
Abstract
Abstract
Background:
Skin fibrosis is a clinically serious pathological process of secondary lymphedema (SLE). The detection of latent or incipient skin fibrosis, including early tissue changes, using sensitive diagnostic equipment is essential. The SkinFibroMeter has been used in skin care; however, its ability to assess skin fibrosis in patients with SLE of the lower limb has not been explored.
Methods and Results:
In this study, 45 female patients with secondary unilateral lower limb LE and 15 healthy female volunteers were enrolled. The skin stiffness values of affected and healthy limbs were measured by using the SkinFibroMeter, and skin samples were assayed by Masson staining. The circumference and interstitial fluid of limbs were also measured and analyzed. Increasing skin stiffness with increasing severity of SLE of the lower limb and skin stiffness significantly positively correlated with stage of lower limb SLE.
Conclusions:
Our results demonstrate that the SkinFibroMeter is very sensitive and accurate for detecting skin fibrosis of edematous limb. Therefore, this new instrument is a promising prospect for diagnosis and assessment of skin fibrosis in patients with lower limb SLE.
Introduction
L
SLE presents as chronic unilateral or bilateral swelling of the lower limbs and is always accompanied with limb pain, heaviness, skin thickening, hyperpigmentation, and altered sensation. 7 Untreated patients are at high risk of infection, skin fibrosis, and functional limitations of the affected limb. Therefore, the earlier SLE is detected and appropriately treated, the better the outcome. 8 In particular, skin fibrosis is a possible serious and irreversible outcome of SLE and is also one of the most difficult symptoms to treat. 9 During the early stage of skin fibrosis, the affected skin gradually hardens.
Some devices are available for assessing skin fibrosis, including tonometer, E-tonometer, indurometer, magnetic resonance (MR) imaging, and ultrasound; these instruments perhaps have the similar technical principle but they have different characteristics and limitations. The earliest modality for evaluating the tonicity of lymphedematous skin, the tonometer, was developed by Clodius et al. 10 Tonometer measures the resistance of tissue to compression; this resistance depending on the mechanical properties of the skin, and in LE-associated fibrosis on the proportion between subcutaneous matrix and interstitial fluid.10–13 However, the plunger of the tonometer needs to be pressed forcibly because of relative insensitivity. Furthermore, the dial must be read while the device is held on the patient, which is challenging for certain measurement sites. In addition, the pits produced by application of the instrument to affected skin can cause pain or discomfort. 14 Therefore, more recently, technologic developments have resulted in modified versions of tonometer and these have been used in a variety of LE-related studies. The electronic digital tonometer (E-tonometer/lymphometer) has replaced the outdated tonometer. Although E-tonometer can eliminate the gravity effect and display the value instantly on the screen, the sensitivity of the sensor is still poor (precision 0.1 g/mm2). Furthermore, it is still necessary to press hard on the skin.15,16 Another device, the indurometer, is also being designed to replace the tonometer. This electromechanical device uses a 200 g mass and a displacement gauge to objectively measure tissue induration. It has a 0.01 mm resolution and a constant force spring allows it to be used in nonvertical positions.14,17 However, Vanderstelt et al. reported that two participants were pinched by the indurometer, indicating a defect in this instrument's design, and this device should be further modified in the assessment of LE. 14 MR imaging and ultrasound can assess changes in fibrotic skin thickness and texture; however, these modalities cannot accurately and quantitatively analyze skin stiffness and their operation is complex and costly.18–20 Thus, many limitations of these devices make fibrosis to be often overlooked by both the patient and physician at an early stage of SLE. Detection of latent or incipient skin fibrosis, including early tissue changes, by using sensitive and convenient diagnostic equipment, is therefore very important.
The SkinFibroMeter (Delfin, Kuopio, Finland), a recently developed, portable, and sensitive instrument, utilizes a small measurement probe (diameter of 23 mm) that is briefly pressed on the skin at all anatomical sites, including curved region. The presence and severity of fibrosis are assessed by using a special three-dimensional (3D) computational finite element to analyze the biomechanical response of skin tissue to external force. To the best of our knowledge, there is no similar 3D computational finite element for previous devices. The skin resists changes in shape when an external force is applied; thus, its ability to resist deformation under a short-term load indicates its stiffness, which is expressed in Newtons (N). The value thus obtained is a measure of skin stiffness, which in turn reflects the presence and severity of skin fibrosis.
The SkinFibroMeter has been used in skin care; however, its ability to assess skin fibrosis in patients with SLE of the lower limb has not been explored. In this study, we used this device to diagnose and evaluate fibrotic changes in the skin of patients with stage I–III SLE of the lower limb and analyzed the relationship between the measured values and disease progression. Specifically, we investigated whether the values measured with the SkinFibroMeter correlate with the severity of skin fibrosis in patients with SLE.
Materials and Methods
Patients and tissue sample collection
From July 2015 to February 2016, 15 women with secondary unilateral lower limb LE were allocated to each of three groups, namely an LEI, LEII, and LEIII group, according to a three-stage scale for classification of lymphedematous limbs. 21 The mean age of these 45 women was 53.7 years (range 38–74 years) and all had undergone radical surgery and completed radiotherapy and/or chemotherapy for endometrial, ovarian, or cervical cancer. The left limb was edematous in 31 patients and the right in 14. No patients had cancer recurrence, deep venous thrombosis in the limbs, kidney failure, cardiac edema, or dermatosis according to blood biochemistry and medical imaging performed by oncologists and physicians. The detailed characteristics of these patients are presented in Table 1. In addition, a control group of 15 healthy female volunteers (mean age 51.5 years, range 39–67 years) was included. Full-thickness skin biopsies of the lymphedematous limbs (2.5 × 1.5 cm) were taken from the pretibial medial part of the leg, 5 cm above the ankle, from two subjects in each group. All subjects provided written informed consent. This clinical study was approved by the Ethics Committee of the Shanghai Ninth People's Hospital.
Values are presented as median or number.
LE, lymphedema.
Measurement and analysis of limb skin stiffness
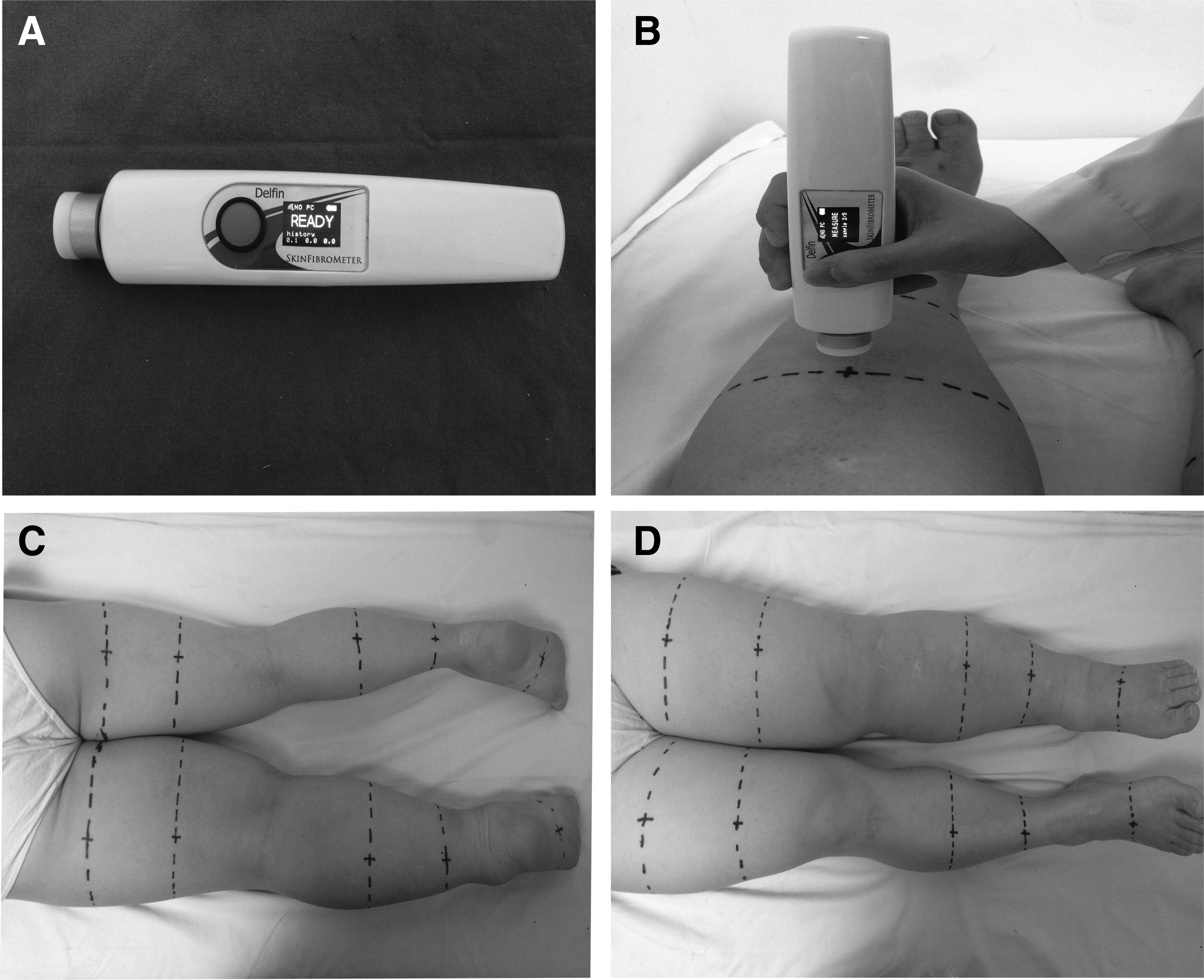
Skin stiffness in the affected and healthy limbs was measured by using the SkinFibroMeter (Fig. 1A). The patient lay on a treatment couch in a supine or prone position and relaxed her lower limbs, which were lying horizontal. The SkinFibroMeter probe was briefly (0.5 seconds) pressed perpendicularly against the skin. Each stiffness value was calculated as the mean of five successful consecutive measurements at the same site (Fig. 1B). Previous stiffness readings were listed under the most recent value and the values mathematically modeled using 3D computational finite element analysis, the final value being displayed on the main screen. If the force applied or duration of measurement was not correct, the message “USER ERROR” was displayed and the repeat measurements obtained. Skin stiffness was measured at 20 points on each lower limb. First, the circumference was measured and a dotted line drawn connecting the following five positions on lower limb: 5 cm above the second plantar toe joint, 5 cm above the lateral malleolus, 10 cm below the inferior border of the patella, and 10 and 20 cm above the superior border of the patella. This resulted in four points of intersection between the foot circumference line and upper, lower, medial, and lateral foot midlines. In addition, there were 16 intersection points between the other circumference lines and anterior, posterior, medial, and lateral midlines of the thigh and leg. These 20 points were marked with a “+” and the SkinFibroMeter used to take measurements at each of them (Fig. 1C, D). The mean value of the skin stiffness at these points of intersection was considered to indicate the overall skin stiffness in the lower limb. The skin stiffness ratio was defined as (mean value of the lymphedematous limb − mean value of the contralateral limb)/mean value of the contralateral limb. To provide a comparison, the control skin stiffness ratio was defined as (large value − small value of the control [contralateral] limb)/small value of the control limb.
Measurement and analysis of limb circumference
The circumferences of each edematous limb were measured using a standard 1-mm polyvinyl chloride fiberglass tape. For lower limb circumference measurements, the patients lay in a supine position, with their legs relaxed and knees straight. The circumferences were measured in cm at five positions on the lower limb: 5 cm above the second plantar toe joint, 5 cm above the lateral malleolus, 10 cm below the inferior border of the patella, and 10 cm and 20 cm above the superior border of the patella and the mean circumference for these five positions calculated. The circumference ratio was defined as (mean circumference value of the lymphedematous limbs − mean circumference value of the contralateral limb)/mean circumference value of the contralateral limb.
Measurement and analysis of interstitial fluid content of the limb
The interstitial fluid content of the lower limbs was measured and analyzed by using a multiple-frequency bioelectrical impedance analysis instrument (Inbody 3.0; Biospace, Seoul, Korea). This instrument measures the impedance of tissue fluid to tiny electrical currents (1 kHz–1 MHz) to accurately assess changes in interstitial fluid in the edematous limb. All measurement data were recorded in kilogram (kg). The interstitial fluid ratio was defined as (mean interstitial fluid value of the lymphedematous limb − mean interstitial fluid value of the contralateral limb)/mean interstitial fluid value of the contralateral limb.
Masson staining
Skin biopsies were embedded in paraffin and the 5 μm sample sections deparaffinized, rehydrated, and then stained in hematoxylin solution. Excess dye was removed with hydrochloric acid in ethanol and the sections were stained in ponceau-acid fuchsin solution, immersed in 2% glacial acetic acid, incubated in phosphomolybdic/phosphotungstic acid solution, and transferred directly to an aniline blue solution. Before imaging, the sections were washed in 2% acetic acid. With this staining method, collagen and mucous cells appear blue, cytoplasm, cellulose, and muscle cells red, and cell nuclei dark blue.
Statistical analysis
Data are presented as mean (range) or number (percent). Statistical analysis was performed using Pearson's method, Spearman correlation coefficient, and Student's t-test with SPSS 17.0 software (IBM, Armonk, NY). All tests were two sided, with a significance level of 0.05 or 0.01.
Results
Expression of collagen in the skin of lymphedematous lower limb increases in parallel with disease stage from LE stage I to stage III
Masson staining revealed greater collagen deposition in lymphedematous than normal skin, indicating definite fibrosis in the edematous limbs. Furthermore, expression of collagen increased in parallel with stage of disease from LE Stage I to Stage III (Fig. 2).
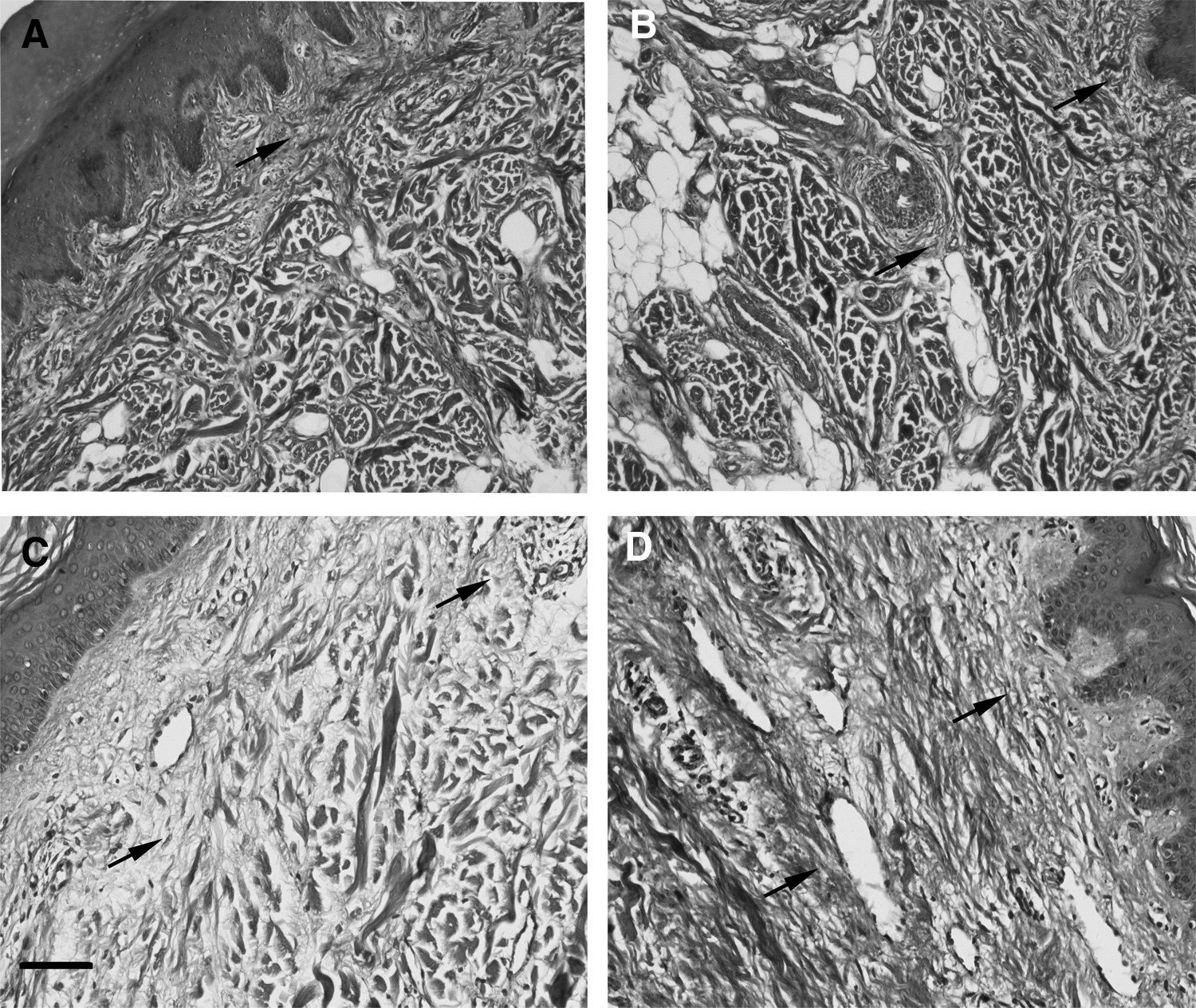
Images of collagen in Masson-stained skin sections. The staining of collagen was blue (black arrows).
Increasing skin stiffness with increasing severity of SLE of the lower limb
Skin stiffness was significantly greater in lymphedematous than normal skin. In patients with Stage I SLE, the mean skin stiffness of the lymphedematous limb was 0.0711 ± 0.0087 N and the mean skin stiffness ratio was 0.0744 ± 0.0516. Both were significantly higher than the corresponding values of the control limbs (0.066 ± 0.0085 N and 0.0326 ± 0.0228, respectively; both p < 0.01). The mean skin stiffness was 0.1089 ± 0.0183 N and 0.1605 ± 0.0304 N in patients with Stage II and Stage III disease, respectively; the mean ratios in these two groups being 0.4144 ± 0.2937 and 1.0168 ± 0.4767, respectively. In both Stage II and Stage III disease, the values were significantly higher than those of the control (p < 0.01, each). Furthermore, skin stiffness tended to increase from Stage I to Stage III SLE. The mean stiffness and mean stiffness ratio of the lymphedematous limbs were significantly higher in patients with Stage III than in those with either Stage I or Stage II disease (both p < 0.01) (Fig. 3).
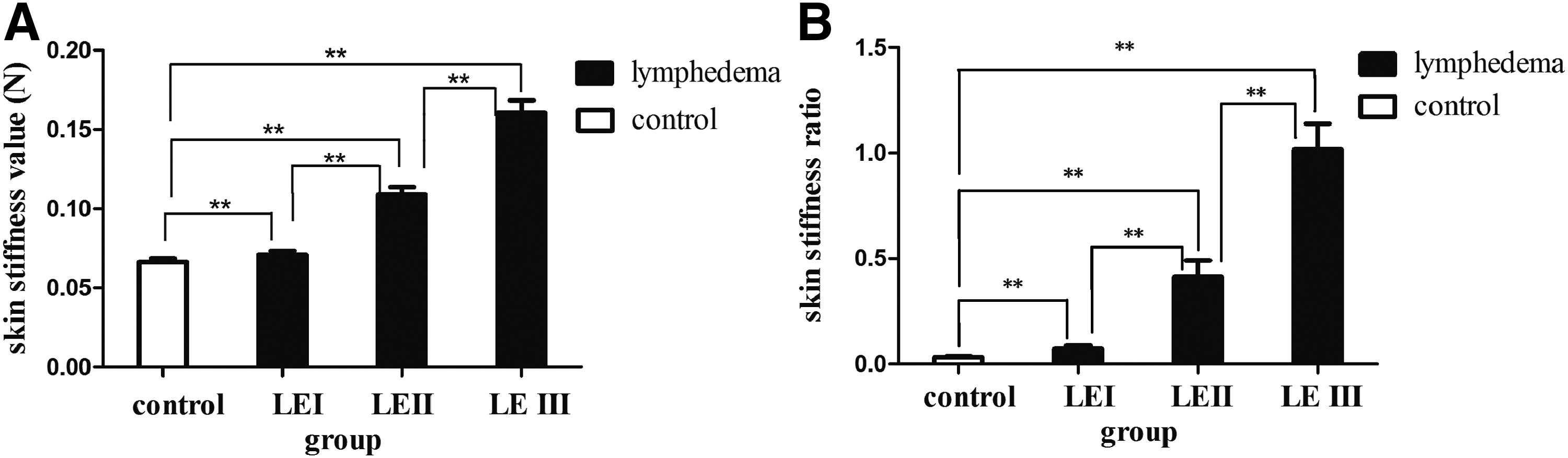
The skin stiffness value
Increasing circumference ratio and interstitial fluid ratio with increasing severity of SLE of the lower limb
The circumference and amount of interstitial fluid were both significantly greater in lymphedematous than in normal limbs. In patients with Stage I SLE, the circumference ratio of the lymphedematous limb was 0.0175 ± 0.0063 and the interstitial fluid ratio was 0.0426 ± 0.038. Both were significantly higher than the corresponding values of the control limb (0.0048 ± 0.0039 and 0.0037 ± 0.002, respectively; both p < 0.01). In patients with Stage II SLE, the circumference and interstitial fluid ratio of affected limbs were 0.1001 ± 0.0525 and 0.2622 ± 0.1608, respectively; both values differed significantly from those in the control group (both p < 0.01). In patients with SLE Stage III, the circumference and interstitial fluid ratios were 0.236 ± 0.0039 and 0.592 ± 0.2559, respectively, both being significantly higher than the corresponding values in the control group (both p < 0.01) (Fig. 4).
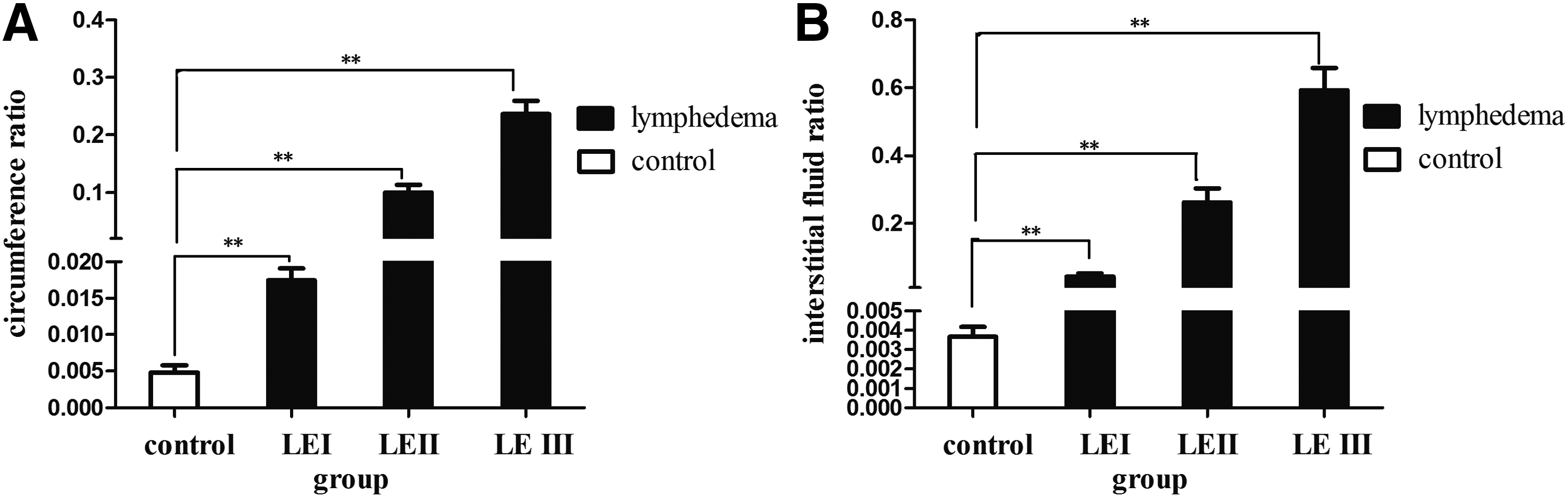
The circumference ratio and
Skin stiffness ratio correlates positively with circumference and interstitial fluid ratios in lower limbs with SLE
A statistically significant positive correlation was observed between the skin stiffness and circumference ratios in lymphedematous limbs (r = 0.649, p < 0.01) (Fig. 5A). The skin stiffness ratio also positively correlated with interstitial fluid ratio in the lymphedematous limbs (r = 0.699, p < 0.01) (Fig. 5B). Thus, in edematous limbs, the higher the values for circumference and interstitial fluid, the harder the skin.
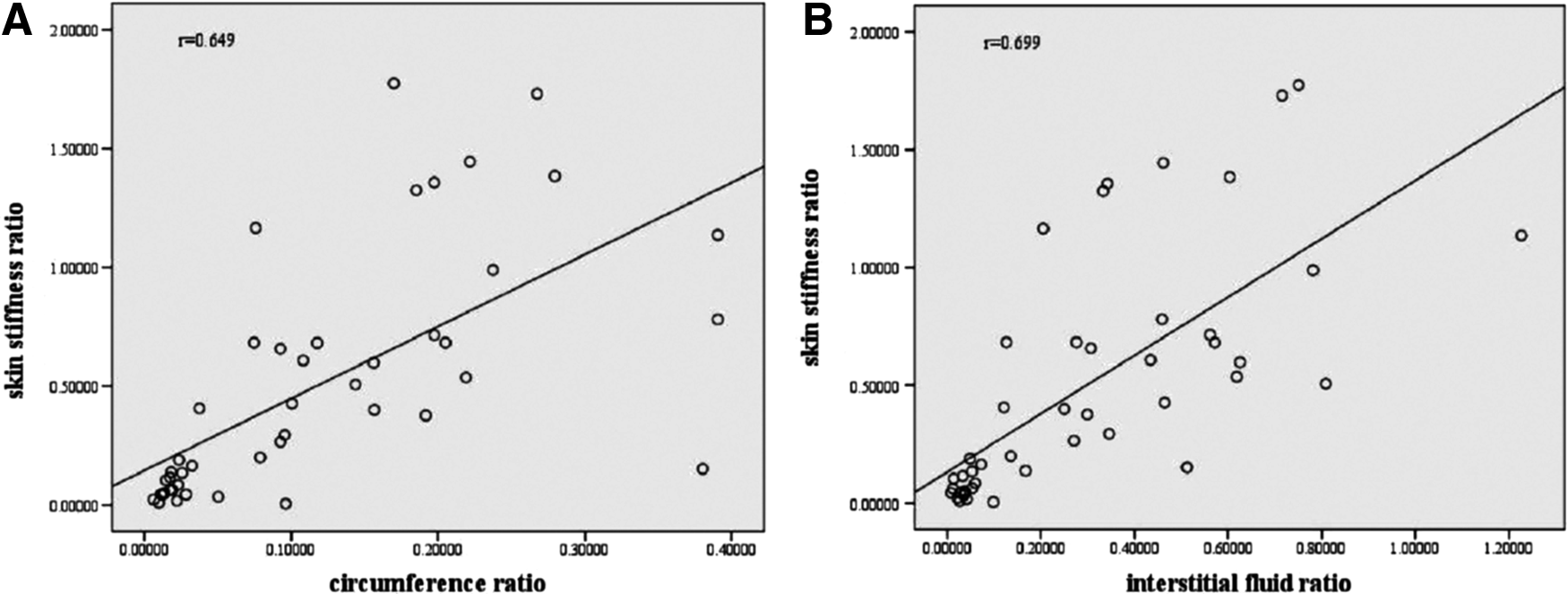
The scatter plots of positive correlation between the skin stiffness ratio and circumference ratio
Skin stiffness correlates positively with stage of lower limb SLE
The skin stiffness value and ratio of lymphedematous limbs were* significantly positively correlated with LE stages (r = 0.9, p < 0.01; r = 0.81, p < 0.01, respectively). From SLE Stage I to Stage III, the edema in the affected lower limb was more severe and the skin correspondingly harder (Fig. 6).

The scatter plots of correlation between the skin stiffness value and LE stages
Discussion
Skin fibrosis is one of the most important pathological changes in limbs with SLE. The diagnosis and assessment of skin fibrosis have been challenging, mainly because of the absence of an appropriate method of diagnosing the stage of SLE. In this study, we investigated the use of the SkinFibroMeter to accurately evaluate skin stiffness in patients with SLE of the lower limb. Our results clearly show that this portable instrument provides diagnostically valuable information on the severity of skin fibrosis in the lymphedematous lower limb.
Fibrosis arises from the deposition of large amounts of collagen in lymphedematous skin. 7 Examination of skin specimens taken from the lower limbs of patients with SLE Stages I, II, and III revealed a gradual increase in the expression of collagen that paralleled the severity of SLE. Abundant collagen deposition consistent with fibrosis was seen in the dermis, especially in patients with Stage II and III disease. Previous studies showed that increased collagen deposition reduced skin elasticity, resulting in hardening of the skin. Thus, skin stiffness reflects the degree of fibrosis: the stiffer the skin, the more severe the fibrosis.22–24
We here showed that the SkinFibroMeter can quantitatively evaluate the severity of skin stiffness and thus facilitate the assessment of fibrosis in patients with SLE. Higher values indicate stiffer skin and more severe fibrosis. In this study, we compared normal with lymphedematous skin of patients with different stages of SLE. We found that the normal stiffness value is 0.066 ± 0.0085 N and that this value gradually increased in parallel with severity of SLE. In patients with Stage I, palpation of the skin of the affected lower limb showed it to still be soft and elastic, however, the stiffness value and ratio were higher than the corresponding values for normal skin. Furthermore, the circumference and interstitial fluid ratios were also higher. Thus, already in early-stage disease, some areas of the skin become hard and fibrotic. This result is consistent with the study of Földi and Földi, 25 who reported that fibrosclerotic changes are present only locally and the swollen skin is still soft in the Stage I disease. This mild swelling and localized skin stiffness can escape the notice of the patient and her physician, easily resulting in a missed diagnosis. In the absence of early intervention, SLE may progress to Stage II, which is characterized by pitting edema, greater circumference of the affected limb, and harder skin. 26 We measured skin stiffness values and ratios and showed that both are significantly higher beyond Stage I, implying that skin fibrosis is more severe. This is consistent with the findings of a previous study which showed that, in Stage II SLE, increased fibroblast proliferation and collagen deposition result in a loss of skin softness and development of swelling and fibrosis. 27 In Stage III, the symptoms and signs of edema are more obvious, tissue fibrosis causing further hardening of the skin and a loss of its normal elasticity, and increases the likelihood of infection, ulceration, and hyperkeratosis. 28 The significant increases in skin stiffness values and ratios measured by the SkinFibroMeter reflect these changes in the skin and Spearman analysis demonstrated they correlated positively with SLE severity. Based on these results, we recommend the use of a SkinFibroMeter to measure stiffness and thus accurately diagnose and classify fibrotic skin at any stage of SLE.
In the clinic, measurements of the circumference and interstitial fluid ratio of the affected limb are conventional examinations, additional information being obtained by more sophisticated methods, including lymphoscintigraphy, ultrasound, and MR lymphography, to diagnose SLE stage.29–32 Of interest, stiffness ratio correlates positively with circumference and interstitial fluid ratio. Many previous studies have demonstrated that, as the disease progresses, an overload of lymph results in dysfunction and dilation of lymphatic vessels, causing lymphatic fluid stasis within them. Leakage of this fluid into the interstitial space results in swelling of the lymphedematous limb and an increase in its circumference.21,33 Prolonged stasis promotes infiltration by microbes and failure to eliminate specific antigens and plasma proteins is a timely manner. These immunogenic substances induce a chronic inflammatory reaction in which monocyte and macrophage release inflammatory cytokines, such as transforming growth factor-β1 (TGF-β1), tumor necrosis factor-α, interleukin (IL)-6, and IL-8.20,34,35 These cytokines, particularly TGF-β1, stimulate deposition of collagen and extracellular matrix, leading to fibrosis and the hardening of the skin that are characteristic of SLE. This sequence of events explains why measuring stiffness is an effective method to diagnosis SLE, similar to determinations of limb circumference and the interstitial fluid ratio. In addition, the SkinFibroMeter can also be used to monitor the effect of treatment, for example, evaluating the fibrotic skin after manual lymphatic drainage and bandage compression therapy.
The SkinFibroMeter has other advantages; namely, it is highly sensitive, portable, and accurate. Unlike diagnostic methods based on skin biopsy and puncture, SkinFibroMeter measurements are noninvasive and do not damage skin structures, thus reducing patient anxiety. Also, the wireless data collection system uses DMC software, thus enabling real-time data acquisition and storage. Measurement is easy to perform, requiring only depression of the operation button and adjustment of the power and velocity of the probe.
Taken together, we have shown that the SkinFibroMeter is very sensitive and accurate for detecting skin fibrosis of edematous limbs. Therefore, this new instrument is a promising prospect for diagnosis and assessment of skin fibrosis in patients with lower limb SLE.
Footnotes
Acknowledgments
This study was supported by the Chinese National Science Foundation (grant number 81272146), the National Key Specialty of Clinical Plastic Surgery Project, and the Shanghai Key Specialty of Clinical Reconstructive Surgery Project.
Author Disclosure Statement
No competing financial interests exist.