
Abstract
Abstract
Introduction:
Aberrant, altered, or blocked lymphatic drainage may contribute to the high recurrence rate of breast cancer. Thus, an efficient evaluation of lymphatic drainage from the breasts and/or upper limbs is essential in the management of lymphedema and in ipsilateral primary or contralateral recurrent breast cancer patients. There are very few reports of lymphatic drainage to the paravertebral lymph nodes in patients with a lymphedema after breast cancer surgery with or without reconstruction.
Methods:
We used lymphoscintigraphy to examine lymphatic drainage in a case series.
Results:
We observed five patients with upper limb and/or mammary lymphedema (after breast cancer surgery with or without reconstruction) who had lymphatic drainage from the upper limb or breast to the posterior intercostal and/or paravertebral lymph nodes. One patient also presented with nodal relapse at the time of our investigation.
Conclusions:
The cases from this study demonstrate the unusual, and mostly unrecognized, lymphatic drainage pathways toward lymph nodes, which may be at risk for further evolution of breast cancer.
Introduction
T
Materials and Methods
The local ethics committee of the Jules Bordet Institute provided ethical approval for this study. The study was conducted in accordance with the Declaration of Helsinki from 1975 and revised in 2008.
Lymphoscintigraphy
A well-standardized protocol was followed for radionuclide upper limb lymphangiographies. The patients laid on a gamma camera table with their upper limbs resting. They were injected subcutaneously in the first interdigital space of each hand with one tenth of a vial of Human Serum Albumin (HSA) nanosized colloids (Nanocoll R, GE Healthcare, Belgium) labeled with 2 milliCuries (mCi) of 99mTc in a volume of 0.2 mL. The technician prepared the injections by adding 20 mCi of 99mTc-O4 in 2.0 mL in one vial of Nanocoll and then filled two tuberculin syringes with 0.2 mL each after labeling. Using a dual-head single-photon gamma camera equipped with a parallel-hole, all-purpose low-energy collimator, planar images (anterior and posterior views) of the injected sites, the forearms, elbows, arms, and axillae, were obtained after 30 minutes with the limbs in resting conditions (phase 1), after 15 minutes of hand-gripping (phase 2), and after 1 hour of normal activity (phase 3) (for one example, see Fig. 5a). Dynamic images centered on the axillae were also acquired during phase 1 and 2. Single-photon emission computed tomography (SPECT/CT) was performed when available (for technical consideration about SPECT/CT acquisitions and processing see Supplementary Appendix available in the online article at www.liebertpub.com/lrb). Additional intradermal injections of radiocolloids (0.4 mL of the same vial used for previous injections) were later given using tuberculin syringes. The injections were primarily at the level of the upper and external part of the edematous arm (“phase 4”) and/or secondarily at the level of the homolateral mastectomized anterior chest wall (usually on the midclavicular line under the scar of the mastectomy), and/or at the level of the edematous breast (in the midpart of the inferior breast in line with the nipple) (“phase 5”). Images were obtained directly after the injections as well as after stretching and massaging the injection site.
Results
The clinical characteristics of the investigated patients and the results from lymphoscintigraphy are summarized in Tables 1 and 2.
ALND, axillary lymph node dissection; BL, breast lymphedema; Breast rec., breast reconstructed; L, lumpectomy; LySc inj., lymphoscintigraphic injection performed in the hand (H) and/or breast (B) and/or shoulder (S); M, mastectomy; ND, no data; Rel, exam performed at the time of one relapse; ULL, upper limb lymphedema.
Ax. leakage, lymphorrhea from the axilla toward the thoracic wall; Contralateral Ax LN, visualization of anterior drainage toward the contralateral axillary lymph node; Intercostal LN, visualization of drainage toward the posterior intercostal lymph node; Internal mammary LN, visualization of drainage toward the anterior internal mammary lymph node; Paravertebral LN, visualization of drainage toward the posterior paravertebral lymph node.
Case presentations
Patient 1
When the lymphoscintigraphic investigation was performed, this patient had developed an edema of the left upper limb and the breast 1 year after simple mastectomy and immediate reconstruction by implant combined with the transverse rectus abdominis muscle. Fifteen years before, she had undergone a lumpectomy and left ALND. There was no evidence of disease metastases in the 15 lymph nodes removed. The patient had received adjuvant radiotherapy and 5 years of tamoxifen. The lower panel of Figure 1 shows the anterior (left) and posterior (right) pictures, centered on the thorax and axillae, obtained after intradermal injection of the 99mTc HSA nanosized colloids in the left breast. On the anterior view, one lymphatic vascular drainage (from down to up arrows) can be seen from the injected site, toward and crossing the midline to reach the right contralateral axillary nodes, whereas three paramedian lymph nodes can be seen (from right to left horizontal arrows) on the posterior view. On the upper panel, the left lateral view (left) and the oblique posterior view (right) distinctly show (oblique arrows) at least two lymphatic vessels originating from the injected breast and running laterally and posteriorly to reach the lymph nodes.
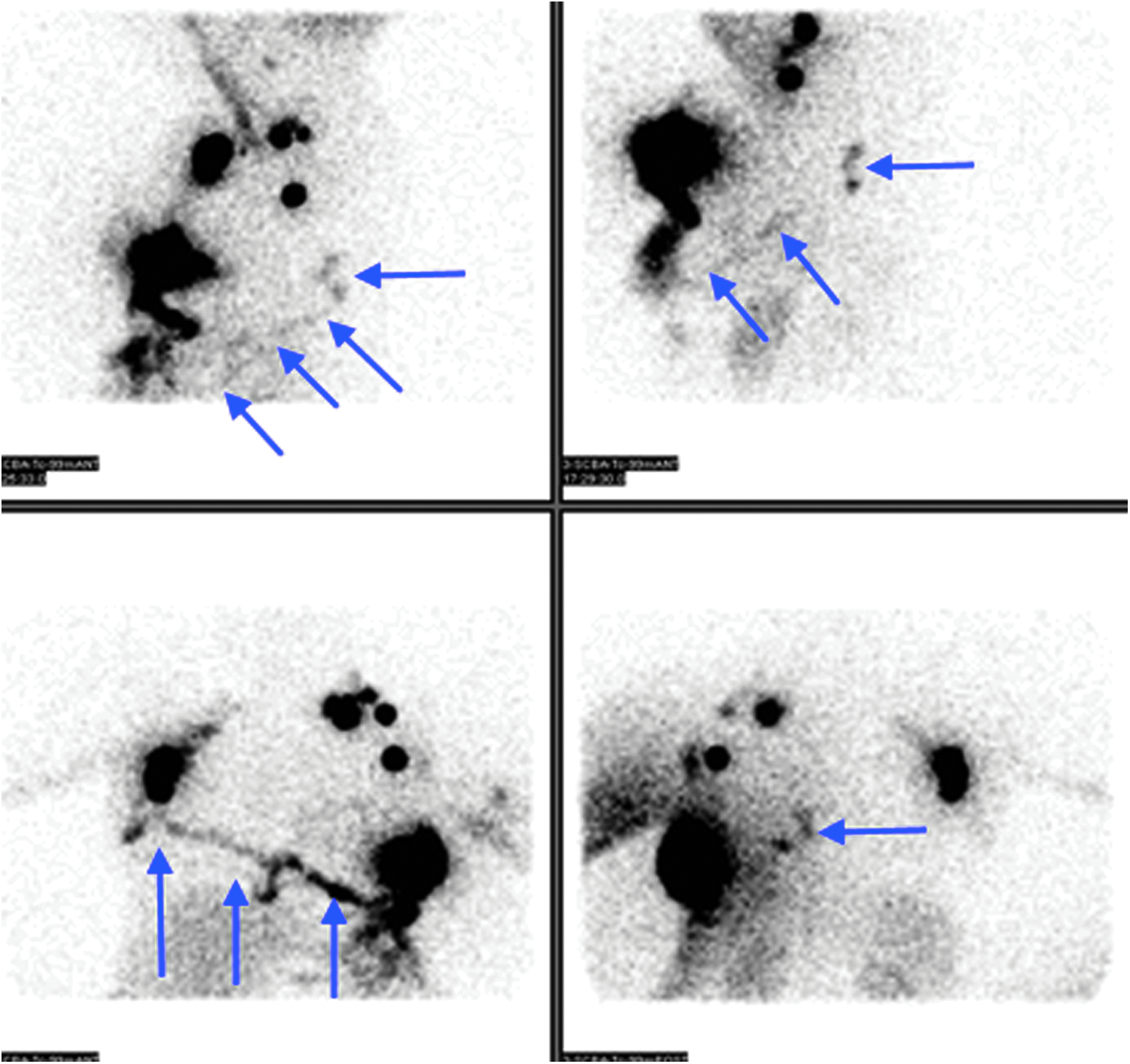
Anterior (left) and posterior (right) pictures centered on the thorax and axillae (lower panel) and left lateral (left) and left oblique posterior (right, upper panel) centered on the left axilla and lateral thoracic wall obtained after the intradermal injection of the 99mTc HSA nanosized colloids in the left breast of patient 2. HSA, human serum albumin.
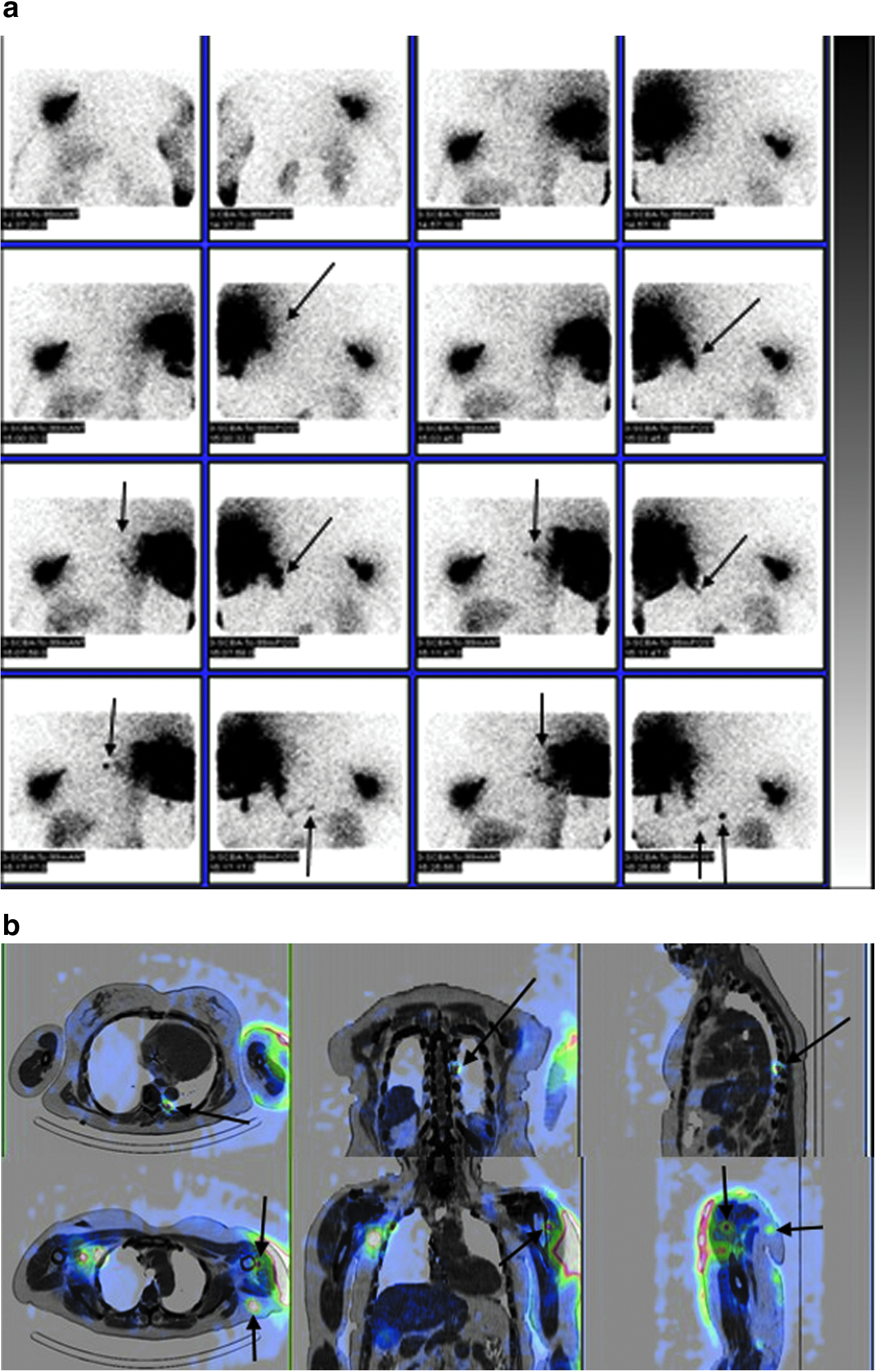
Patient 2
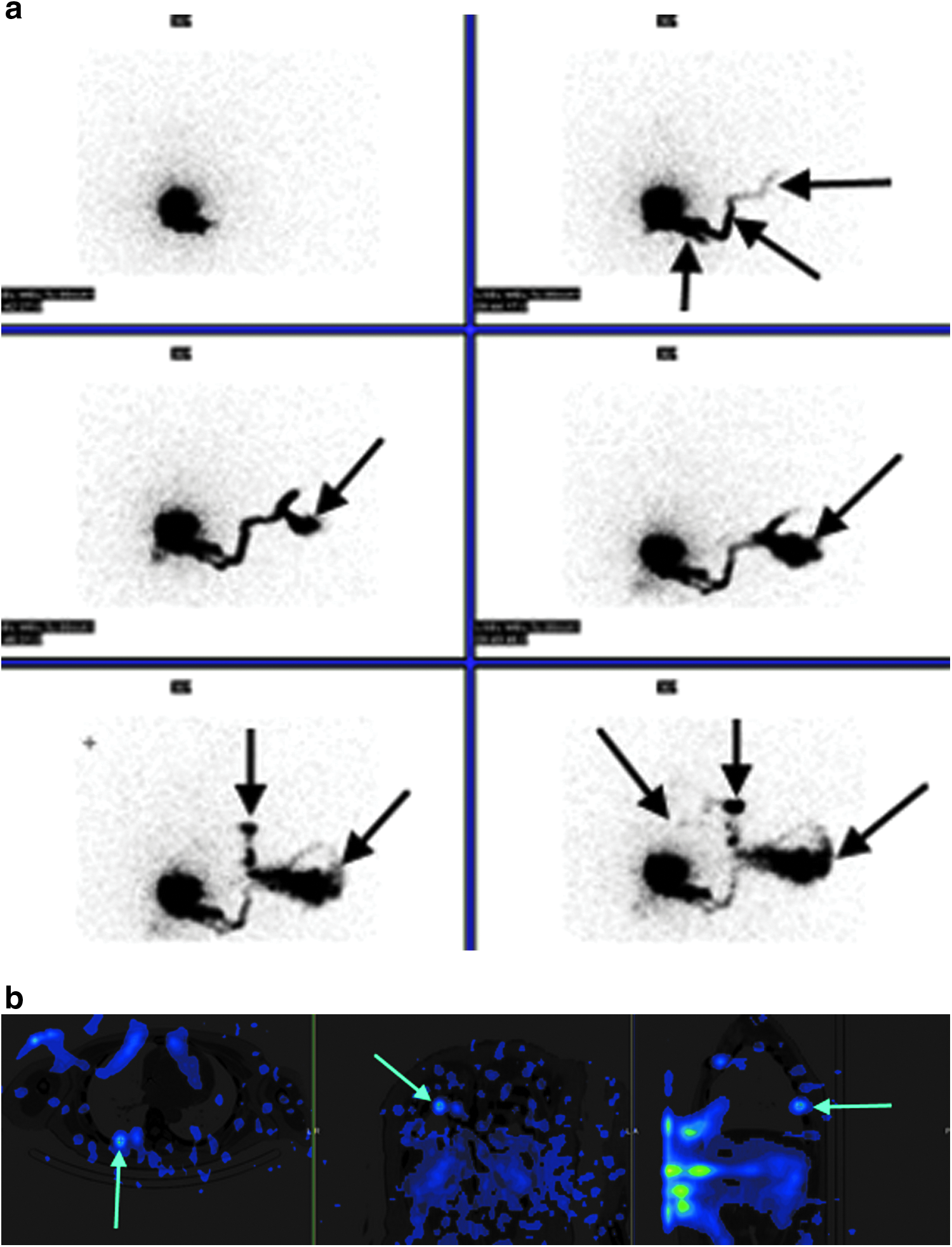
This patient was referred to the department of nuclear medicine because she developed an edema of the right breast and upper limb. Seven years before, she had a modified radical mastectomy and the ALND showed metastasis in 9 out of 27 resected nodes. The patient received adjuvant radiotherapy and hormonal therapies. She also had one reconstruction by implant combined with the transverse rectus abdominis muscle 2 years ago, but the implant was removed 1 year after because of infection. Her clinical examination showed that the right breast was edematous, but also the inferior part of her left breast. Her lymphoscintigraphic pictures were successively obtained (from left to right and up to down, Fig. 2a) after intradermal injection in the right breast. We first observed one lymphatic vessel running from the injected site horizontally toward the midline (from down to up vertical arrow), then running up (from down to up oblique arrow) and horizontally (horizontal arrow). In the next pictures (mid and lower panels), we can see the tracer flowing in the inferior part of the left breast (from up to down oblique arrows), but also one lymphatic drainage toward the parasternal nodes (from up to down vertical arrows). In the last picture, a faint focal activity can be seen above the injected site (from up to down and left to right oblique arrow) that is clearly demonstrated on the SPECT/CT images to correspond to one intercostal right side lymph node (see arrows on Fig. 2b).
Patient 3
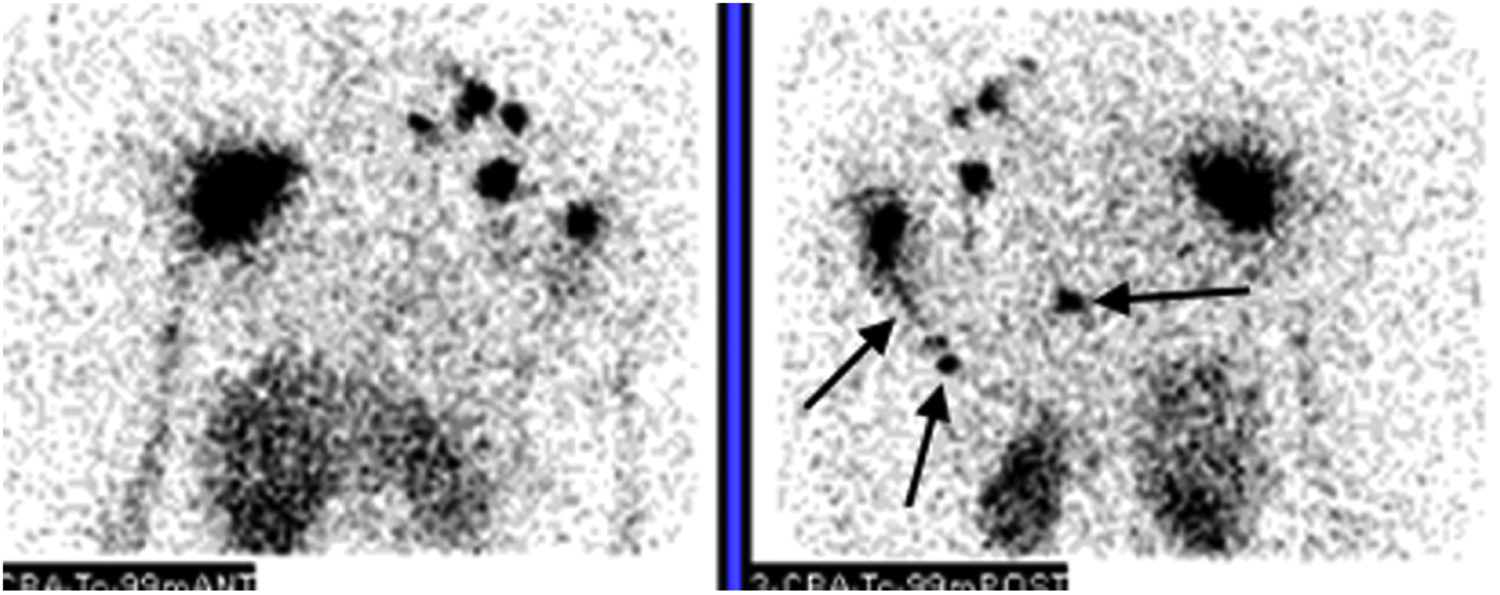
This patient developed an edema of the left upper limb 10 years after a left lumpectomy and ALND. She had received chemotherapy, radiation therapy, and tamoxifen. The anterior (left side) and posterior (right side) planar views (Fig. 3) were obtained with our last phase of imaging (after 1 hour of normal activity and after injection of the radiocolloids of the tracer in the first interdigital space of each hand). The anterior view shows “only” one abnormal distribution of the lymph nodes in the left axillary and supraclavicular areas, while the posterior view shows one lymphatic vessel originating from one inferior axillary lymph node (oblique arrow) and reaching (vertical arrow) one posterior lymph node (not seen on the anterior view), but also one right side paravertebral lymph node (horizontal arrow).
Anterior (left) and posterior (right) planar pictures obtained from patient 4 after 1 hour of normal activity (phase 3 pictures) and the subcutaneous injection of the radiocolloids in the first interdigital space of each hand.
Patient 4
This patient was referred to the department of nuclear medicine for her first investigation (Fig. 4a: left panel) because she developed an edema of the right upper limb at the same time that she presented with a second right axillary and infraclavicular recurrence. Nine years ago, she had a right radical mastectomy with ALND, which showed metastasis in five of nine lymph nodes resected. Six years ago, she had a reconstruction by deep inferior epigastric perforator flap. Three years ago, she had a recurrence in the right axilla treated by excision (the final pathology revealed metastasis in two out of four lymph nodes resected). Her second investigation (Fig. 4a: right panel) was performed 9 months after the first one because her lymphedema had worsened.
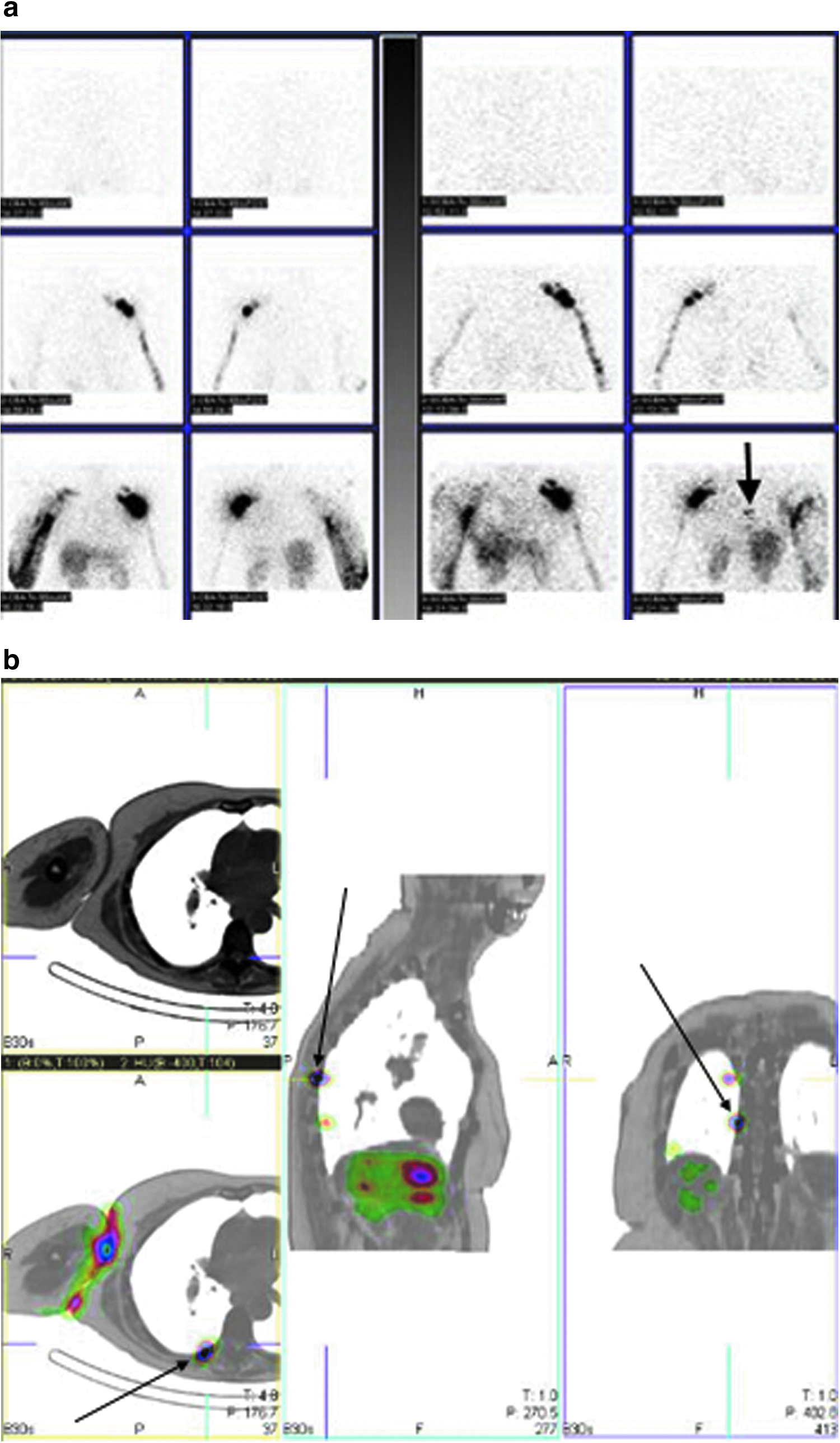
Her first investigation (Fig. 4a: left panel) showed only vascular lymphatic drainage and progression of the tracer through the superficial collateralization lymphatic network (at the level of the shoulder) up to the root of the right upper limb. Her second investigation (Fig. 4a: right panel) showed (vertical arrow), in her last posterior view, the appearance of two foci of activity corresponding to at least one paravertebral lymph node on the SPECT/CT images (Fig. 4b).
Patient 5
This patient was referred to the department of nuclear medicine because of worsening of her edema that affected her left upper limb 4 years after one lumpectomy with ALND. At the end of our classical lymphoscintigraphic investigation, we observed (Fig. 5a) one progression of the tracer through the superficial lymphatic collateralization network (from the hand to the root of her left limb, at the level of the external part of her left shoulder, and no lymph nodes in the left axillary and/or supraclavicular areas). The intradermal injection of the radiocolloids showed (Fig. 5a) not only anterior drainage of the shoulder toward the apical axillary and supraclavicular lymph nodes (Fig. 5b: vertical arrows) but also one posterior lymphatic drainage toward the lateral part of the thoracic wall (oblique arrows), which drained toward one paravertebral lymph node (see from down to up vertical arrows).
Discussion
The lymphoscintigraphic observations were obtained in patients who presented with upper limb lymphedema that was associated with mammary lymphedema. The flow direction of lymph in the chest wall or truncal areas is considered ambiguous and easily influenced or changed by mastectomy, radiation, ALND and lymph node status, and/or reconstruction, and varies greatly from patient to patient.1,3,4,13–17 In our limited series, these factors may have influenced the lymphatic drainage toward the posterior paravertebral nodes in three patients (1, 2, and 4). However, in the two other, no influencing factor was found.
Visualizations of drainage of the thoracic wall (and of the breast) toward the homolateral and/or heterolateral internal mammary and the heterolateral axillary lymph nodes are well documented 1 (three of the five patients in this series). The lymphatic drainage of the upper limb and/or the thoracic wall toward posterior intercostal and/or paravertebral lymph nodes that we observed in five patients was previously reported only by two authors.18,19 Kreel and George 18 described one breast cancer patient who had benefited from mastectomy and radiotherapy 4 years before. During an evaluation of her severe upper limb edema, they visualized one paravertebral lymph node (and one lymph node in the opposite axilla) with their delayed imaging, 10 days after lymphangiography with injection of contrast agent in the upper limb. Lymphatic drainage from the skin of the back to the paravertebral nodes in the thorax was also described by Uren et al. 19 during a preoperative lymphoscintigraphic investigation to locate the sentinel lymph node in patients with a melanoma on the back.
Our observations might be important from an oncological point of view. Contralateral axillary metastasis is the easiest to diagnose and has an incidence around 3.6%–6%.20,21 It occurs mainly by lymphatic spread in most, if not all, patients and not by hematogenous spread. This contralateral axillary metastasis can be the only site of metastasis and may occur either at the time of diagnosis of breast cancer or months or years later. These aberrant drainage pathways were significantly more frequent after a previous ALND than after a previous SNB. Although, the description by Uren et al. 19 of a direct lymphatic drainage from a melanoma on the back to paravertebral lymph nodes in the thorax was obtained preoperatively when detecting the sentinel lymph nodes. This finding suggests that these extra-axillary drainage pathways might represent clinically significant drainage. This risk is highlighted by our patient 4, who was examined by lymphoscintigraphy to evaluate the lymphonodal evolution of her cancer. The intercostal and paravertebral lymph nodes are at risk for further nodal evolution of the disease. Although this drainage may be uncommon, it might have important implications when detected for clinical management and early detection of any recurrence. These lymph nodes are not readily accessible for surgical biopsy and their pathological status might only be suspected if they are enlarged on CT and/or hypermetabolic in a PET-CT investigation with 18F-DG (to the best of our knowledge, this has not been reported in the literature, but such localizations may exist). On the other hand, these aberrant drainage pathways might also be important in the management of lymphedema. Lymphedema is a possible complication following axillary node surgery and is treated mostly with physical therapy and manual lymphatic drainage (MLD), pressotherapy (PT), and multilayered bandaging (MLB). 22 In cases like these, those treatments could work, but should be adapted to the patient because of the limitations of the techniques. The PT and MLB can only be applied to the forearm and the arm, leaving the shoulder and the thoracic wall without treatment. MLD could be a valid treatment option. The physiotherapist might follow the aberrant drainage pathways on the shoulders and the thoracic wall, and open new routes of drainage. 23 Although, if the aberrant drainage pathway is far beneath the skin, the physiotherapist will have difficulties stimulating the lymphatic system. In these cases, physical treatment should therefore be adapted to the patient's lymphatic system. The PT and MLD should be efficient in the management of the superior edema and MLD should be applied on the superficial lymphatic pathways indicated on the images of the thoracic wall and shoulder. Although, what we observed in this study corresponded to deep lymphatic draining pathways, for which superficial MLD is not effective. Some other therapeutic approaches might be helpful, like reinforcement exercises of the back, stretching, respiratory exercises, and fasciatherapy. 22
Two patients in our series had mammary edema and were injected intradermally in the edematous breast. These edematous breasts may represent the first sign of one malignant mastitis. If the patient presents thereafter with either a cutaneous relapse or second primary, the ipsilateral and/or contralateral internal mammary and/or axillary lymph nodes have to be considered sites for further evolution of the disease as well as the posterior intercostal and/or paravertebral lymph nodes. From a technical point of view, it has to be stressed that the use of SPECT/CT lymphoscintigraphy was helpful in at least one case (patient 2) to detect and/or resolve such unusual drainage toward intercostal and/or paravertebral lymph nodes.
Conclusions
In conclusion, these five cases illustrate that using lymphoscintigraphy ± SPECT/CT in patients with lymphedema of the upper limb/breast at the time of the nodal evolution of their mammary cancer can show lymphatic drainage in the ipsilateral and/or contralateral axillary, and/or internal mammary lymph nodes, as well as toward the intercostal and/or paravertebral lymph nodes. Surgeons, radiotherapists, physiotherapists, and medical oncologists should consider the therapeutic implications of these findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.