
Abstract
Abstract
Background:
According to current guidelines, complete lymphadenectomy (LAD) is indicated in melanoma patients with a positive sentinel lymph node. Whereas there is little evidence from randomized trials for a survival benefit of this procedure, its morbidity is not trivial. We aimed to assess clinical associations between risk factors and complications of LAD to guide decision making about this aspect of melanoma management.
Methods and Results:
A cohort of 174 patients who had undergone LAD for primary melanoma was retrospectively analyzed, and multivariable logistic regression models were used to correlate patient risk factors, tumor characteristics, number of excised lymph nodes, and procedural details with the incidence of complications. The overall rate of LAD-associated complications was 41.4%, 33.9% being lymphatic complications. The number of excised lymph nodes was independently associated with development of lymphatic complications (odds ratio 3.90/12.78 if more than 10/20 lymph nodes had been removed, p = 0.01/<0.001, respectively). However, the number of excised lymph nodes had no influence on overall survival using a multivariable Cox proportional hazards regression analysis.
Conclusions:
In this retrospective cohort study, an important association was found between the extent of LAD and lymphatic complications. Further studies should evaluate the necessity and extent of aggressive LAD to balance survival benefit with morbidity of LAD procedures.
Introduction
T
Considering the controversial discussion for survival benefit from radical LAD in melanoma patients, open patient counseling is mandatory. This is especially important since LAD can be associated with significant postoperative complications.9–11 To clarify the factors that should inform this complex decision making process concerning LAD, we retrospectively analyzed the rate of postoperative complications after axillary or inguinal LAD in patients with primary melanoma attending our tertiary referral center between 2001 and 2012. Our aim was to identify clinical risk factors associated with increased risk of postoperative lymphatic complications. We chose to focus particularly on lymphatic problems because lymphatic fistulae and lymphedema occur frequently, can be long lasting, and therapeutic options for them are limited. 12
Taken together, we report in this study that in this cohort of 174 patients, the extent of LAD was associated with an increase of lymphatic morbidity. We aim to raise awareness of the risk of overtreatment of melanoma patients by aggressive LAD.
Patients and Methods
In this retrospective cohort study, we identified 238 melanoma patients in our center's database who had undergone axillary or inguinal lymphadenectomies from January 2001 to January 2012. Of these 238, we excluded 24 patients who had undergone LAD for lymphatic recurrence and a further 16 patients who had undergone resection of more than one lymphatic area. We also excluded 8 patients with more than one primary lesion and 16 patients who had been receiving palliative treatment for advanced disease. Thus, we included 174 of the original 238 patients in our analysis. Data were extracted from the hospital's computer archive, patients' charts, and the Bavarian Melanoma Registry. The study was approved by the local ethics committee (Ethikkommission der Universität Regensburg, No. 12-101-0145).
The clinical decisions for or against sentinel node biopsy (SNB) and LAD were made independently of this analysis by the management team, which regularly included dermatologists and general surgeons. LAD was performed in patients with clinically suspicious lymph nodes (“therapeutic lymphadenectomy” based on the assessment of an experienced dermatologist) or when SNB turned out positive (“completion lymphadenectomy,” usually offered to patients with melanomas thicker than 1 mm). Following LAD, patients were treated on a surgical ward until discharge. Surgery was conducted under the supervision of three attending oncological surgeons. In brief, axillary lymph node dissection was performed routinely in level I and II guided by the respective anatomical structures (axillary vein, pectoralis muscle, latissimus dorsi muscle), achieving an en bloc resection of the lymphatic field. Level III lymph nodes were left unresected unless clinically suspicious. For inguinal dissection, lymph nodes (including the saphenous vein) distal to the inguinal ligament were routinely resected. Lymph nodes proximal to the inguinal ligament and deep pelvic lymph nodes were only removed if there was clinical evidence for metastatic disease in these compartments. Lymphatic vessels were ligated using standard sutures or sealed using a vessel sealing device according to the surgeon's preference. Sole dissection of lymphatic structures was avoided. Pathological examination was carried out on a routine basis by our institution's Department of Pathology following routine protocols.
Regular follow-up was performed by an interdisciplinary team of dermatologists and surgeons. Lymphatic complications were defined as presence of lymphatic fistula, lymphatic edema, and/or lymphatic seroma. Since there is no current consensus definition of “lymphatic fistula,” patients were considered having a fistula when there was continuous lymphatic flow from the wound site after drainage removal, or if drainage removal was not possible due to too high flow rates. We registered this event in the current analysis if further treatment was required, such as replacement of drainage, prolonged hospital stay, or readmission. Lymphatic edema was diagnosed in patients with clinically obvious swelling of the respective extremity. Similarly, lymphatic seroma was defined as visible swelling of the operated area. Wound infections (local infection requiring either reopening of the wound or antibiotic treatment), hematomas (clinical obvious hematomas with swelling and/or necessity of surgical removal), and paresthesias (according to self-assessment by the patient) were classified as “nonlymphatic” complications. Regular status reports were sent to our institution and/or to the Bavarian Melanoma Registry on patients who were followed up elsewhere.
Statistical analyses
Statistical analyses for this study were performed by a biostatistician (FZ) using IBM SPSS Statistics 21.0.0.1 and R (version 3.0.2).
Continuous data are expressed as mean (standard deviation [SD]) and categorical data as frequency counts (percentages). Uni- and multivariable logistic regression was used to identify patient risk factors, tumor characteristics, and procedural details that influenced the incidence of lymphatic and nonlymphatic complications. The influence of excised lymph nodes and of known prognostic factors on overall survival was assessed by means of a multivariable Cox proportional hazards regression model. Odds ratios (ORs), hazard ratios, and corresponding 95% confidence intervals (CIs) were calculated. To assess whether there was a linear relationship between number of removed lymph nodes and mortality, restricted cubic splines (RCS) with five knots (designated at the 5th, 25th, 50th, 75th, and 95th percentile) were used in a multivariable Cox proportional hazards regression model using a SAS macro. 13 The model was adjusted for the same covariates as the main model. A two-sided p-value of ≤0.05 was considered to indicate statistical significance.
Results
Patient and tumor characteristics
The mean age of our study patients was 57.0 years, a majority of patients being male (63.8%; Table 1). The mean body mass index (BMI) was 27.2 kg/m2 (SD: 5.1). Concerning possible risk factors for perioperative complications, 51/174 of the patients (29.3%) were known smokers, 13/172 (7.6%) had type II diabetes mellitus, and 21/172 (12.1%) had peripheral artery disease. Seventeen of 172 patients (9.9%) had a history of a malignancy other than melanoma, and 3/172 (1.7%) were carriers of a chronic infectious disease (either hepatitis B/C or HIV). The median follow-up was 27.8 months.
Hepatitis B/hepatitis C/HIV.
BMI, body mass index; PAD, peripheral artery disease.
The primary melanoma affected the trunk in 79/174 of the study patients (45.4%), the lower extremities in 69/174 (39.9%), and the upper extremities in 25/174 (14.4%). In one patient, the location of the primary was unknown. The most prevalent histological subcategory was nodular melanoma (41.4%), followed by superficial spreading melanoma (24.1%) and acral lentiginous melanoma (13.2%). Amelanotic and polypoid melanomas occurred less frequently (3.4% and 1.7%, respectively). The mean melanoma thickness was 3.46 mm (SD 2.93), the majority of melanomas being classified as T3 (63/174; 36.2%), followed by T2 (43/174; 24.7%), and T4 (42/174; 24.1%). 14 Only 18/174 of all patients (10.3%) had a primary tumor thinner than 1 mm. Regarding N stage after final pathologic examination, most patients were N1 (62/162; 36.7%), N2 (54/162; 32.0%), or N3 (47/162; 27.8%), only a few patients being staged N0 (6/162; 3.6%). The median time span between resection of the primary and LAD was 2 days (range 0–184 days). SNB had been performed in 96/174 cases (55.2%), 80/96 (83.3%) being positive. In most patients, lymph nodes were clinically suspicious at the time of resection (120/151; 79.5%; Table 2).
Based on clinical examination.
LAD, lymphadenectomy; LN, lymph node; SNB, sentinel node biopsy.
Lymph node dissection and postoperative course
Clinically, complete lymph node dissection had been accomplished in all cases. Axillary and inguinal lymph node dissection was performed in 95/174 and 79/174 patients, respectively. The mean duration of surgery was 1 hour and 57 minutes and a mean of 12 lymph nodes were resected. Up to 10 lymph nodes had been removed in 77/172 of cases (44.8%), 11–20 in 77/172 (44.8%), and >20 in 18/172 (10.5%).
Seventy-two of the 174 patients (41.4%) had developed at least one postoperative complication: in 19 (10.9%) these were wound infections; postoperative hematomas or paresthesiae were documented in fewer patients (seven [4.0%] and six cases [3.3%], respectively). The commonest complications were lymphatic, defined as edema, seroma, or fistula; these occurred in 33.9% of patients. The mean lymphatic drainage decreased from 153.3 mL/24 h on day 3 to 74.0 mL/24 h on day 7 and to 24.8 mL/24 h on day 14 postoperatively. The drainage volume was greater than 100 mL/24 h on day 7 in 40 patients (23.7%), the numbers decreasing to 10 patients (6.9%) on day 14. Approximately one in four patients (24.7%) had been discharged with the draining tube in place because the volume of fluid still draining was too great to allow safe removal of the drainage (Table 3). The overall mean postoperative hospital stay was 12.5 days (range 3–89 days), whereas it was 8.7 days for patients with no complications and 17.9 days for those with at least one surgical complication. Occurrence of nonlymphatic complications led to a mean hospital stay of 21.9 days compared with 17.3 days for patients with lymphatic complications (Table 3).
Risk factors associated with lymphatic and nonlymphatic complications
Uni- and multivariable logistic regression analyses were performed to identify risk factors leading to the development of postoperative complications in the present cohort of patients. According to univariable analyses (data not shown), age, BMI, diabetes, peripheral arterial disease, site of surgery, and number of excised lymph nodes were risk factors. According to multivariable logistic regression of all significant variables, the risk of lymphatic complications was independent of age, BMI, and comorbidities; however, the risk of developing a lymphatic complication was significantly greater in patients who had undergone LAD of the groin (OR 11.1; p < 0.001) than in those who had undergone LAD at the axilla and increased in parallel with the number of lymph nodes removed (OR 1.11; 95% CI 1.04–1.18: p = 0.001). Compared with patients in whom up to 10 lymph nodes had been resected, patients in whom 11–20/more than 20 lymph nodes had been removed had increased ORs of 3.90/12.78, respectively (p values: 0.003/<0.001, respectively; Table 4). The risk of developing a nonlymphatic complication increased with BMI (OR 1.09; p = 0.033) and with groin as site of surgery (OR 4.0; p = 0.012).
Significant p values are shown in bold.
Site of surgery: groin versus axilla.
Number of resected lymph nodes.
Kaplan–Meier and multivariable Cox regression analysis of overall survival
Kaplan–Meier survival analysis was stratified by pathological nodal status according to the TNM system. Comparing patient survival within the individual N stages, resection of more than 10 lymph nodes did not significantly improve survival in any N-stratified subgroup of patients (Fig. 1). Furthermore, according to multivariable Cox regression analysis for age, tumor thickness (T stage), nodal stage (N stage), and number of resected lymph nodes, only T and N stage significantly influenced overall survival (Table 5), while the number of excised lymph nodes was no predictor of survival. Conversely, RCS analysis identified a positive linear relationship between number of removed lymph nodes and increased mortality, suggesting that hazard for mortality increases in parallel with number of excised lymph nodes (data not shown).
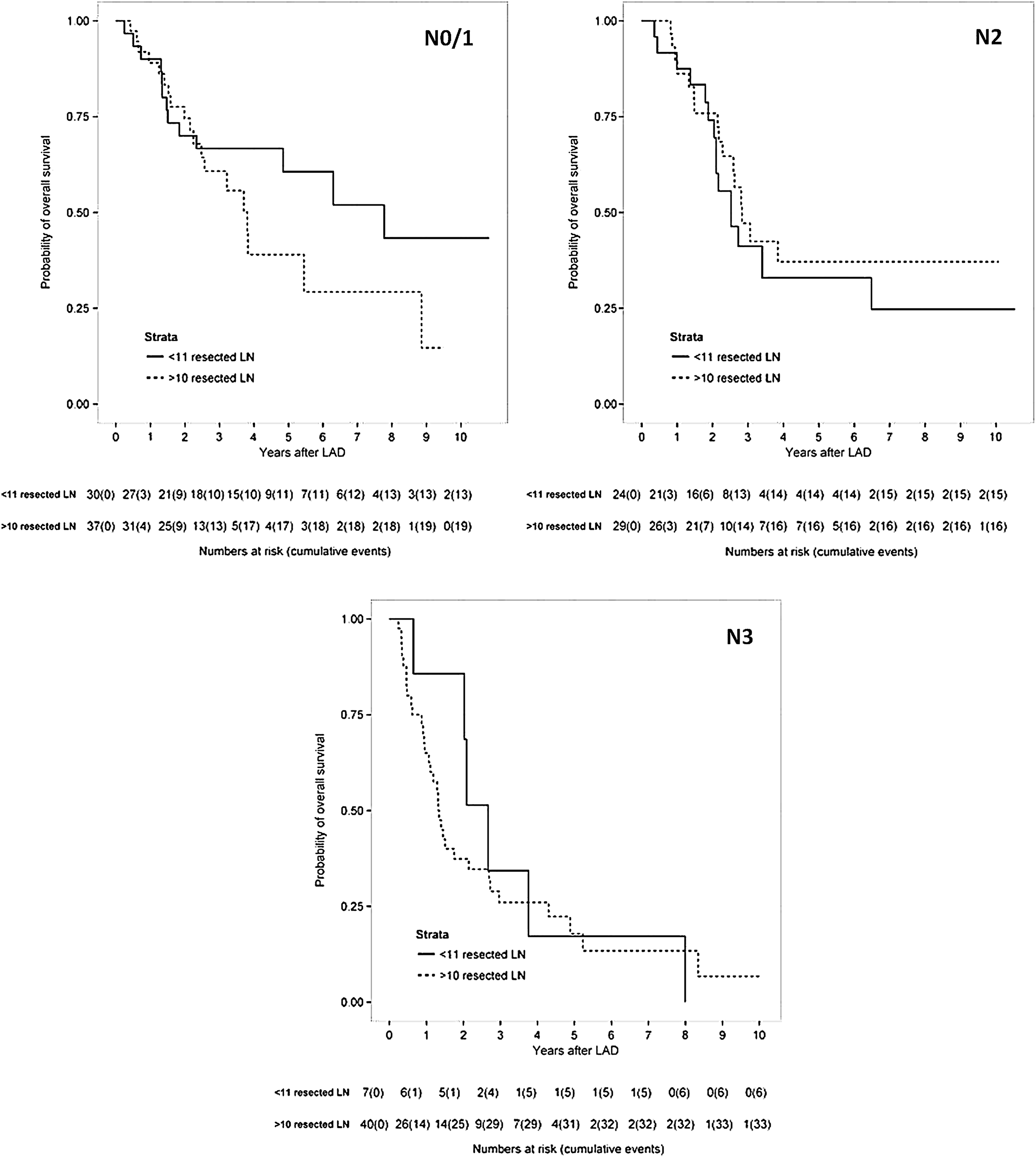
Kaplan–Meier survival curves stratified by N stage: patients with 10 or less lymph nodes versus more than 10 lymph nodes resected. Statistical analysis did not show a significant survival benefit in any category (p values: N0/1: 0.209; N2: 0.538; N3: 0.569).
Significant p values are shown in bold.
Number of resected lymph nodes.
CI, confidence interval; HR, hazard ratio.
Discussion
Although a definite survival benefit has to be confirmed by future trials,3,5,7 LAD is currently the recommended treatment for melanoma patients with a tumor-positive sentinel lymph node or clinically suspicious lymph nodes. Because the morbidity following LAD is significant, we attempted to identify risk factors associated with postoperative complications to facilitate improved individual patient counseling. Because current studies either focus on oncologic outcome or overall morbidity, leaving questions about an individual's risk factors unanswered, our focus on postoperative complications is particularly important.
Our current data show that LAD is associated with significant postoperative morbidity, especially for LAD of the groin. In our study, the most frequent complications were lymphatic in origin, such as lymphedema and lymphatic fistulas. Of interest in this context, some authors postulate an increased lymphatic flow associated with melanoma lesions, although this hypothesis is not supported by observations in humans. 15 In line with other studies, postoperative seromas, wound infections, paresthesiae, and hematomas were less frequent.9–12,16 The high incidence and clinical implication of lymphatic edema were previously shown by Hyngstrom et al., who showed that LAD is frequently associated with limb volume increase of more than 5% causing symptoms. 11 We have added to published data by showing that the extent of LAD correlates positively with the frequency of lymphatic complications, an important clinical aspect that has not previously been elucidated. We need to add, however, that only clinically apparent complications were recorded, thereby possibly missing subclinical complications. Remarkably, patient-specific risk factors (such as clinically significant comorbidities) were not associated with an increased rate of lymphatic complications. Concerning nonlymphatic complications, high BMI was the only relevant independent risk factor contributing to increased morbidity in our study. It has been reported that early LAD is associated with less complications than late LAD 17 ; we did not address this factor in our cohort of patients. Of note, the overall hospital stay was comparably long in our cohort of patients, even when no complication occurred. This might be best explained by the fact that patients usually stay in our hospital until all tubes are removed and a therapy plan based on the pathology report has been made. Our data, however, outline that any complications lead to a prolongation of the hospital stay.
From an oncologic perspective, the evidence on which the recommendation to perform LAD in all sentinel node-positive patients is inconclusive.18,19 The seminal (yet disputed6,7) Multicenter Selective Lymphadenectomy Trials (MSLT)-I study compared SNB followed by LAD with clinical observation of the relevant nodal basin and resection once lymph nodes became clinically apparent. Although disease-free survival rates favored immediate lymph node dissection, overall survival did not differ between these groups; however, advantages for certain subpopulations were subsequently postulated. 20 Several additional studies, none of them prospective or randomized, have reported possible benefits (such as control of regional disease) of LAD in various subgroups of patients.21–24 Recently, a large retrospective study by Rossi et al. reported a positive association between the number of excised lymph nodes and prognosis, suggesting that aggressive LAD is beneficial. 25 In our cohort of patients, we found no correlation between extent of LAD and survival, that is, no prognostic advantage, for any patient subgroup. This finding is supported by a recent retrospective study by van der Ploeg et al., in which patients with sentinel node-positive melanoma who had undergone immediate LAD did not have superior overall survival to those who had not undergone LAD. 26 A phase III trial comparing SNB plus complete LAD with ultrasound-based observation has commenced (MSLT-II); the results are not yet available. 27 On the contrary, that complete lymph node dissection provides the most accurate staging for diagnostic purposes is undisputed; however, this should not be conflated with the debate about “oncological benefit.” 28
Because the concept of clearing malignant cells from the lymphatic basin to prevent further metastatic seeding seems logical, LAD will likely remain standard practice until very robust evidence against it has been produced. However, this apparently logical concept ignores the possibility that the process of lymph node metastasis does not follow a sequential model (“incubator hypothesis” 27 ). In an alternative scenario, positive lymph nodes are an indicator of systemic disease. Thus, it is then too late for LAD to influence the course of disease. Experimental models and clinical studies are required to further elucidate the biology of melanoma metastasis, especially as a growing body of evidence suggests that metastasis is an early event in cancer development. 29
In conclusion, our retrospective cohort study underscores the high complication rate of LAD in melanoma patients, but does not solve the problem of whether or not to undertake therapeutic LAD for malignant melanoma. Rather, because according to our findings, LAD is the only risk factor for morbidity that can be modified by the treating surgeon, we encourage a discussion with melanoma patients on the necessity for this radical procedure. Until better evidence is available, patients should be made aware of the risks and possible benefits of LAD, and it seems responsible to offer less radical LAD in an attempt to decrease the risk of postoperative morbidity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.