
Abstract
Abstract
Background:
Intermittent pneumatic compression (IPC) is a widely used lymph drainage therapy that can be performed at home. However, the effectiveness of IPC for lymph drainage remains unclear. The aim of this study is to investigate the real-time change in the lymph flow velocity during IPC and consider which mode and pressure are best for treating lower limb lymphedema.
Methods and Results:
Eight lower left limbs of 8 healthy volunteers and 17 lower limbs of 15 secondary lymphedema patients were investigated. Indocyanine green lymphography was performed with the subject covered with a transparent six-chambered IPC garment. The IPC treatment was administered in several modes (sequential or nonsequential inflation mode, sequential or interrupted deflation mode, and under high or low pressure). Using a brightness intensity analysis software program, the real-time change in the fluorescence intensity during the treatment was recorded and graphed. The maximum inclination of the graph between 2 seconds in the inflation phase (SLOPE) and the mean SLOPE value of all subjects (average SLOPE) were calculated. The average SLOPEs of each mode of treatment were then compared. The average SLOPEs were also compared between patients with mild and moderate lymphedema. There were no significant differences among the SLOPEs in the healthy group. However, in the patient group, the average SLOPE was significantly higher in the sequential inflation mode as well as under high pressure than in the nonsequential inflation mode. On comparing the mild and moderate lymphedema groups, the average SLOPE tended to be higher in the mild group; however, the difference was not statistically significant.
Conclusions:
Sequential programs and high pressure resulted in a faster lymphatic flow than other modes. These results suggest that a greater treatment effect could be obtained by adjusting the mode of treatment and the pressure of IPC.
Introduction
S
In 2010, Adams et al. reported direct evidence of the improvement of lymphatic function in normal and breast cancer-related lymphedema (BCRL) of the upper limbs using IPC and indocyanine green (ICG) lymphography. 2 Three normal control subjects and six women diagnosed with unilateral BCRL were investigated. IPC garments were placed around the trunk, chest, and arm, and ICG lymphography was performed before, during, and after the treatment. The fluorescent packets were counted to calculate the rates of lymphatic propulsion (number of propelled packets over a period of time) and apparent lymph velocity (velocity of each packet). They also checked the lymphatic vessel recruitment (appearance of new linear lymph vessels after the treatment) and proximal advancement of ICG.
Using these factors, the authors evaluated the lymphatic function before, during, and after the IPC treatment. ICG lymphography was performed not only on the affected/treated side but also on the contralateral/untreated side to evaluate both the local and systemic effect of IPC on the lymphatic system. In the control subjects, the rate of lymphatic propulsion increased after the treatment and lymphatic vessel recruitments were observed. In the affected arm of the lymphedema subjects, proximal advancement of ICG was observed after the treatment. In addition, in both the control and lymphedema subjects, lymphatic propulsion on the untreated side increased during and after the treatment. Based on these results, the authors concluded that IPC was effective in stimulating the lymphatic function locally and systemically.
However, in their study, the rate of propulsion and the velocity could not be analyzed due to obscuration caused by dermal backflow (DBF; diffuse and dense dermal dyeing caused by abnormal filling of the lymph capillaries). Furthermore, both in the control and lymphedema subjects, the real-time evaluation of the treated side during the treatment was impossible because the device covered and hid the limb.
In this study, which targeted the lower limbs, we investigated real-time lymph flow on the treated side during IPC and the difference in the velocity of the lymph fluid among several modes of inflation and deflation, and with high and low pressure using a pneumatic compression device with a transparent multichambered boot and a video analysis software program. The aim of this study was to evaluate the real-time change in the lymph flow velocity during IPC and determine which mode and pressure were best for treating lower limb lymphedema.
Materials and Methods
Materials
The pilot study was performed on eight left lower limbs of eight healthy volunteers (one man and seven women). The mean age of the volunteers was 38 years (range, 22–53). None of the volunteers had subjective or objective evidence of lower limb edema or any history of trauma or surgery in their lower limbs, nor did they have cardiac, renal, or hepatic disease or undernutrition.
Based on the results of the pilot study, 17 lower limbs of 15 secondary lymphedema patients were included in the subsequent study. All of the patients were women. The mean age of the patients was 63 years (range, 39–83). There were 13 unilateral cases and 2 bilateral cases, including 10 right limbs and 7 left limbs. The primary diseases were gynecological cancer (n = 14) and colon cancer (n = 3), and the types of lymphatic damage were surgery including lymph node dissection (n = 10), surgery including lymph node dissection and additional irradiation (n = 5), and irradiation only (n = 2). The clinical stages according to the International Society of Lymphedema (ISL) were 3 stage I limbs and 14 stage II limbs.
The diagnosis was made based on the medial history, presence of edema of the lower limb, and abnormal findings such as DBF or collateral lymph pathways on lymphoscintigraphy. The severity was graded based on Maegawa's classification of lymphoscintigraphy (Fig. 1). 3 Thus, the severity was graded as type 1 (mild) in nine limbs, type 2 (mild to moderate) in five limbs, and type 3 (moderate) in three limbs. The 17 limbs were divided into 2 groups: a mild group, with 9 type 1 limbs (all limbs were ISL stage I), and a moderate group, with 8 type 2 limbs and 3 type 3 limbs (3 limbs were ISL stage I and 6 were ISL stage II).

Maegawa's classification of lymphoscintigraphy.
Type 4 (moderate to severe) and 5 (severe) limbs were excluded because it was impossible to perform the analysis due to intensive DBF or the absence of lymph vessels on lymphography in the observed region (the distal part of the lower leg). Patients who underwent surgery for lymphedema, such as lymphaticovenous anastomosis, were also excluded due to their altered lymphatic dynamics.
The following concomitant conservative therapies had been provided: MLD with an elastic stocking in the daytime (10 limbs), and MLD with an elastic stocking in the daytime and compression by a garment made of urethane sponge while sleeping (5 limbs); no concomitant therapies had been provided for 2 limbs. These 15 limbs (excluding the 2 untreated limbs) were treated by the same therapist, and all of them were in a maintenance phase of the treatment. The filming device was set up and a video analysis was performed by Author No. 2 (J.M.) in the pilot study, and the setup and analysis in the subsequent study were performed by Author No. 1 (S.K.).
Methods
Outline
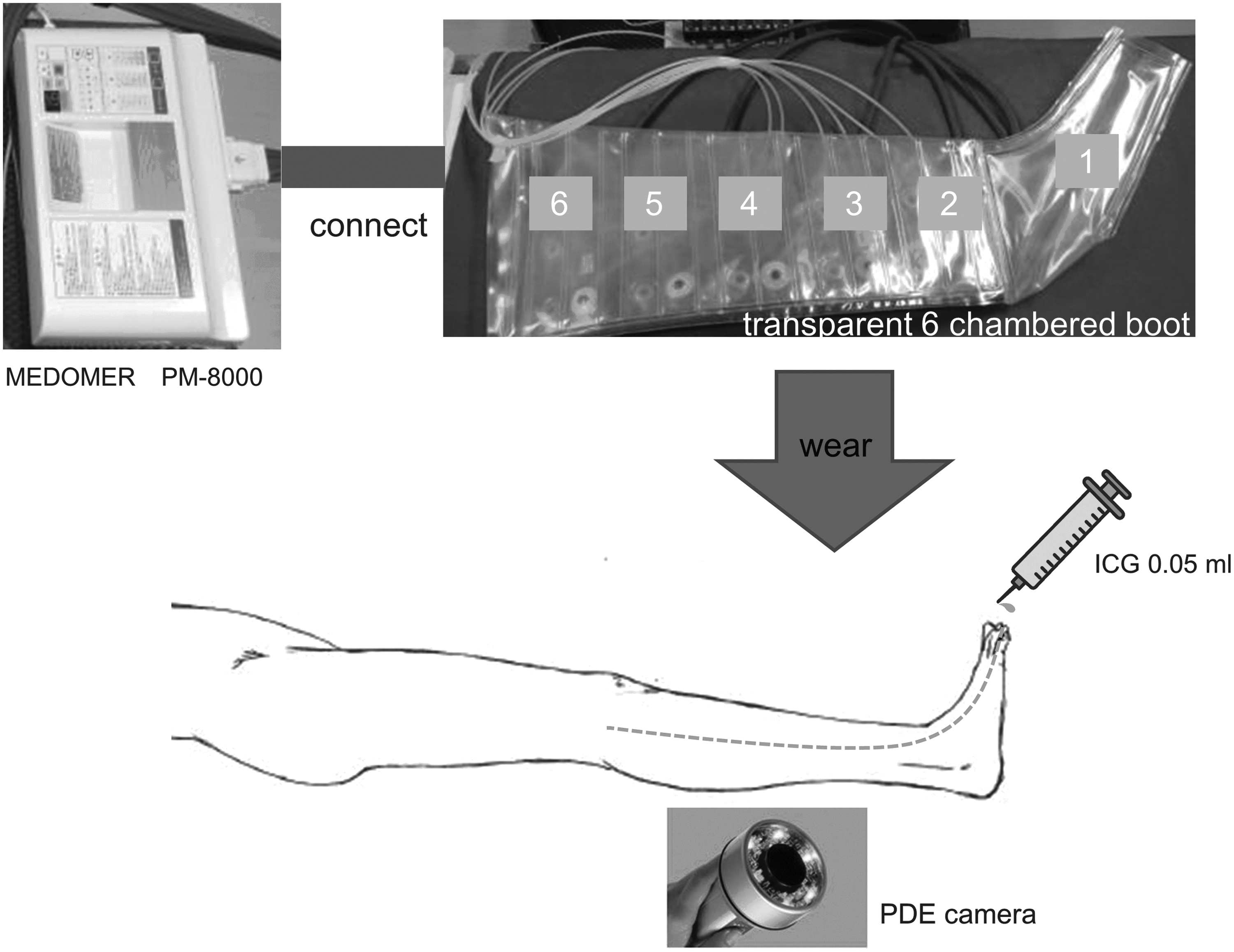
After assuming a supine resting position for 10 minutes, the ICG (0.05 mL) was injected intradermally into each interdigital area. We then checked the linear patterns of the lymph vessels using a near-infrared fluorescence camera system (Photo Dynamic Eye camera: PDE-neo; Hamamatsu Photonics K.K., Hamamatsu City, Japan). Normally, several superficial lymph vessels are detected at the dorsum of the foot. These join together to make one or two main collecting lymph vessels at the distal part of the lower leg and flow upward through the medial side of the lower limb.
We covered the lower limb with a transparent six-chambered (chambers 1–6 from the distal side to the proximal side) IPC garment and set the Photo Dynamic Eye (PDE) camera to observe chamber 2 (the distal part of the lower leg). The IPC treatment was then administered with several modes of inflation and deflation. As the garment was transparent, we were able to observe and record the fluorescence change in real time during the treatment (Figs. 2 and 3).
Settings.
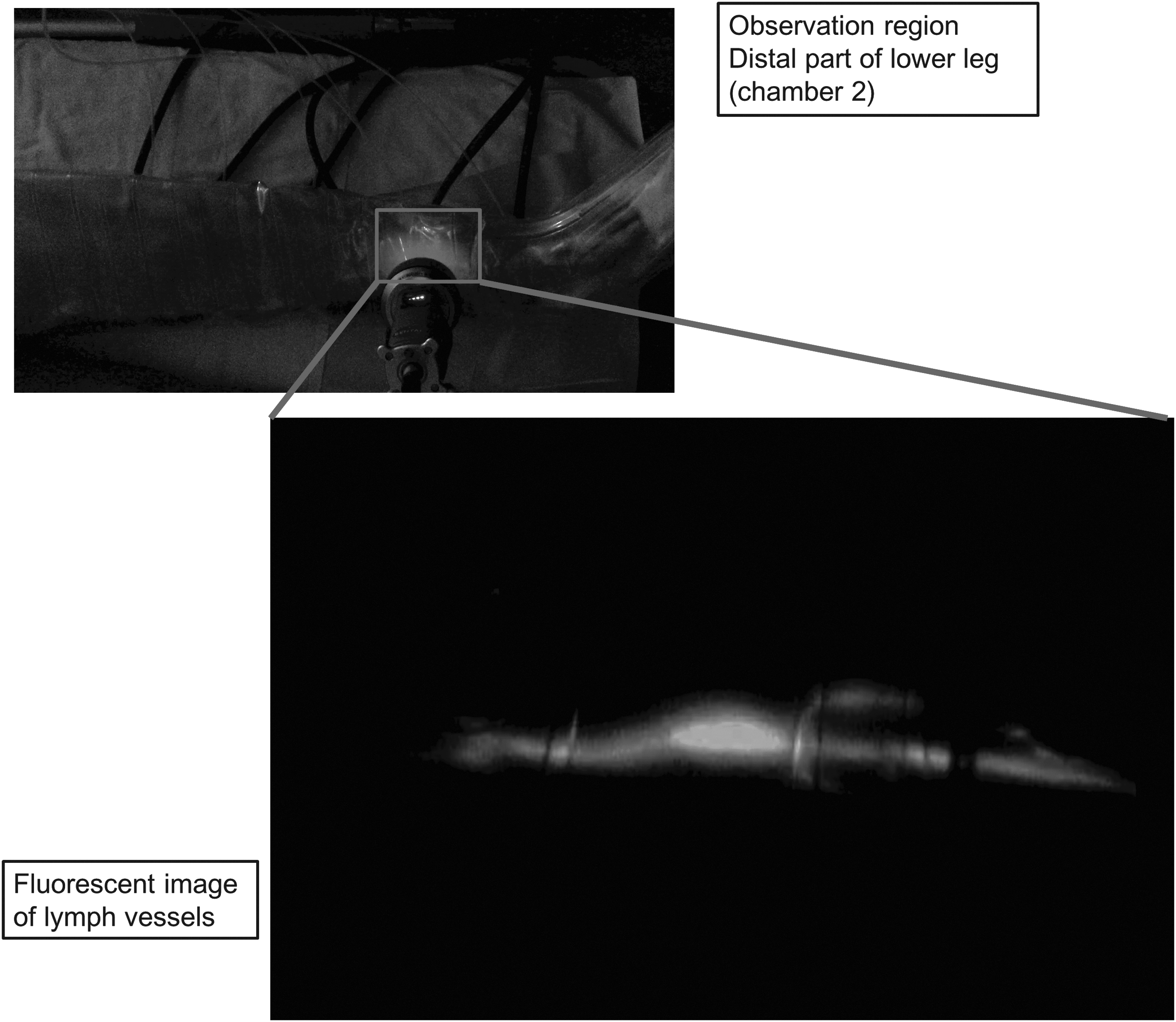
Observation region and fluorescent image of lymph vessels.
We subsequently analyzed the change in the fluorescence intensity of the obtained videos to assess the effects of each mode of treatment. The treatment device was a MEDOMER PM-8000 (Nitto Kohki Co., Ltd., Tokyo, Japan). PM-8000 has multichambered programmable pumps, which provide sequential inflation and deflation of freely selected order and pressure. Such devices with adjustability and expanded programs are called advanced pneumatic compression devices (APCDs). Conventional PCDs typically consist of a simple single-chambered pump that provides static nonsequential compression to the whole limb. A video analysis software program (ROIs ver. 2.0; Hamamatsu Photonics K.K.) was used to analyze the fluorescence changes.
The modes of treatment
We evaluated two modes each for inflation and deflation. The modes of inflation were hyper (HP) mode, in which the whole lower limb was compressed simultaneously, and squeeze (SQ) mode, in which the limb was compressed sequentially from chambers 1 to 6 (distally to proximally). The modes of deflation were A mode and B mode. In A mode, the lower limb was decompressed sequentially from chambers 6 to 1. In B mode, the chamber decompression sequence was 6, 4, 2, 5, 3, and 1. The duration of the inflation and deflation was set to 30 and 20 seconds, respectively.
The pressure was set at 90 mmHg in the pilot study. Given that the pilot study analysis revealed that lymph flow accelerated under lower levels of pressure, we performed the subsequent study at both 45 and 90 mmHg. Thus, there were four modes of treatment (90 mmHg: HP-A, HP-B, SQ-A, SQ-B) in the pilot study, and eight modes of treatment (45 and 90 mmHg: HP-A, HP-B, SQ-A, SQ-B) in the subsequent study (Fig. 4). These treatment modes were applied for three cycles of inflation and deflation.

Modes of treatment.
The video analysis
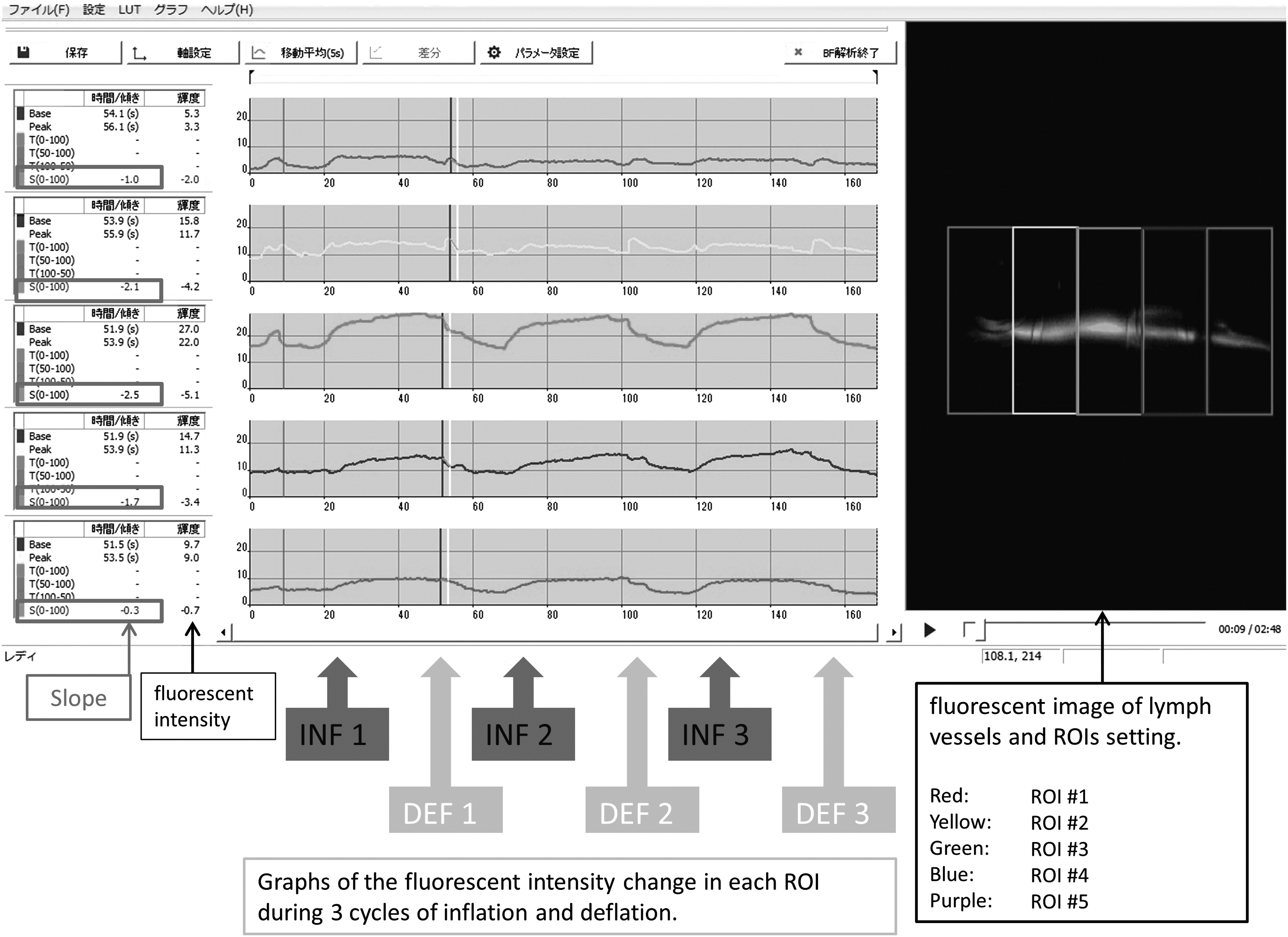
Using the video analysis software program, the contrasted lymph vessels in the regions of interest (ROIs) were visualized as fluorescent lines that were divided into five cells of identical size (ROIs #1–5 [proximal to distal]). The mean fluorescence intensity in each ROI was sampled every 0.2 seconds to graph the change in brightness (Fig. 5). The maximum inclinations between 2 seconds in the inflation phases (three times; INF 1 to INF 3 in Fig. 5) in each graph were calculated. Subsequently, the mean value of these three inclinations (the SLOPE) was calculated, reflecting the velocity of the lymph flow of each subject in each mode of treatment (SLOPE dimension: “fluorescent intensity change per second”).
The video analysis.
We focused on the mean SLOPE value of all subjects (average SLOPE) as the parameter for assessment. The inclination in the deflation phase was also observed, but we decided not to adopt it as a parameter for the following reasons: fluctuations in the fluorescence intensity are the superimposed outcome of passive flow generated by IPC treatment and active, physiologic, and spontaneous flow reflecting the contractile activity of lymph vessels. Given that the contractile activity of the lymph vessels differs among individuals depending on age, gender, and the degree of lymphatic obstruction or dysfunction, it could conceivably become a source of bias in the evaluation, especially in the deflation phase. Therefore, fluctuations in the fluorescence intensity in the deflation phase may not reflect the therapeutic effectivity.
In contrast, the fluorescence changes in the inflation phase are mainly generated by the increasing speed of lymph flow during squeezing. The SLOPE of the inflation phase therefore seems to reflect the effect of IPC directly. We compared the average SLOPE of each mode of treatment as well as between the patients with mild and moderate lymphedema.
Student's t-test was used for the statistical analyses. p-Values of <0.05 were considered to indicate statistical significance.
Informed consent was obtained from all of the patients, and the study was approved by the Yokohama City University of Medicine Ethics Committee.
Results
Healthy volunteer group
Lymph vessels were visualized as fluorescent lines at the medial side of the distal lower leg, and the real-time fluorescence change during IPC treatment was observed in all subjects. In healthy subjects, there was no significant difference in the change among the modes of treatment (Fig. 6).
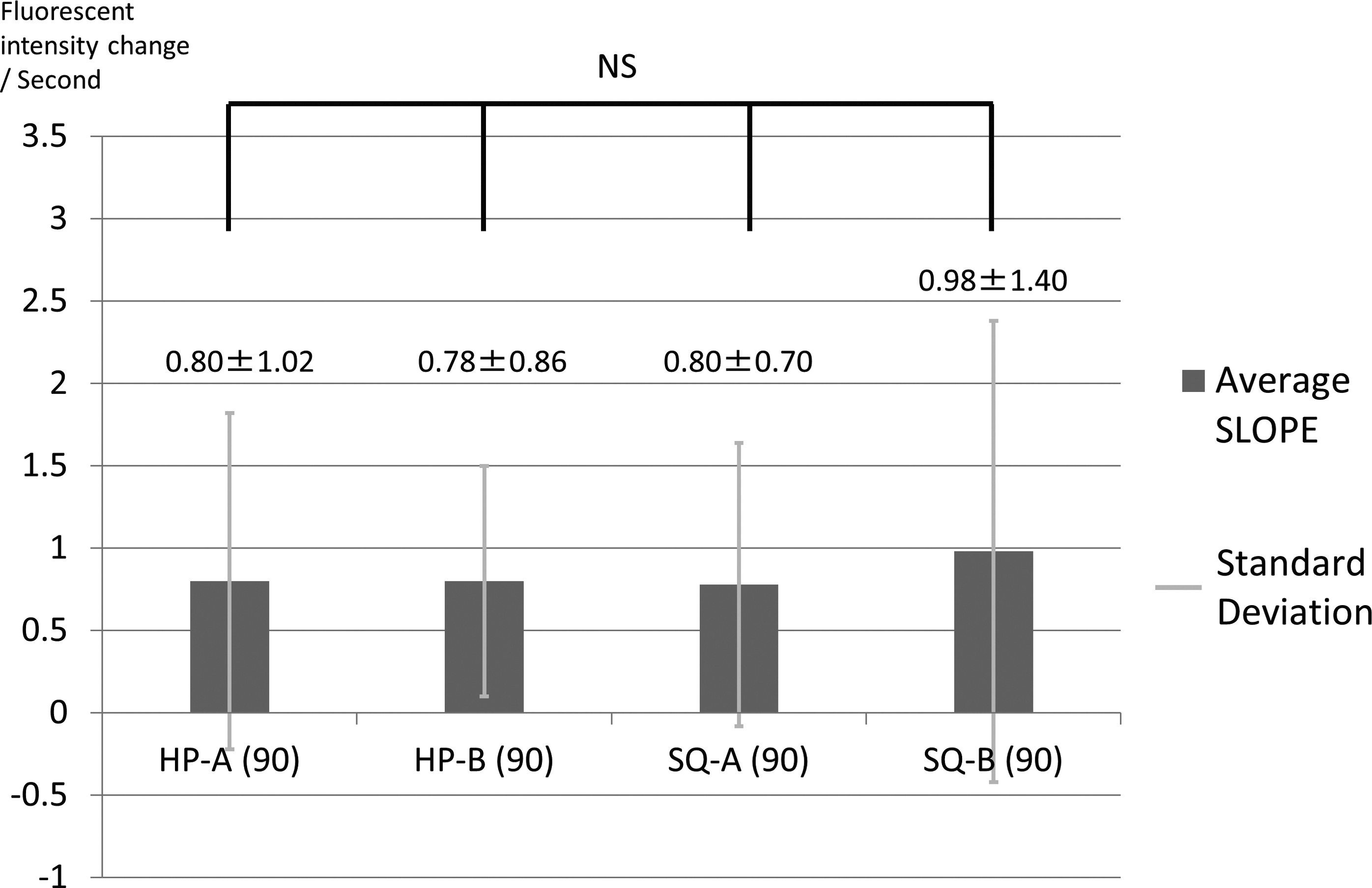
The results in healthy subjects and a comparison among treatment modes.
Lymphedema patient group
Unlike the healthy group, lymph vessels were not detected on the medial side of the distal lower leg in seven subjects in the lymphedema patient group. In such cases, the collateral lymph vessels were detected at the lateral or frontal side of the distal leg. DBF appeared at the thigh or knee in many of the type 1 and 2 cases and spread to the proximal part of the lower leg in three type 3 cases, indicating the progression of congestion. Nevertheless, lymph vessels were detected as linear patterns at the distal lower leg, and their fluorescence change was observable.
The average SLOPE was significantly higher in the SQ mode than in HP mode, regardless of the mode of deflation (Figs. 7 and 8). In addition, the SLOPE was significantly higher under high pressure (90 mmHg) than low pressure (45 mmHg) in the SQ mode (Fig. 9). On comparing the mild and moderate lymphedema patients, the average SLOPE was generally higher in the mild group, but the difference was not significant (Fig. 10). These results suggested that, in lower limbs with lymphedema, faster lymph flow could be obtained with sequential inflation and under higher pressure.
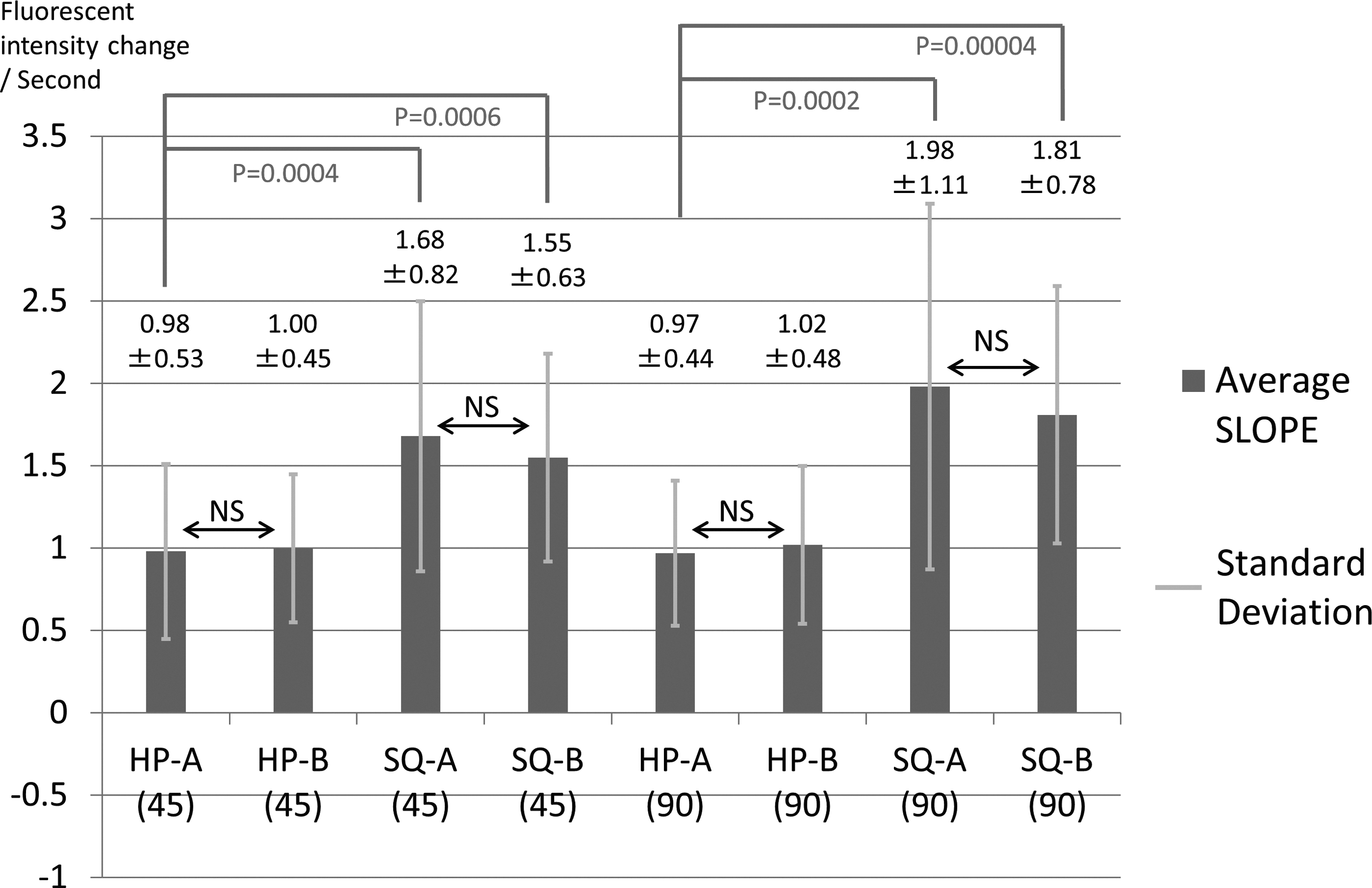
The results in lymphedema subjects and a comparison among treatment modes (1).

The results in lymphedema subjects and a comparison among treatment modes (2).

The results in lymphedema subjects and a comparison between pressures (45 mmHg vs. 90 mmHg).
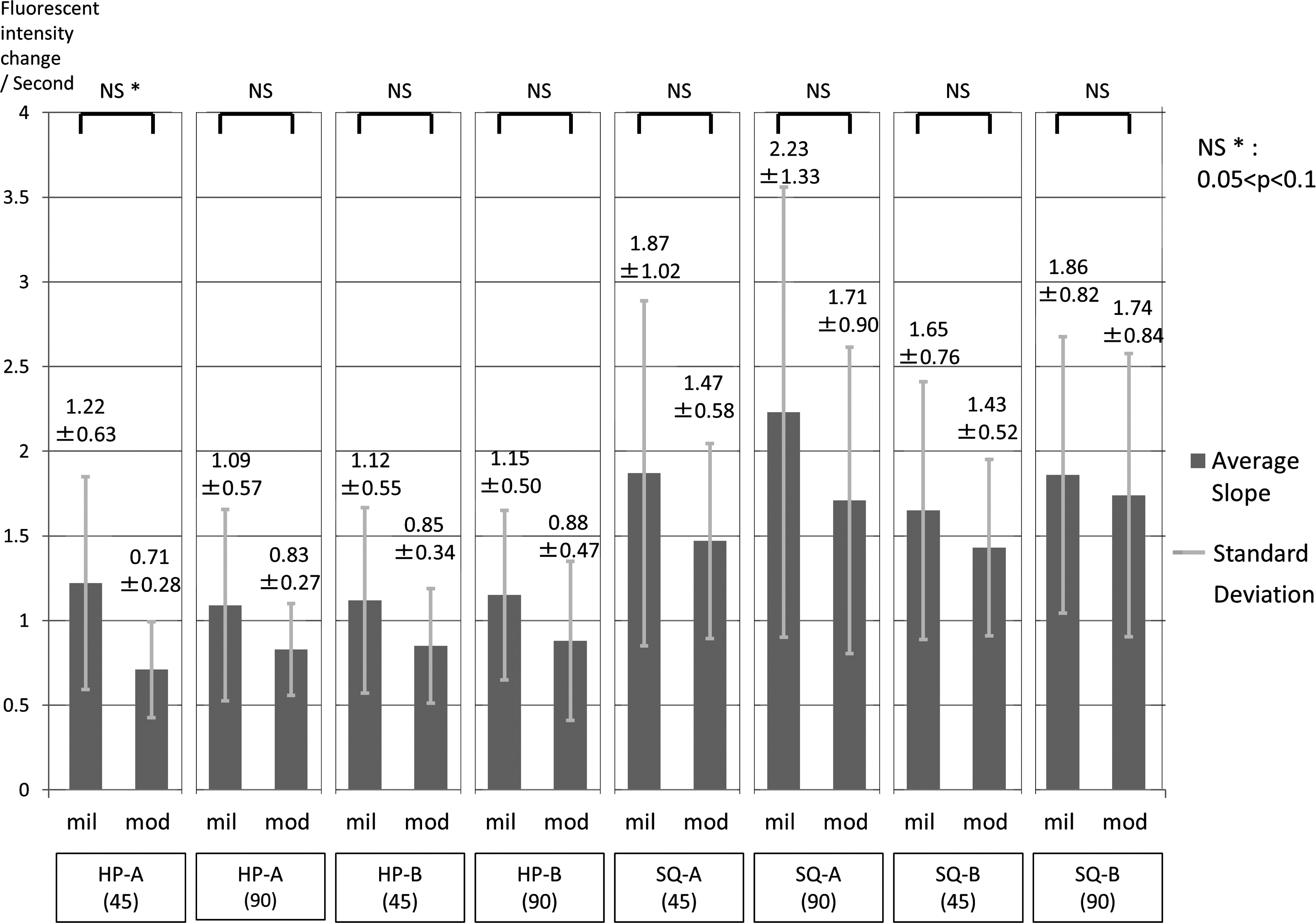
The results in lymphedema subjects and a comparison between severity.
Discussion
ICG lymphography was first reported by Unno et al. in 2007 as a novel imaging technique for diagnosing lymphatic disorder. 4 Subsequently, several investigations concerning the utility, benefits, and applications of ICG lymphography have been reported; for example, it has been used for diagnosing and classifying lymphedema based on various abnormal findings5–14 ; for the evaluation of the lymphatic function, such as lymph transportation capacity, or the lymph pump function or circulation15–22 ; and for the detection of functional lymph vessels before and during the surgery and assessment of the results of the surgery.23–29 Given the above-mentioned advantages, ease of performance, safety, and low invasiveness, ICG lymphography is now enjoying widespread use.
ICG lymphography shows different distribution and morphology in normal and lymphedema limbs.4–6 In normal limbs, continuous lymph vessels are observed from the injection site to the groin, along the medial aspect of the lower limb, called a normal linear pattern. However, in lymphedema limbs, diffuse and dense dermal dyeing appears in various parts of the limb, caused by abnormal filling of the lymph capillaries in a process termed DBF.
With the progression of lymphedema, the DBF patterns are divided into splash, stardust, and diffuse patterns based on the morphological characteristics.6–8,13 Although DBF usually spreads in the proximal to distal direction in conjunction with the progression of the lymphatic obstruction and dysfunction, in limbs with congenital lymphatic disorder or hypoplasia, it can spread from the distal direction or not appear at all.12,14 These findings regarding the morphology and distribution of DBF are useful for evaluating the severity of lymphedema and determining the treatment strategy.
Several investigations concerning the evaluation of the lymphatic function using ICG lymphography have been reported.15–22 Unno et al. measured the lymph pumping pressure (cuff pressure when the contrast agent exceeded the upper border of the cuff) and transit times (time for the contrast agent to reach the knee or groin) to assess the lymph function.15–17 Yamamoto et al. analyzed the lymph transportation capacity (ICG velocity and transit time) of lymphedema limbs using dynamic ICG lymphography.21,22 The results of these studies indicate that the lymph pump function decreases as the lymphedema severity progresses.16,19,21,22 In addition, the function differs depending on the age and gender. 17
In this study, we set two patterns for the deflation mode. However, we did not adopt the inclination of the deflation phase as an assessment parameter because considerable individual differences in the lymph pump function could have affected the results. The results of this study showed that the average SLOPE was higher in the SQ mode than in HP mode, regardless of the mode of deflation. We therefore concluded that, at the very least, the lymph flow during inflation was unaffected by the deflation patterns antecedent to the inflation.
ICG lymphography can be used for various lymphatic investigations. However, to our knowledge, the previously mentioned report by Adams et al. is the only study to have evaluated the direct effect of IPC using ICG lymphography. In that study, the DBF or the device itself obstructed the propulsion and velocity analyses, and real-time evaluation on the treated side. Regarding the details of IPC, such as the number of chambers, modes of inflation and deflation, treatment time, number of cycles, and pressure, the methods adopted in different studies have varied widely, and no consensus on these parameters has been reached thus far.30–32
Therefore, in our study, we used a transparent garment and enrolled relatively mild lymphedema limbs without DBF in the distal lower leg to evaluate the real-time change in the lymph flow. In addition, IPC was performed with two modes of inflation and deflation under two pressure settings to compare the lymph flow velocity. We found that the change in the lymph flow velocity differed between the healthy group and the patient group. In the healthy group, the average SLOPE value was not markedly different between the modes of treatment. However, the SLOPE was significantly greater in the SQ mode than in HP mode in the patient group. One reason for this discrepancy in findings is the difference between the two groups in the ease of lymph flow.
Given that healthy limbs have good automatic lymph transport capability, sufficient lymph flow can be achieved without compression; as such, the mode of inflation has little effect on the flow. In contrast, given that lymphedema limbs lack automatic lymph transport capability due to the presence of congestion, valve insufficiency, and degeneration, there is little lymph flow without compression. Patients with lymphedema are therefore affected by the mode of inflation. In the SQ mode, the distal to proximal sequential compression of the chambers prevents the backward flow of lymph, resulting in a higher degree of fluorescence intensity change. APCDs offer an SQ mode. Some reports indicate that the lymph drainage effects of APCDs are superior to those of conventional PCDs, which offer only an HP mode.33,34
The pressure was set to 90 mmHg in the pilot study. However, the video analysis showed that lymph flow accelerated early in the inflation phase (under less pressure). Accordingly, less pressure may be needed to obtain superficial lymph drainage. Therefore, in the subsequent study of lymphedema patients, we used pressures of 45 and 90 mmHg. Nevertheless, the results showed that the average SLOPE was significantly higher under high pressure than under low pressure in the SQ mode.
The high internal pressure in the lymph vessels due to degeneration or congestion may affect the ease of flow. Zaleska et al. measured the subcutaneous internal pressure during IPC using the wick-in-needle technique. They noted that high pressure (80–120 mmHg) was necessary to obtain effective tissue fluid pressure (30 mmHg) and the tissue fluid pressure differed at various levels, depending on the conditions of the soft tissue. 35 Therefore, higher pressure may be required in cases with progressed fibrosis. In the HP mode, the backward flow might reduce the influence of high pressure.
Some authors have claimed that too much pressure can cause adverse events, such as lymph vessel injury, inflammation, and genital swelling 36 ; however, there has been no obvious evidence to support these claims.32,37 In this study, no such events occurred; however, a few subjects complained of an oppressive feeling under 90 mmHg of pressure. We feel that it is better to use IPC under high pressure to obtain good lymph drainage, but we should consider reducing the pressure in mild cases of lymphedema or when patients experience pain under high pressure.
We expected that the average SLOPE would be lower in the more severe cases than in the mild cases because of their strong congestion. A comparison of the average SLOPE in the mild and moderate groups revealed that the values in the mild group were higher for all modes of treatment; however, the difference was not statistically significant. It is necessary to detect a linear pattern at the distal part of the lower leg to analyze the fluorescence change. Therefore, in this study, we enrolled subjects with relatively mild lymphedema without DBF in the distal lower leg. Many of the subjects in the moderate group had type 2 limbs in which congestion was localized at the thigh. This may have affected our findings.
A comparison of the average SLOPE values between normal subjects and patients would have been interesting. However, we did not conduct this comparison because the settings for the filming device and the video analysis were established by the respective observers. As the average SLOPE was affected by these factors, it was difficult to compare the data obtained from different observers. Future studies should focus on this issue and conduct such a comparison.
Few studies have focused on direct evidence of the effects of IPC. We showed direct evidence of the real-time effects of IPC on lymph flow and the difference in the lymph velocity of the different modes of inflation and deflation. A programmed sequential mode of treatment with high pressure was the most effective in achieving faster lymphatic flow. The results of this study suggested that a greater treatment effect could be obtained by adjusting the mode of treatment and the pressure of IPC.
The subjects investigated in this study achieved passively accelerated lymph velocity by the IPC treatment. However, faster lymph flow does not necessarily give a greater therapeutic effect. Parameters such as increase in the light intensity after the IPC treatment would be more meaningful to assess when evaluating the therapeutic benefits. However, given the results of several previous reports, there is a considerable possibility that IPC improves the lymphatic function both locally and systemically.2,18,20 An accelerated lymph flow stimulates the lymphatic systems and might trigger functional improvement. The correlation between the real-time lymph velocity and change in the fluorescence intensity after the IPC treatment might be meaningful for underscoring this point.
ICG lymphography is useful for providing direct evidence of lymph flow. Further investigations will be required to create a better treatment protocol.
Footnotes
Acknowledgments
This study was funded by Nitto Kohki Co., Ltd. and was supported by grants from the Ministry of Education, Culture, Sports, Science and Technology (Japan) NN 24591914.
Author Disclosure Statement
No competing financial interests exist.