
Abstract
Abstract
Background:
Prolongation of survival in patients with breast cancer due to early diagnosis and modern methods of treatment has turned the attention on lymphedema, which is the most important morbidity secondary to the treatment of the disease. Determination of lymphedema and related risk factors in patients before a surgical intervention may provide protection for patients and early treatment. The aim of this study was to determine the presence of lymphedema before surgery by bioimpedance analysis in patients with breast cancer and to establish risk factors associated with lymphedema.
Patients and Methods:
A total of 277 patients who were diagnosed as having breast cancer, were planned to undergo a surgical intervention, and had no clinical lymphedema were included in the study. The presence of lymphedema was evaluated with clinical examination, measurement of arm circumference, and bioimpedance analysis.
Results:
Lymphedema was found in 59 (21.3%) patients with no detected differences in arm circumferences. A significant relationship was found between the presence of lymphedema and body mass index (BMI), number of positive lymph nodes, and capsule invasion of the tumor (p = 0.001, p = 0.003, p = 0.002, respectively). Multiple regression analysis revealed that BMI and the number of positive lymph nodes were independent variables (p = 0.024, p = 0.002). ROC curve analysis resulted in an increased risk of preoperative lymphedema when the number of positive lymph nodes was ≥8. Correlation analysis revealed a positive correlation between the number of positive lymph nodes and L-dex score (p = 0.001, r = 0.219).
Conclusion:
Preoperative bioimpedance analysis demonstrated that ∼1/5 of the patients had subclinical lymphedema. Preoperative subclinical lymphedema is associated with obesity and the number of positive lymph nodes, and thus, treatment of the axilla in patients who are preoperatively detected to have subclinical lymphedema should be revised.
Introduction
P
The development of lymphedema in patients who underwent no ALND and received no radiotherapy suggests the presence of other factors that might be effective in the etiology of lymphedema. These are high body mass index (BMI); chemotherapy, especially regimens that include taxane; advanced disease stage; breast cancer at the side of the dominant arm; and no regular physical activity of the patient. 10 The differences in lymph flow in other extremities of patients who developed lymphedema due to breast cancer have been demonstrated in some recent studies.11–16 These results also suggest the role of genetic predisposition in the development of lymphedema.
The classic methods used in the diagnosis of lymphedema have not been of much help in the diagnosis of subclinical lymphedema and may cause a delay in treatment. 17 Bioimpedance analysis determines the difference in the amount of extracellular fluid between two extremities by measuring the tissue resistance of the extremities against alternating electric flow. The diagnosis of subclinical edema is possible by this means, and development of marked lymphedema can be prevented by education, preventive measures, and early treatment.17–19
Development of subclinical lymphedema before axillary surgery in patients who are diagnosed as having breast cancer may be explained by the blockage of the lymph flow of the metastatic lymph nodes in these patients.20,21 Detection of lymphedema preoperatively should suggest the development of a much more marked lymphedema following ALND. No study was encountered in the literature search related with preoperative lymphedema and causal risk factors. The aim of this study was to preoperatively detect whether lymphedema was present using bioimpedance analysis in patients with breast cancer who were found to have no lymphedema using classic methods. In addition, we analyzed causal factors in patients who were detected to have lymphedema.
Patients and Methods
A total of 277 patients with breast cancer who were diagnosed as having early-stage breast cancer and treated at the Istanbul Florence Nightingale Hospital, Breast Health Center, between 2012 and 2015, were included in this study. The clinical evaluation of the patients was performed by a specialist physician in physical medicine and rehabilitation. Symptoms of swelling and sense of heaviness in the arm were questioned and a physical examination of the musculoskeletal system was performed. Circumference measurements of the hand, arm, and forearm were performed at nine different points, 5 cm apart from each other. A difference in circumference of the two arms of more than 2 cm was accepted as presence of lymphedema.
Patients with accompanying diseases that might be the cause of edema such as heart failure, renal failure, and hypothyroidism; patients who had a pacemaker or a metal implant that interrupted the performance of bioimpedance analysis; patients who had undergone prior breast surgery, neoadjuvant chemotherapy (NAC), or radiotherapy; and patients with unavailable pathology reports were excluded from the study. Demographics (age, height, weight, and BMI) and pathologic parameters (number of lymph nodes resected, lymphovascular invasion, capsular invasion, and tumor stage) of the patients were evaluated and recorded.
A multifrequency bioimpedance analysis device (L-Dex U400; ImpediMed, Australia), which was developed for the measurement of the extracellular fluid, was used in the evaluation of bioimpedance. Information on bioimpedance measurement was reported in our previous study. 22 According to the results of the measurement, as dictated by the operating manual, values between −10 and +10 were accepted as normal and values below or above these levels were accepted as lymphedema. 22
Statistical analysis
IBM SPSS version 21.0 was used in the analysis of the data. Distribution analysis of the data was performed using the Kolmogorov–Smirnov test. 23 The Mann–Whitney U test and chi-square test were used as nonparametric tests and Fisher's exact test was used when chi-square conditions were unmet. Spearman's correlation test and the Kruskal–Wallis test were used in the correlation analysis and multivariate analysis, respectively. Analysis of independent parameters was performed using logistic regression analysis. p < 0.05 was accepted as significant.
Ethics board approval was obtained from the institution before beginning the study.
Results
The mean age and BMI of the 277 patients included in the study were 51.7 years (range 23–91 years) and 27.9 kg/m2 (range 19.2–42 kg/m2), respectively. No lymphedema was diagnosed in the clinical examination and circumference measurements of the arms. SLNB and axillary dissection due to a positive SLNB were performed in 144 and 133 patients, respectively. The patients were divided into two groups with and without lymphedema, as diagnosed using preoperative bioimpedance analysis. The two groups were compared with regard to age, BMI, surgical intervention, presence of lymph node involvement, and capsular invasion of the lymph node (Table 1).
L-dex values outside the range between −10 and +10 were accepted as presence of lymphedema.
ALND, axillary lymph node dissection; BMI, body mass index; SLNB, sentinel lymph node biopsy.
The correlation between the number of positive lymph nodes and bioimpedance values was found significant (p < 0.001, r = 0.219) (Fig. 1).
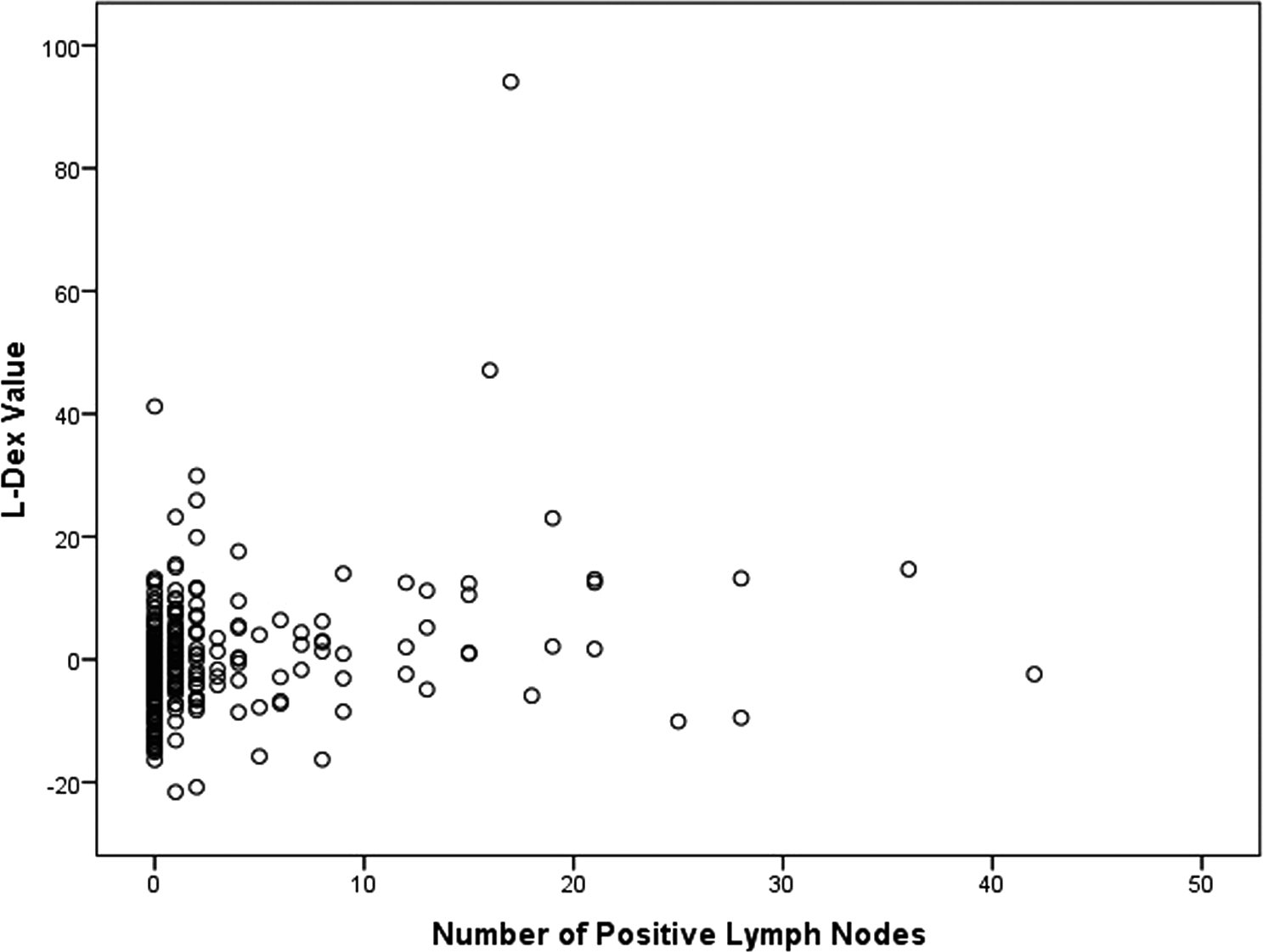
The correlation between the number of positive lymph nodes and L-dex values.
Rates of L-dex were found significantly different in patients with and without capsular invasion (p = 0.002).
L-dex values were found significantly lower in patients without involvement of lymph nodes (pN0) compared with those with positive lymph node involvement (pN+) when patients with and without lymph node involvement (pN0 and pN+) were compared (p = 0.03). With a subgroup analysis, a significant difference was found between pN0 and pN2 (p = 0.01), but no statistically significant differences were found between pN1 and pN2, and pN2 and pN3 (p = 0.21 and p = 0.12, respectively) (Table 1).
ROC curve analysis was performed to determine the relationship between L-dex positivity and the number of lymph nodes, and preoperative risk of presence of lymphedema was found to be increased in patients with ≥8 positive lymph nodes (Table 2 and Fig. 2).
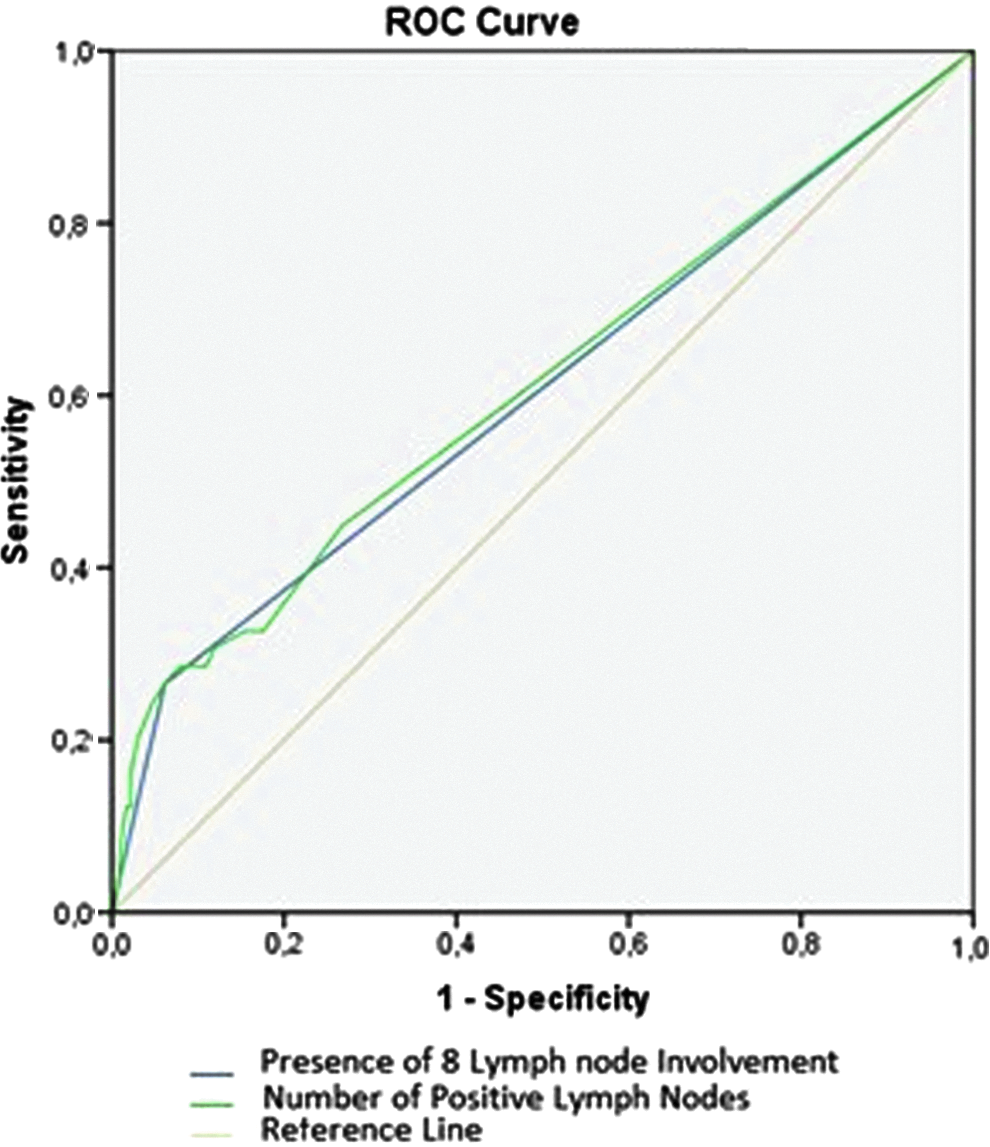
Sensitivity of preoperative lymphedema in determining the number of positive lymph nodes. The gray line has the largest area under the curve, which means positivity of eight lymph nodes has the higher sensitivity and specificity. n7positive, cutoff point 7 lymph nodes; n8positive, cutoff point 8 lymph nodes; n9positive, cutoff point 9 lymph nodes.
A logistic regression analysis performed to determine the independent factor effective in preoperative lymphedema resulted in an accurate prediction rate of 81.9% for the model; BMI >30 and the number of positive lymph nodes were found as independent factors (Table 3).
OR, odds ratio.
Secondary lymphedema risk was found statistically significantly higher in patients with a BMI of 30 and higher (p < 0.001).
When the patients were divided into two groups according to whether their BMI was equal to 30 and higher and <30, the number of positive lymph nodes and lymphedema were found associated; no statistically significant relationship was found between the number of positive lymph nodes and BMI in patients with a BMI of <30 (p = 0.858, p = 0.013).
Median follow-up period was 36 months (10–52 months), and clinical lymphedema was seen in 23.5% (n = 65) of the patients. Subclinical lymphedema turned to clinical lymphedema in 24 (49%) patients after surgery. Clinical lymphedema risk was found to be statistically significantly higher in patients who have had subclinical lymphedema before surgery (p = 0.000) (Table 4).
There was no statistically significant difference in the lymphedema rates between the <65 and >65 age groups (p = 0.219).
Discussion
Prolongation of survival due to increased rate of early diagnosis and modern treatment methods resulted in raised attention in increasing the quality of life of patients. Therefore, studies have started to focus on oncoplastic breast surgery for a better cosmetic appearance and early diagnosis, and prevention and treatment of lymphedema.24–26
Bioimpedance analysis measures the difference in the amount of extracellular fluid between two extremities and has gradually been increasingly used in the diagnosis of lymphedema.27–29 The superiority of this method over other diagnostic methods is in the possibility of early diagnosis and achievement of quantitative measurement. 18 The rate of lymphedema was found to reach 17.7% using preoperative bioimpedance analysis in patients with no clinical symptoms of lymphedema in the present study. The results of the physical examination and measurement of arm circumference demonstrated no difference between the two extremities, and thus, the results revealed the presence of subclinical lymphedema. Preventive measures, exercise, and treatment may decrease the rate of clinical lymphedema in patients who are diagnosed as having subclinical lymphedema.22,30,31 In a study by Soran et al., the rate of clinical lymphedema was demonstrated to be decreased to 4.4% from 36.4% through early diagnosis and treatment in patients with subclinical lymphedema using bioimpedance. 30 In our previous study, resolution of lymphedema or regression to a milder stage was provided in patients with subclinical lymphedema. 22 In the present study, subclinical lymphedema was diagnosed using bioimpedance analysis in ∼1/5 of the patients who were diagnosed as having early-stage breast cancer despite the absence of clinical lymphedema, and this group has higher clinical lymphedema rates after the surgery. The results reveal that early diagnosis of lymphedema, which significantly worsens the patients' quality of life, is possible with bioimpedance analysis and clinical edema is preventable.
Factors that increase the risk of lymphedema following treatment of breast cancer with a high level of evidence have been reported to be ALND, number of lymph nodes excised from the axilla, mastectomy, and high BMI.1,2,11,32,33 The number of metastatic axillary lymph nodes, radiotherapy, chemotherapy, and not participating in regular physical activity are risk factors with intermediate evidence levels. Blockage of lymph flow at the level of lymph nodes in general and the resulting accumulation of protein-rich lymph fluid in extracellular fluid have been proposed to be the main physiopathologic mechanism of lymphedema. 20
The rate of lymphedema is 8%–28% in patients who undergo ALND, and around 5%–7% in patients who undergo SLNB alone.1,34,35 In the current study, extremity lymphedema was evaluated and the extracellular fluid (lymphedema) in an extremity compared with the contralateral side was found increased in patients with capsular invasion in the lymph node and presence of metastasis in more than eight lymph nodes, and this result supports the theory of the lymph flow blockage in the pathophysiology of lymphedema. Nevertheless, detection of subclinical lymphedema in 20 (13.8%) out of 144 patients with negative axilla among the patients who underwent SLNB alone suggests the possible responsibility of factors in the developmental mechanism other than flow blockage secondary to lymphatic tumor infiltration. Stanton and colleagues demonstrated an increase in lymph flow in the normal arm following treatment of breast cancer. 14 Another study by Bains et al. found that preoperative lymph flow was increased in arms in which lymphedema developed due to the treatment of breast cancer. 15 In a study by Cintolessi et al., preoperative lymphatic pump pressure and rate of transport of radioactive substances were found increased in patients who developed lymphedema secondary to breast cancer compared with patients without lymphedema. 12 In an experimental study by Gousopoulos et al., Ly6G+ and CD4+ lymphocytes were found effective in the development of lymphedema that developed secondary to trauma in lymph vessels. 36 These studies suggest the effects of the structural properties of the lymphatic system and immunologic factors in the development of lymphedema.
Increased BMI has been demonstrated to significantly increase the risk of development of lymphedema among all other factors.1,2,11,34,37–39 In the present study, BMI ≥30 kg/m2 was also found as a major factor that increased the rate of lymphedema. The negative effect of obesity on lymphedema, independent of surgery, has been tried to be explained by a decreased transport capacity of the lymphatic fluid and destruction of the structure of lymph nodes secondary to fatty infiltration.40–42 Among the findings of the current study, the number of positive lymph nodes found to be associated with lymphedema in patients with a BMI higher than 30, along with the absence of a similar relationship in patients with a BMI of <30, suggests that the factors responsible might be damaged lymph flow at the first stage, and subsequently, lymphatic blockage secondary to tumoral infiltration of the lymph nodes.
As mentioned above, ALND has been reported to be one of the most important risk factors for lymphedema in almost all of the studies on lymphedema.1,3–7,9,10 In a meta-analysis, the rate of lymphedema among patients who underwent SLNB and axillary lymph node biopsy was reported as 5.6% and 19.9%, respectively. 1 ALND has morbidities other than lymphedema, such as limited shoulder movements and numbness in the arm.43,44 This high rate of morbidity has resulted in the evaluation of the genetic profile of the tumor instead of ALND, which is beneficial in determining the prognosis of breast cancer, and has been accepted as having an important role in the treatment. 45
The results of some prospective clinical studies have demonstrated that omitting ALND in patients with a positive SLN had no effect on local recurrence and survival rates, and thus surgeons may become content with SLNB alone.9,46,47 In the American College of Surgeons Oncology Group (ACOSOG) Z0011 study, patients who underwent lumpectomy and SLNB and were found to have no more than two positive sentinel lymph nodes were randomly divided into two groups, those who underwent ALND and those who received radiotherapy to the breast. Overall survival, disease-free survival, and local recurrence rates were similar between the groups. The rate of lymphedema was found increased in patients who underwent ALND. 9 In the AMOROS study, patients with cT1-2N0 breast cancer and positive SLN were randomized into two groups, those who underwent ALND and those who received radiotherapy to the axilla. 47 The 5-year recurrence rates were 0.43% and 1.19% in the ALND and axillary radiotherapy groups, respectively (p > 0.05). The rate of lymphedema in the ipsilateral arm was found higher in the group that underwent ALND compared with the radiotherapy group. In addition, a twofold increase in the lymphedema rate was found in patients who received regional nodal irradiation (including internal mammary, supraclavicular, and axillary lymph nodes) in addition to whole-breast irradiation in the MA.20 Clinical Trial. 48 The Axillary Lymphatic Mapping Against Nodal Axillary Clearance (ALMANAC) trial, in which ALND was compared with SLNB in terms of quality of life and arm edema, demonstrated that arm edema, arm numbness, and pain and function loss in the shoulder were seen in increased rates in the ALND group. 46
Axillary lymph node positivity and capsular invasion of lymph nodes were found to be significant risk factors for subclinical lymphedema in patients with breast cancer in our study. Since the pathologic complete response (pCR) rate increased up to 40% in clinical studies with new drugs, NAC has been used more frequently in patients with clinically node-positive breast cancer. 49 This high pCR resulted in a tendency toward SLNB instead of ALND in clinically node-positive patients undergoing NAC. In a new meta-analysis, the pooled estimate for false-negative rate (FNR) was found to be 13%. 50 FNR was also 13.7% in our previous study. 51 Although FNR is higher in patients with locally advanced breast cancer after NAC than those with clinically node-negative early breast cancer patients, an FNR of 13% is very unlikely to adversely affect overall survival. For this reason, the SLNB after NAC in biopsy-proven node-positive patients may be a reasonable alternative management strategy to complete ALND. In biopsy-proven node-positive patients with subclinical lymphedema, NAC may be preferred, and SLNB may replace ALND. This less radical surgical treatment of axilla can decrease the lymphedema rate and increase the quality life of patients with axillary lymph node positivity and capsular invasion of lymph nodes.
In conclusion, it is clear that bioimpedance may provide the diagnosis of subclinical lymphedema and this may be helpful to make a decision for surgical and radiation treatment of the patients. Early treatment of subclinical lymphedema may prevent progression of this complication to clinical lymphedema. ALND may be avoided in patients with lymphedema, even if the axilla is positive. The addition of axillary radiotherapy to SLNB together with systemic therapy may decrease locoregional recurrences and lymphedema risk and also increase the quality of life.
Footnotes
Acknowledgment
The authors thank Mr. David Chapman for his meticulous editing of the manuscript.
Author Disclosure Statement
No competing financial interests exist.