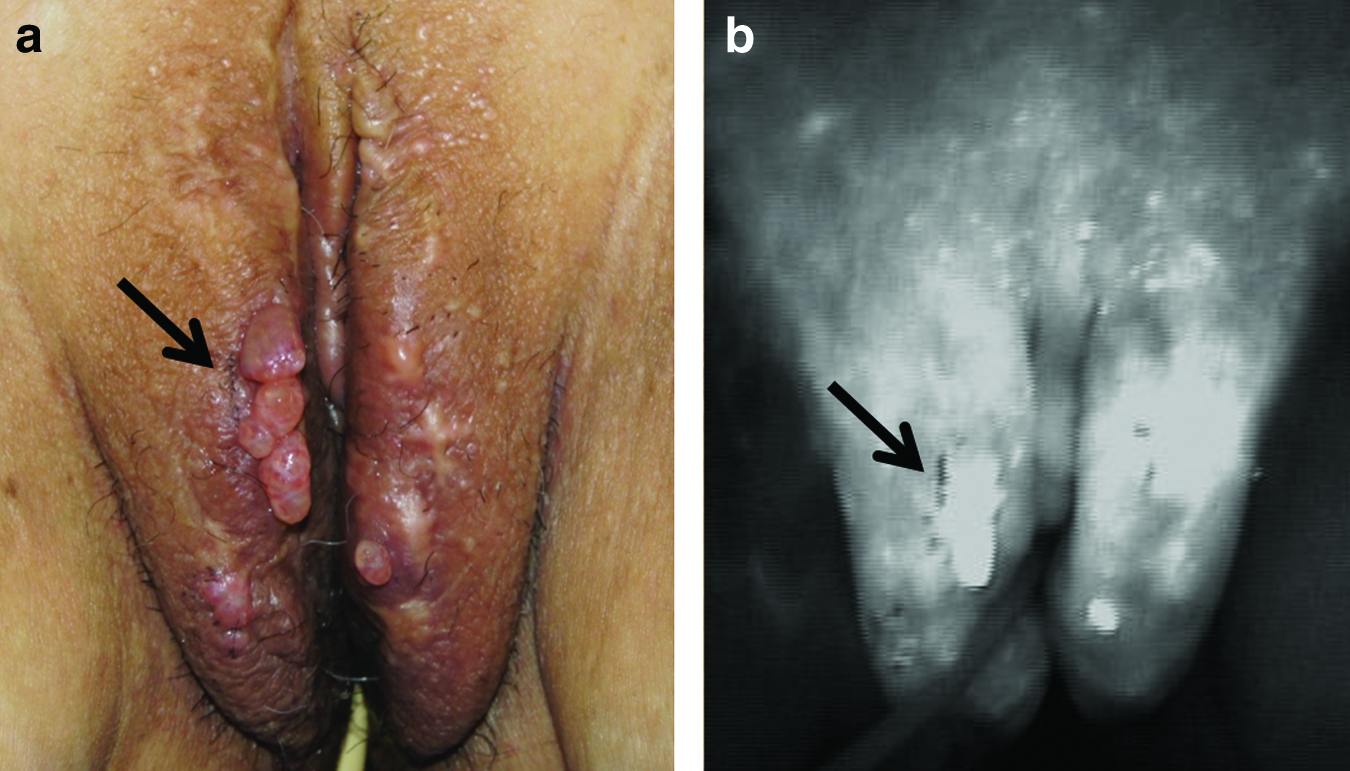
Clinical appearance and indocyanine green (ICG) lymphography of case 1.
On pathological examination, dilated lymphatic vessels in the papillary dermis were observed (Fig. 8). Proliferation of collagenous fiber, acanthosis, parakeratosis, and infiltration of lymphocytes and plasma cells were also present. CD20+ B cells infiltrated around the erosion, and a lymph follicle had formed near the erosion (Fig. 9a, b). Epidermal penetration of CD8+ T cells was observed (Fig. 9c).

Pathological examination of case 2 ( × 40, H&E). Acanthosis and dilated lymphatic vessels in the papillary dermis can be observed.
Pathological examination of case 2.
Discussion
In this study, 16 skin biopsies from 10 patients, who had acquired lymphangiectasia with lymphedema, were analyzed. We observed the infiltration of lymphocytes in the dermis and epidermis, with lack of clinical inflammatory findings. To our knowledge, this is the first report of the pathological findings of acquired lymphangiectasia in connection with the infiltration of lymphocytes.
In all cases, definite fibrosis was present that conformed to lymphedema. In these cases, the long-standing increased lymphatic inner pressure could have induced dilation of superficial lymphatic vessels. The lymphatic leakages in these patients were not related to tumors. Thus, the term “lymphangioma circumscriptum” did not seem to be suitable, and we used the term “acquired lymphangiectasia” in this article.
Although the dilated lymphatic vessels were positive for podoplanin, six of eight specimens were negative for LYVE-1. This may indicate that the lymphatic endothelial cells got injured and became dysfunctional.
We previously reported that the acquired lymphangiectasia accompanied by secondary lymphedema is connected with the deeper lymphatic network as shown by ICG lymphography.1,2 Moreover, in case 1 in the current study, the lesions were enhanced with ICG injected in the patient's foot. This finding differs from the studies of Whimster or Chattranukulchai who reported that there is not a connection between acquired lymphangiectasia and the usual lymphatic network.24,29–31 This difference may be due to whether they are congenital or secondary. In the present study, the lymphatic vessels were dilated in the superficial layer of the dermis, which seemed secondary to increased lymphatic inner pressure.
Infiltration of inflammatory cells was seen in all patients, despite the lack of clinical evidence for inflammation. The lymphocytes infiltrating the dermis were mainly CD4+ T cells, or less commonly, CD8+ T cells and CD20+ B cells. While on one hand this could be the result of repeated cellulitis, on the other hand, it could also be the cause of frequent cellulitis. It is well known that patients with lymphedema often experience cellulitis without definite skin injury. The pathogenesis and progression of the symptoms are very rapid, and redness and local fever quickly spread throughout the whole limb within an hour, which completely differs from usual cellulitis without lymphedema. In lymphedematous limbs, lymphocytes are consistently present in the dermis and subcutaneous tissue, seem to extravasate from lymphatic vessels, and bacterial infection or other small stimuli may induce production of inflammatory cytokines such as INFγ. 31 This phenomenon may be responsible for acute progression of cellulitis in lymphedematous limbs, resembling the mechanism of fixed drug eruption.32–34 In the present study, in seven of eight specimens, epidermal penetration of CD8+ T cells was observed. This is usually seen in fixed drug eruption, in which CD8+ T cells reside in the epidermis, induce the same inflammation when the same drug is administered, and can have a relation to frequent cellulitis of lymphedema patients.
Also, some of the dilated lymphatic vessels were negative for LYVE-1 in some cases, which may mean that the hyaluronic acid receptor of lymphatic endothelial cells was inactivated. LYVE-1 is reported to be downregulated during inflammation, 35 and this can be related to the repeated cellulitis. LVA can reduce the frequency of cellulitis, 3 and this may be explained by this pathology.
We have treated lymphedema patients with LVA36–43 and applied both LVA and skin lesion resection to treat acquired lymphangiectasia.1,2 Simple resection of acquired lymphangiectasia may remove only “the tip of the iceberg” and increased lymphatic inner pressure will persist, thus rendering recurrence inevitable. In the current study, pathological findings indicated that there were many hidden dilated lymphatic vessels other than the most outstanding one. The skin lesions seem to be secondary to increased lymphatic inner pressure, and decreasing the lymphatic inner pressure by LVA may be considered essential for acquired lymphangiectasia.
One limitation of this study is related to the small number of patients investigated. In addition, the relationships between clinical conditions, therapeutic strategies, and the results of long-term follow-up need to be elucidated.
In conclusion, lymphatic dilation in the dermis was seen in all cases of acquired lymphangiectasia. Proliferation of collagenous fiber in the dermis and infiltration of lymphocytes were observed. Finally, constant infiltration of lymphocytes in the dermis and the epidermis may have a relation to frequent cellulitis, which is often seen in lymphedema patients.
Footnotes
Acknowledgment
We thank Akio Hirota for his helpful discussion.
Author Disclosure Statement
No competing financial interests exist. The article was supported by Grant-in-Aid for Scientific Research (26861493). The study sponsor had no role in the data collection, article writing, and submission process.