
Abstract
Abstract
Objective:
This study sought to evaluate the effect of elastic compression, functional compressive bandaging, and kinesiotherapy on blood flow of the upper limb with lymphedema secondary to the treatment of breast cancer.
Methods:
This was a randomized blind crossover clinical trial with a washout period of 7 days between treatments. We evaluated 20 women with a mean age of 66.85 years (standard deviation = 11.76), undergoing three types of therapeutic procedures randomly applied by lot: kinesiotherapy, functional compressive bandaging + kinesiotherapy (FCB), and elastic compression + kinesiotherapy (EC). Blood flow, including mean and maximum velocity, was assessed by Doppler ultrasound before and after the therapeutic procedure (immediately after, 15 minutes, and 30 minutes). We used two-way analysis of variance for repeated measures followed by Bonferroni's test, considering a significance level of 5%.
Results:
The EC and FCB groups showed a significant increase in the mean velocity of blood flow in the axillary and brachial arteries and veins compared to the group that received only kinesiotherapy (p < 0.05), but no difference between them (p > 0.05). Moreover, the EC and FCB groups showed greater increase in maximum velocity of blood flow in the brachial artery (p < 0.05) compared to the group that received only kinesiotherapy, but no difference between them (p > 0.05).
Conclusion:
Elastic compression and functional compressive bandaging combined with kinesiotherapy increased blood flow of upper limb lymphedema.
Introduction
W
The physiology of the microcirculation provides a model for a clear understanding of how arterial and venous circulation may interfere in the lymphatic system. Changes occur in the hemodynamics member affected by lymphedema, and the pathophysiology of these changes is still unclear, and therapeutic interventions do not consider this interaction, 7 hence the importance of the study.
The lymphatic system, characterized by specific anatomical conditions, carries the accumulated lymph in the interstitial space into the blood stream, exerting pressure in the microcirculation of the blood vessels and tissues, being the main aim of this complex decongestant therapy. 8
It has been reported in the literature the involvement of blood circulation in the development of upper limb lymphedema, due to the surgical intervention for the treatment of breast cancer. Studies5,9–11 evaluate blood disorders related to lymphedema compared to the contralateral limb, the increase in the flow the main finding, apparel featuring stenosis vessels.
The treatment of lymphedema secondary to the treatment of breast cancer provides the basis for the principles of complete decongestive therapy, considering the best intervention practices consisting of skin care, manual lymphatic drainage, elastic compression, and exercise. 12
The therapeutic procedures used to control and reduce lymphedema as part of complete decongestive therapy are considered effective. 13 However, the circulatory effect of the different techniques used is unclear. Previous studies14,15 have shown that despite the wide use of decongestive therapy, their actual effectiveness remains controversial.
The use of compression therapy promotes increased interstitial pressure, increasing the effectiveness of the vascular pumping especially when associated with exercise due to muscle contraction. 8 The amount of pressure exerted on the limb with lymphedema is extremely important to control the limb volume. 16 The functional compressive bandaging (FCB) is a technique considered as standard therapy in the intensive phase of treatment of lymphedema.17,18 However, the adherence of patients to treatment with this technique is low at this stage due to discomfort caused to the patient. 19
The elastic compression therapy (EC) is used in the maintenance phase and limb edema stability, so the adhesion of the patient to the greatest treatment because it provides less discomfort and is better member of functionality, under a constant pressure. 16
The choice of compression therapy to be performed requires comparative evidence of the functional compressive bandage and the elastic compression, as studies show that both techniques are effective to reduce lymphedema volume. However, the FCB negatively impact on the limb function and patient quality of life13,20 and viable choose to use EC.
The effectiveness of different types of compression therapy in the treatment of lymphedema due to changes in limb volume and blood flow is unclear. Knowledge about the impact of the effects inherent to these therapeutic procedures in morbidity can impact objective and effective intervention strategies. Given the above, this study aims to evaluate the effects of different types of compression treatment on blood flow of the upper limb with lymphedema of women treated for breast cancer.
Materials and Methods
Ethical aspects
This study was approved by the Research Ethics Committee at the Clinics Hospital of the Medical School of Ribeirão Preto of the University of São Paulo, under protocol number 810616/2014 and registered at ClinicalTrials.gov (NCT02517086). All individuals included in this study confirmed their participation by signing a voluntary informed consent.
Study design
This was a randomized blind crossover clinical trial. One researcher was responsible for recruiting and evaluations, another for randomization and concealed allocation, a third researcher was responsible for the implementation of treatment programs, while the last processed and analyzed the data collected.
After standard anamnesis, simple randomization was performed for distribution of individuals into the following groups: kinesiotherapy, functional compressive bandaging + kinesiotherapy (FCB), or elastic compression + kinesiotherapy (EC). The concealed allocation of subjects was carried out with the use of opaque envelopes, sealed and numbered sequentially. Randomization and concealed allocation were conducted by an independent researcher who was not involved with the process of recruitment, evaluation, or intervention. The envelopes were opened only at the time of intervention by the researcher responsible for the implementation of treatment programs.
Population
Sample calculation was performed using Ene software, version 3.0 (Autonomous University of Barcelona, Barcelona, Spain). The sample size was calculated based on a clinical trial conducted by Fong et al. 21 For such, we elected as the outcome variable the maximum velocity of arterial blood flow. The calculation was based on the detection of differences of 4.80 cm/s between groups, assuming a standard deviation (SD) of 5.00 cm/s. Thus, considering a statistical power of 80% and alpha of 5%, 18 patients per group were estimated, and considering sample losses, we recruited 20 patients.
Twenty breast cancer survivors who developed lymphedema were invited and selected to participate in this study, with a mean age of 66.85 years (SD = 11.76) and body mass index (BMI) of 30.27 kg/m2 (SD = 3.06). Regarding the treatment of breast cancer, 18 underwent mastectomy and 2 quadrantectomy. All patients underwent axillary dissection, radiotherapy, and chemotherapy.
The exclusion criteria established were: women with muscle-tendon injuries and/or joint damage in the affected limb; skin disorders; diabetes; adjuvant treatment in progress; submitted to bilateral axillary dissection; diagnosis of metastasis; and peripheral arterial disease risk. Considering the above eligibility criteria, there was no sample loss in this study as shown in Figure 1.
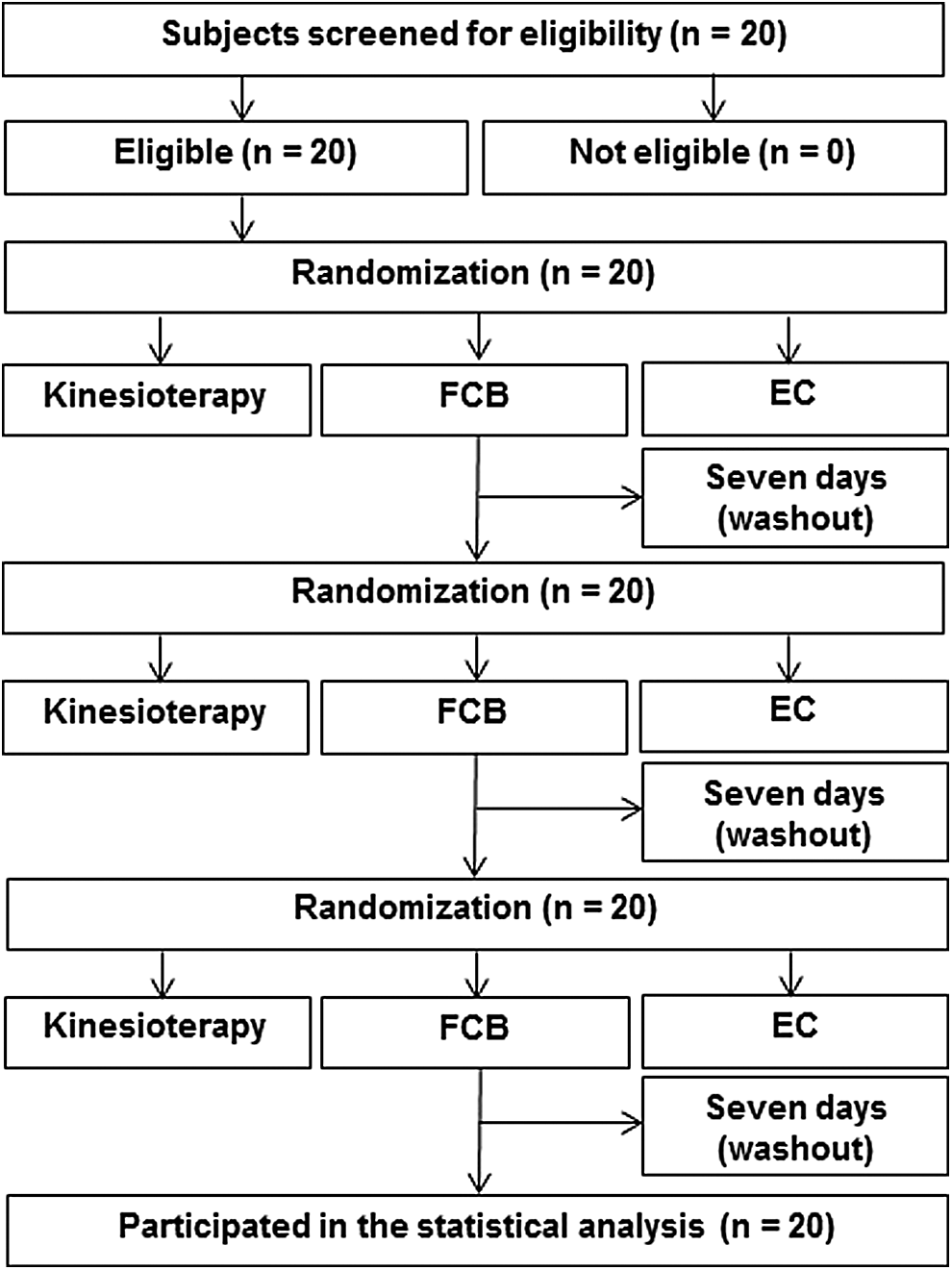
Diagram of the development of the study flow. EC, kinesiotherapy + elastic compression; FCB, kinesiotherapy + functional compressive bandaging.
Initial evaluation
The risk of peripheral artery disease was checked by calculating the ankle–brachial index (ABI). The evaluation was performed in the supine position, after 5 minutes of rest, and systolic blood pressure of posterior tibial artery and the brachial artery was measured bilaterally. The result was the ratio between the highest pressure in the ankle by the higher systolic pressure found in the brachial artery of the upper limbs. Normal values for the ABI are between 0.90 and 1.40, with rates higher than 1.40 representing an increase in resistance of the arteries and rates lower than or equal to 0.90 demonstrating the presence of peripheral arterial disease. 22 Accordingly, there was risk of peripheral artery disease with a mean value of 1.10 (SD = 0.02).
Clinical evaluation was made with standard patient history containing personal data, previous diseases, medication use, data related to the treatment of breast cancer, and physical examination with mass measurement, height, and BMI. Bilateral perimetry was also conducted by an examiner familiar with the procedure. 23 Measurement of seven points distributed in the upper limb was conducted, with tape used to measure the circumference modified with a load at the end to achieve exactly the same tension in all measurements.
For perimetry, the upper limb volume was calculated, considered as the gold standard for measuring irregular lymphedema, performed by an indirect method by sum of the approximate volume of the six truncated cones, formed by measure points of the circumferences of the seven points of the arm and forearm. The sum of these six points provided the total volume. This evaluation method has demonstrated good levels of intra- and inter-rater reliability, with an intraclass correlation coefficient of 0.99. 24 This study considered the difference in volume between the affected upper limb and the unaffected by lymphedema. 25 The mean difference in volume between the members was 0.23 mL (SD = 0.13), with 14 patients with lymphedema on the right and 6 on the left.
Blood flow assessment
For the assessment of blood flow, patients rested for 10 minutes in a room at a controlled temperature of 23°C, positioned supine with arm in supine position. 26 The measurement of the mean and maximum velocity of the arterial and venous blood flow was performed by calibrated ultrasound Doppler SONARA/Tek (Nicolet Vascular; Natus, Pleasanton, CA), with 4 MHz transducer. The analysis of the mean blood flow velocity was performed with the transducer positioned at 45° to the blood vessel to be measured, on greased skin with water soluble gel.
To evaluate the vein and axillary artery, the patient was positioned in supine with the upper member being assessed with abduction and elbow flexion 90° and the transducer positioned in the axillary region. For the evaluation of the vein and brachial artery, the patient remained in the supine position and the upper limb positioned in abduction with 45° of shoulder and elbow extension; the transducer was positioned in the anterior region of the cubital average line. Each evaluation was performed thrice (time window of 5 seconds).
For statistical analysis, we used the arithmetic average of the blood flow of the axillary and brachial arteries and veins. The measurements of blood flow velocity were performed preintervention, immediately after, and 15 and 30 minutes after application of therapeutic procedures.
Treatment protocols
A crossover study was carried out, and a therapeutic session for each therapeutic intervention was conducted with a washout period of 7 days. The order of treatment protocols was randomized by simple draw for each volunteer: kinesiotherapy, functional compressive bandaging and kinesiotherapy (FCB), and elastic compression and kinesiotherapy (EC), detailed in Figure 1.
Kinesiotherapy
The kinesiotherapy program applied in all groups consisted of exercises performed for 50 minutes, involving shoulder active mobilization, including flexion, extension, abduction, adduction, internal rotation, and external rotation, in isolated or combined movements, with 10 replications of each movement, besides stretching movements ending the sequence of movements.26,27
Functional compressive bandaging + kinesiotherapy
The kinesiotherapy intervention was applied according to the parameters described above. Functional compressive bandaging was applied with the patient sitting and with the upper limb on a support. After hydration of the member, cotton knit was used to prevent friction of the strip of foam that was involved in the member. Elastic bandages were wrapped in cotton 5, 10, and 15 cm from the fingers to the axillary region into multiple layers. 28 The degree of pressure exerted by the bandaging (between 30 and 40 mmHg) was measured with equipment developed for this purpose based on Damstra and Partsch 29 and Kang et al. 30
Elastic compression + kinesiotherapy
The kinesiotherapy intervention was applied according to the parameters described above. Elastic compression was performed through clamp VENOSAN (Abreu e Lima, PE, Brazil) with compression of 30–40 mmHg, 13 according to the patient's limb measurements.
Statistical analysis
To check the effects of the treatments in this study, the data were examined first using histograms. Then, we used analysis of variance for repeated measures followed by Bonferroni test, considering two factors (two-way): time (before the intervention, immediately after, and 15 and 30 minutes after) and group (kinesiotherapy, kinesiotherapy + elastic compression, and kinesiotherapy + functional compressive bandaging). Mauchly's sphericity test with Greenhouse-Geisser correction was considered in this analysis. The data from this study were presented as mean, SD, and confidence interval of 95%. Data analysis was performed using SPSS software (Chicago, IL) version 17.0. A 5% significance level for all comparisons was used.
In addition to inferential statistics, we used Cohen's d to determine the size of the clinical effect of the interventions proposed. The interpretation of the values was based on the classification established by Cohen: <0.20 (negligible effect), 0.20–0.50 (small effect), >0.50–0.80 (moderate effect), and >0.80 (large effect). 31
Results
Mean velocity of blood flow
Data relating to mean velocity of blood flow demonstrated a significant group-versus-time interaction for the axillary artery (F = 7.033, p < 0.001) and vein (F = 5.524, p < 0.001) and brachial artery (F = 11.195, p < 0.001) and vein (F = 10.521, p < 0.001). Comparisons over time showed an increase in blood flow velocity immediately after, 15 minutes, and 30 minutes in the FCB and EC groups in all arteries and veins evaluated (Table 1).
Values expressed as mean (SD). All comparisons were performed using the two-way ANOVA for repeated measures post hoc Bonferroni.
Differs from Pre (p < 0.001).
Differs from P0 (p = 0.002).
Differs from P0 (p < 0.001).
Differs from P15 (p < 0.001).
Differs from P15 (p = 0.006).
Differs from P30 (p < 0.001).
Differs from P0 (p = 0.001).
Differs from Pre (p = 0.001).
Differs from P0 (p = 0.004).
Differs from P15 (p = 0.012).
Differs from P15 (p = 0.005).
Differs from Pre (p = 0.004).
Differs from P15 (p = 0.023).
Differs from Pre (p = 0.035).
Differs from P0 (p = 0.010).
Differs from P30 (p = 0.001).
ANOVA, analysis of variance; EC, elastic compression + kinesiotherapy; FCB, functional compressive bandaging + kinesiotherapy; Ki, kinesiotherapy; P0, immediately after treatment; P15, 15 minutes after treatment; P30, 30 minutes after treatment; Pre, pretreatment; SD, standard deviation.
The results for comparisons between groups showed significant results (p < 0.05) for EC and FCB groups, increasing the mean velocity of blood flow of the axillary and brachial arteries and veins compared to the group receiving only kinesiotherapy (Table 2). However, the EC and FCB groups did not significantly differ (p > 0.05).
Values presented in difference between the mean (95% CI). All comparisons were performed using the two-way ANOVA for repeated measures post hoc Bonferroni.
Significant difference (p = 0.001).
Significant difference (p = 0.016).
Significant difference (p < 0.001).
Significant difference (p = 0.019).
Significant difference (p = 0.011).
Significant difference (p = 0.002).
Significant difference (p = 0.014).
Significant difference (p = 0.003).
Significant difference (p = 0.024).
95% CI, 95% confidence interval.
Maximum velocity of blood flow
Regarding maximum velocity of blood flow, no significant group-versus-time interaction for the axillary artery (F = 1.764, p = 0.119) and vein (F = 3.188, p = 0.070) and brachial vein (F = 3.009, p = 0.100) was found. However, a significant group-versus-time interaction was observed in the brachial artery (F = 2.492, p = 0.029). Comparisons over time showed an increase in blood flow immediately and 15 minutes after application of the physiotherapeutic treatments in the three groups in all arteries and veins evaluated (Table 3). In addition, only the axillary vein in EC group and the brachial vein in EC and FCB groups were observed for maintenance of increased blood flow 30 minutes after the application of physical therapy.
Values expressed as mean (SD). All comparisons were performed using the two-way ANOVA for repeated measures post hoc Bonferroni.
Differs from Pre (p = 0.002).
Differs from P0 (p = 0.001).
Differs from Pre (p = 0.008).
Differs from P0 (p < 0.001).
Differs from P15 (p = 0.005).
Differs from Pre (p < 0.001).
Differs from P0 (p = 0.002).
Differs from P15 (p = 0.013).
Differs from P0 (p = 0.020).
Differs from Pre (p = 0.034).
Differs from P0 (p = 0.014).
Differs from Pre (p = 0.027).
Differs from P0 (p = 0.018).
Differs from P15 (p = 0.004).
Differs from Pre (p = 0.010).
The results of the comparative analysis between the groups (Table 4) indicated that the EC and FCB groups showed greater increase in the maximum velocity of blood flow in the brachial artery (p < 0.05) immediately after physical therapy intervention, compared to the kinesiotherapy only group. Furthermore, in the same artery, increased blood flow 15 and 30 minutes (p < 0.05) after the intervention was found for EC and FCB groups compared to the group that received only kinesiotherapy.
Values presented in difference between the mean (95% CI). All comparisons were performed using the two-way ANOVA for repeated measures post hoc Bonferroni.
Significant difference (p = 0.007).
Significant difference (p = 0.018).
Significant difference (p = 0.009).
Significant difference (p = 0.048).
Clinical effects
The results for the clinical effect size showed that Cohen's d values were more significant in the EC and FCB groups for the mean velocity of venous and arterial blood flow (Table 5): a large clinical effect was observed immediately, 15 minutes, and 30 minutes after application of combined physical therapy (Cohen's d ranging from −0.92 to −3.69), except for the axillary vein after 30 minutes, in which a moderate clinical effect was observed, with Cohen's d values of −0.72 and −0.69 for EC and FCB groups, respectively.
In relation to the maximum velocity of venous and arterial blood flow, a smaller clinical effect was found. Thus, there was a negligible to a large clinical effect immediately, 15 minutes, and 30 minutes after application of the physiotherapeutic treatment (Table 6), with Cohen's d values ranging between −0.04 and −1.21.
Discussion
This study aimed to evaluate the effects of different types of compression treatment in the blood flow of the upper limb with lymphedema, with the intent to assess whether the functional compressive bandaging is more effective in the initial treatment of lymphedema due to the treatment of breast cancer. The results showed that both EC and FCB groups provided increased blood circulation of the upper limb.
Functional compressive bandaging is considered standard therapy in the treatment of acute lymphedema.17,18 However, Fu et al. 20 indicated that due to the time, effort, and coordination necessary to carry out the bandaging, this technique becomes expensive and impractical for the patient, and a viable option for alternative intervention is elastic compression garments. According to the findings of this study, the use of elastic compression, in addition to being a more practical technique, showed that blood circulation increased similar to the use of functional compressive bandaging.
Study compared the use of these two resources in women for the treatment of lymphedema, noting greater control of limb volume in women who used functional compressive bandaging. 19
There are few studies evaluating the circulatory changes present in lymphedema. Thus, there are no studies that evaluate the velocity of blood flow after application of compression therapy on upper limb affected by dysfunction. The circulatory effects after applying an exercise protocol in the upper limbs of women with lymphedema were evaluated, 21 detecting increased blood circulation, corroborating the findings of this study.
A systematic review of the effects of exercise on upper limb lymphedema related to breast cancer 32 demonstrated the effectiveness of exercise therapy in reducing limb volume with lymphedema. However, although some studies33,34 evaluate the synergy between compression and exercises, the review points out the lack of studies related to the subject. In this study, although there was an increase of blood flow with exercise, the combination with compression therapy significantly favored this increase compared to kinesiotherapy alone.
Studies32–34 evaluated the combination of compression and exercises and observed a significant reduction in the lymphedema of upper limb compared to active exercises without the use of compression. The inherent effects of compression isolated or combined with exercises are controversial, and all conclusions should be taken with precautions because of the insufficient quality of the selected articles and that the effects on blood circulation are not considered.
The implication of the blood circulatory changes in the development of lymphedema can be detected by Doppler ultrasound that shows the presence of venous and arterial changes in women with mastectomies, which suggest that the formation of lymphedema does not result from lymphatic dysfunction as an isolated event, once many of them do not develop such complications.35,36
The Doppler ultrasound is an important tool in identifying venous and arterial changes. The change in blood velocity reflects impairment of the vessels and the justification for finding. Blood disorders after surgery with lymph interference can be relationship between the blood circulation to the lymph through the anatomical connection (subclavian vein) and the balance of Starling. 37 However, further aspects should also be considered as subsequent changes in lymphatic paths to lock the flow of the lymph collecting vessels, including lymphovenous junction formation with cutaneous vein. 38
Recognition of the impact of the effects inherent to therapeutic procedures (FCB and EC) in morbidity may reflect on objective and effective intervention strategies.
The value of the observation for compression practice and contribution to the mechanism of compression effects was the possibility of modifying the principles of complete decongestive therapy, replacing the FCB by the EC already at an early stage. As the results of this study showed no difference between the methods, the control of lymphedema can be done thus improving the psychological and social aspects of great importance for this population.
Conclusions
This study is the first to evaluate blood flow after application of compression therapy in the treatment of lymphedema of the upper limb secondary to breast cancer, providing directions for these techniques that should be considered by professionals who provide care to this population. Elastic compression and functional compressive bandaging combined with kinesiotherapy promoted, significantly and similarly, an immediate increase in the maximum and mean velocity of blood flow in the axillary and brachial arteries and veins in the upper limb with lymphedema secondary to the treatment for breast cancer.
Footnotes
Acknowledgment
The study received funding of the Coordination for the Improvement of Higher Education Personnel (CAPES).
Author Disclosure Statement
No competing financial interests exist.