
Abstract
Abstract
Purpose:
We aimed to assess the improvement in stiffness in patients with postmastectomy lymphedema (PMLE) after intermittent pneumatic compression (IPC) using acoustic radiation force impulse (ARFI) imaging and evaluate the effects of different IPC pressures.
Methods:
We randomly assigned 45 patients with PMLE (stage II) to three groups based on the IPC pressure: 25, 35, and 45 mmHg. Patients received a single session of IPC for 30 minutes. We recorded the subcutaneous tissue thickness of the proximal upper limbs using ultrasonography and circumference of the upper limbs and stiffness using ARFI before and immediately after IPC.
Results:
Arm circumference and subcutaneous tissue thickness were significantly decreased after IPC in all groups. The shear wave velocity (SWV) decreased after IPC in all groups, but significantly decreased only in the 35 mmHg group. The subcutaneous tissue thickness and SWV in the 35 mmHg group were significantly decreased compared to the other groups.
Conclusion:
IPC can reduce stiffness and subcutaneous tissue thickness of the proximal upper arm in patients with PMLE. A pressure of 35 mmHg yields the largest improvement of stiffness; higher compression pressure did not yield any additional improvement.
Introduction
L
Breast cancer surgery is recognized as the major cause of upper limb lymphedema. 3 The incidence of breast cancer-related lymphedema is markedly high at 24%–49% after total mastectomy, 3%–15% after sentinel node biopsy, and 2.4%–49% after complete axillary dissection.4–9 The individuals with lymphedema experience significant problems such as impaired extremity function, recurrent episodes of soft tissue inflammation (cellulitis, lymphangitis), lymphorrhea, lymphangiosarcoma, unsatisfactory cosmesis, and various psychological and social issues. 10
At present, therapeutic efforts remain focused on minimizing the edema, reducing its severity and symptoms, impeding progression, mitigating the complications, and reversing and restoring the functional and cosmetic nature of the limb. 10 Among the therapies available for edema reduction, the conservative method of external compression remains the main treatment option. In fact, one of the most promising methods is intermittent pneumatic compression (IPC).
Most patients who visit the lymphedema clinic complain of discomfort caused by arm stiffness. Understanding the mechanical properties of subcutaneous tissue is essential in clinical diagnosis, and research on lymphedema and the application of this knowledge to patient care have first call to early diagnosis and rehabilitation. In addition, this objectification is essential to determine the real effect of treatments and to enable health practitioners and patients to better know what to expect after a treatment. More marked results or prognosis could reasonably be expected following a treatment. Several studies have attempted to mechanically measure the stiffness of living tissue. One method involves the evaluation of stiffness of edematous skin based on the relationship between the displacement of the skin surface and force applied by a contact probe. 11 In addition, Kawahara et al. have suggested the noncontact type stiffness sensor. 12 Another method involves fibrotic induration assessment by tonometry; in this method, the resistance to compression is measured (associated with the extent of fiber buildup) by placing a weight-based tonometer over the midpoint of a lymphatic territory or over a watershed. 13 The reliability of these techniques has been tested and, to some extent. But these methods have some issues that measurement result has been disturbed by a local structure, including blood vessels, muscles, and bones. So multiple measurement around the limb has been required for obtaining whole stiffness of limb. The acoustic radiation force impulse (ARFI) imaging utilizes ultrasound elastography technology. It is an ideal tool to noninvasively and quantitatively estimate the tissue stiffness in the clinical setting. ARFI can be performed by mechanically exciting tissues with a localized impulsive radiation force, which leads to the propagation of a shear wave away from the region of excitation. 14 The shear wave velocity (SWV) is directly correlated with tissue stiffness. In general, a greater SWV is correlated with stiffer tissue. Hence, ARFI imaging has been used to study various tissues, including liver, breast, kidney, spleen, prostate, pancreas, testes, thyroid, and muscle and tendon.15–23 The most notable application of ARFI is the detection of liver fibrosis, as fibrous tissues are usually more stiffer than the surrounding tissues.24–29
In the present study, we aimed to assess the improvement in stiffness of patients with postmastectomy lymphedema (PMLE) immediately after pneumatic compression using ARFI and compare the effects of different pneumatic compression pressures.
Materials and Methods
Subjects
The patients (N = 45) were consecutively selected by a physician from the outpatient clinic of the Department of Rehabilitation Medicine of Chungnam National University Hospital. Breast cancer survivors were considered to have breast cancer-related lymphedema based on the following criteria: difference in circumference of >2 cm between the affected arm and normal arm and a diagnosis of lymphedema made by lymphoscintigraphy (delay or obstruction of lymphatic flow compared with the unaffected side, dermal backflow, poor to no visualization of the collateral and main lymphatics, and decreased or no clearance of radioisotope from the injection site). 24
The inclusion criteria were as follows: patients who have undergone mastectomy for unilateral nonmetastatic breast cancer; PMLE stage 2; and not receiving chemotherapy at the time of recruitment. Moreover, the exclusion criteria were as follows: PMLE stage 0, 1, and 3; patients with lymphedema in both arms; patients with a history of bilateral metastatic breast cancer; need for concurrent anticancer chemotherapy; patients with cancer recurrence within 6 months from the time of study enrollment; patients with vascular disease; patients with any neurologic signs, such as decreased motor power, sensory changes, or decreased deep tendon reflexes; and patients who could not communicate.
The study was approved by the ethics committee of our hospital, and informed consent was obtained from each subject. A total of 45 patients were randomly assigned to three groups based on the compression pressure used: Group A, 25 mmHg; Group B, 35 mmHg; and Group C, 45 mmHg.
Baseline data
Demographic information, including age, gender, body mass index (BMI), and affected site, was collected at baseline. The data concerning medical history included time since surgery, chemotherapy, radiation, and number of nodes removed, if applicable. Table 1 summarizes these data for all the subjects according to the groups assigned.
BMI, body mass index.
Compression therapy system
IPC was applied using Lympha Press® Plus (1033-EL; Mego Afek, Israel) along with a 10-chamber sleeve used for applying the Lympha mode. The system delivered a sequential pressure along the limb, from the distal to the proximal end, without any deflation of the distal chambers to prevent backflow fluid and venous stasis. The overall pressure duration was 30 minutes, with alternate periods of inflation (18 seconds) and deflation (4 seconds) (Fig. 1).

ARFI imaging. The ROI located within the subcutaneous tissue. The mean shear wave velocity in the ROI is 2.44 m/s in the
The subjects were comfortably placed in the supine position, while the compression sleeve was pulled up to the axilla. The elbow within the sleeve was positioned at an angle that was comfortable for each subject. To determine the effect of the compression, we measured arm girth, subcutaneous depth, and stiffness before and immediately after IPC.
Arm girth measurements
Girth (circumference) measurements were performed with a nonelastic tape measure. Each subject was seated with their arms extended and palms resting on their ipsilateral knee. The girths were measured at 10 cm proximal to the antecubital fold midpoint. Girth measurements were obtained primarily by two individuals, including a rehabilitation medicine physician and an experienced lymphedema therapist who routinely performs such measurements in active lymphedema practice.
Ultrasonographic measurements
ARFI imaging
A single rehabilitation medicine physician conducted ARFI imaging for all subjects. An ultrasound system (ACUSON S2000, S2000; Siemens Healthcare, Erlangen, Germany) with a 9L4 linear array transducer was used for this study. Prototype ARFI imaging technology has been united into the commercial system in the form of Virtual Touch IQ™ software; this software provides a quantitative assessment of tissue stiffness through SWV measurements.
The subjects were placed in a supine position with their arm in full extension. The transducer was placed in a transverse position at 10 cm proximal to the midpoint of the antecubital fold. During the examination, a visible ultrasound gel layer with a thickness of 2–7 mm was maintained between the transducer and the skin on the ultrasound monitor. The presence of a gel layer resulted in minimal compression from the transducer to the skin and the underlying tissues. During the examination, three trials of ARFI imaging were performed using the Virtual Touch IQ™ software. Each region of interest (ROI) box had a preset size of 5 × 5 mm. The SWV measurements corresponding to these ROI boxes were shown to the right of the ultrasound image (Fig. 2). Three ROI boxes were randomly placed along the subcutaneous tissue, which do not overlap without changing the location of the transducer.

Compression therapy system.
Subcutaneous thickness
A conventional B-mode gray-scale image was obtained at the level of the same point for the measurement of ARFI. The thickness of the subcutaneous tissue was defined as the distance from the skin to the fascia. Accordingly, subcutaneous depth and SWV were measured thrice each by a rehabilitation medicine physician.
Statistical analyses
Statistical analyses were performed using SPSS Version 22.0 for Windows (SPSS, Inc., Chicago, IL). All values were averaged and presented with standard deviation. Statistical significance of the differences before and after treatment was analyzed by the paired t-test. The three treatment groups were compared using the nonparametric Kruskal–Wallis test and post hoc analysis of Pairwise comparison. A p-value of <0.05 was considered statistically significant.
Results
The arm circumference, subcutaneous depth, and SWV values are presented as mean ± standard deviation and are summarized in Table 2.
Reduction of arm girth (circumference)
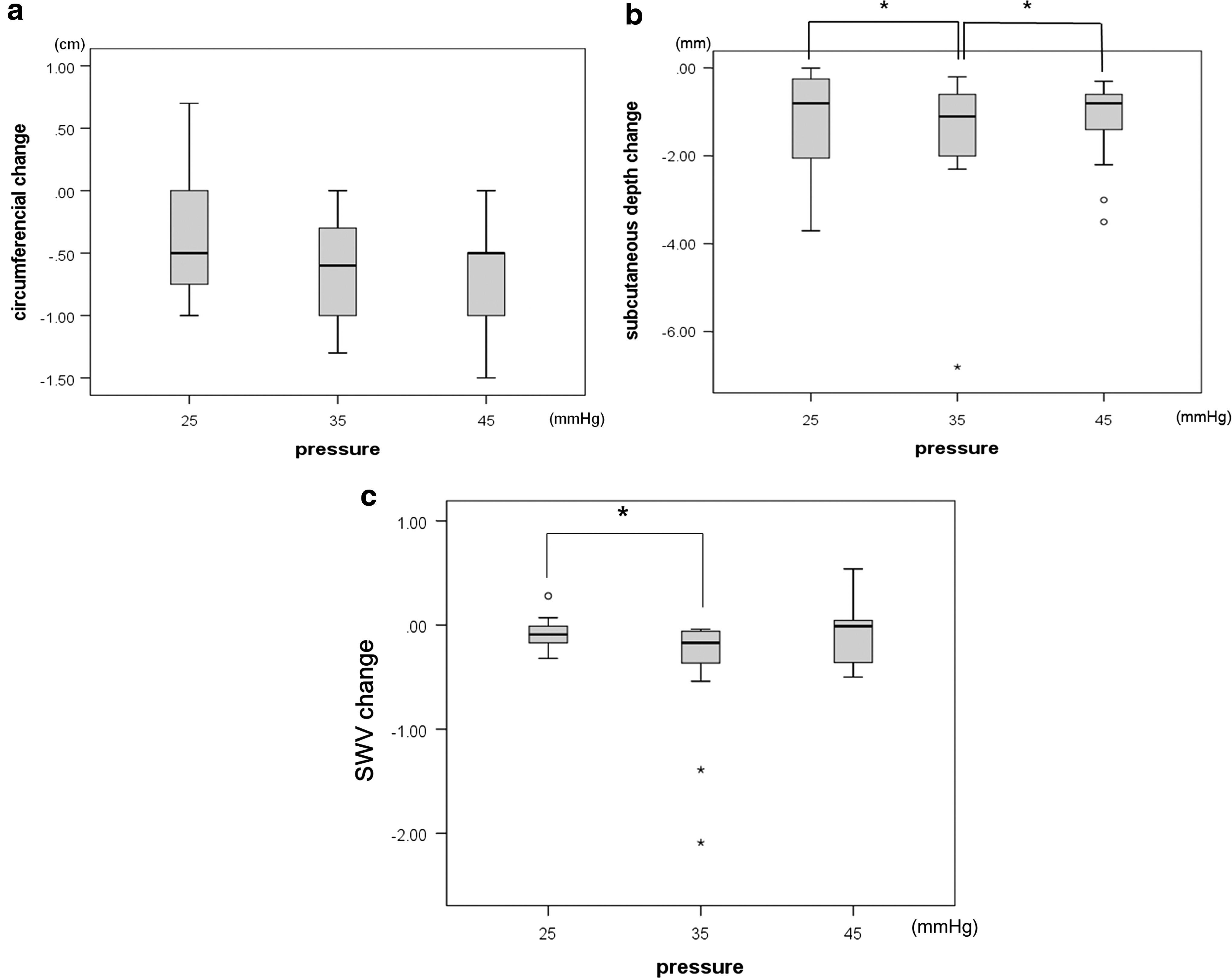
Compared with the baseline values, all three groups showed a significant reduction of arm circumference, with mean reductions of 0.40, 0.63, and 0.67 cm in the 25, 35, and 45 mmHg compression groups, respectively (Fig. 3a).
Changes of
Ultrasonographic measurements
Subcutaneous thickness
Ultrasonographic measurement of the subcutaneous tissue in all three groups indicated a significant decrease immediately after intervention. The mean reduction in subcutaneous thickness was 1.16, 2.07, and 1.20 mm in the 25, 35, and 45 mmHg compression groups, respectively. However, the subcutaneous thickness was significantly different in the 35 mmHg compression group compared to the other groups (p = 0.014) (Fig. 3b).
Shear wave velocity
The SWV was significantly decreased only in the 35 mmHg compression group, with a mean value of 0.40 m/s. The SWV showed a decreasing tendency before and after intervention, although no significant difference was observed in the 25 and 45 mmHg compression groups with mean values of 0.08 and 0.05, respectively. The SWV was significantly decreased in the 35 mmHg group compared to the other groups (p = 0.034) (Fig. 3c).
Correlation of ultrasonographic measurements and clinical values
The reduction of SWV showed a significant positive correlation with subcutaneous depth, with a correlation coefficient of 0.63 (p = 0.00). However, the reduction of arm circumference was not correlated with subcutaneous depth (correlation coefficient, 0.20 [p = 0.18]) or with the SWV (correlation coefficient, 0.16 [p = 0.28]).
Correlation of BMI and measurements
The change showed significant positive correlation of BMI with subcutaneous tissue depth decrease with a correlation coefficient of 0.56 (p = 0.04). The BMI with arm circumference and with SWV change showed no significant correlation.
Discussion
In the present study, we aimed to investigate the improvement of arm stiffness in patients with PMLE after breast cancer surgery and to determine an appropriate pressure for IPC. With regard to the indices for clinical assessment, we measured upper limb circumference on the affected side, as well as subcutaneous tissue thickness and SWV using ARFI imaging.
There are several mechanisms proposed for the development of lymphedema after breast cancer surgery. It can develop as a result of reduced lymph circulation following lymphadenectomy and can also be affected by venous obstruction, axillary vein varicosities, thrombophlebitis, or fibrosis. 30 The condition can be aggravated by additional treatment, such as radiotherapy. 4 The vasospasm of smooth muscle in the blood or lymph vessels is another factor that can contribute to lymphedema. Compared to edema that develops in venous disease, lymphedema is characterized by the deposition of protein-rich fluid, and high-molecular weight proteins cannot cross the capillary walls. This leads to a relative imbalance in hydrostatic and colloid osmotic pressure and can result in increased capillary permeability, followed by the accumulation of interstitial fluid. One method to control edema is to facilitate the entry of extracellular fluid accumulated in the tissues within the circulatory system.
In lymphedema the tissue stiffness depends on the solid structure (mass of collagen, its stereostructure, mass of fibroblasts, and adipocytes) and mobile tissue fluid in the matrix. Fluid accumulation in tissue and recoil force of solid structure generate increased pressure like wet sponge. 31 IPC is a recognized therapeutic procedure for lymphedema through wet and dry sponge phenomenon. In this procedure, the periodic compression exerted on the tissues at the affected extremity facilitates mobile tissue fluid to the lymph vessel and the flow of lymph to the collecting lymphatic vessels; this leads to filling of the vessels when the compression is released. The rhythmic periodicity of compression facilitates the outflow of venous blood, without affecting the inflow of arterial blood to tissues.32–35 There might be no evident change in circumference but change to fluid volume.
Immediately after a single session of pneumatic compression, we observed a decrease in upper limb circumference and subcutaneous tissue thickness on the affected side. Moreover, we observed a significant change in upper limb tissue stiffness caused by lymphedema. In addition, among different pneumatic compression pressures, we observed that a pressure of 35 mmHg led to significant improvements in subcutaneous tissue thickness and stiffness; a higher compression pressure did not yield any additional improvement. Thus, the present study indicated interesting results concerning the extent of improvement in edema and stiffness achieved by different compression pressures. Although, it was suspected that pneumatic compression exerting higher pressures could lead to more pronounced reduction of edema and stiffness, we observed that the improvements were enhanced with an increase in pressure from 25 to 35 mmHg, although no further reduction was observed after increasing the pressure to 45 mmHg. Damstra et al. compared the use of low pressure (20–30 mmHg) with high pressure (44–68 mmHg) compression bandages and found that lower pressure (20–30 mmHg) compression bandages achieved the higher volume reduction than higher pressure (44–68 mmHg) compression bandages. 36 In addition, in the study of Mosti et al., the optimal pressure range concerning leg edema reduction was found between 40 and 60 mmHg, while the higher pressures produced by bandage showed a negative correlation with volume reduction. 37 Recommendations for an optimal pressure range in managing edema of the extremities by compression are still not set. Not only the timing and the pattern but also the magnitude of the optimal pressures in different devices is still discussed.
The two main mechanisms by which compression reduces edema involve the reduction of fluid filtration at the capillaries and the enhancement of lymphatic drainage. However, external pressures exceeding the venular pressure could be counterproductive, as they may have a negative effect on lymphatic transport. This theory can be explained based on the study of Modi et al. 38 The authors observed that patients with postmastectomy arm lymphedema exhibit contractile impairment of lymph collection; hence, external compression exceeding this lymphatic pump pressure could be a hindrance to the lymphatic drainage or would damage the prefascial lymphatics, causing dysfunction of endothelial flap. In the present study, we appeared to have determined the “optimal pneumatic compression pressure” in terms of edema reduction. Moreover, a further reduction of heterogeneous interstitial fluid (not pure water) would lead to a reduction in tissue stiffness.
Nevertheless, the mechanism of optimal pressure in the study can be explained by high skin compliance in the stage II of edema patient, allowing its stretching of the subcutaneous space accumulating excess of capillary filtrate and the pressure smoothly transmitting. In more progressed lymphedema, high compression pressure and as much time would be needed for the efficacy. 39 The differences have been rather small to discuss the effectiveness of the IPC. In addition, the differences have been rather small to discuss the effectiveness of the IPC. The difference would have been somewhat greater if we had a more repetitive treatment and as much compression time. So, long-term study with subjects divided by lymphedema severity would be needed.
The most interesting result of the present study was the positive correlation between the reduction of subcutaneous thickness and SWV using ARFI. This finding reflected the positive effect of immediate IPC on reducing both tissue thickness and stiffness. Regarding the correlation with BMI, the change showed significant positive correlation of BMI with subcutaneous tissue depth decrease. The higher BMI represented the higher value of reduction of subcutaneous tissue thickness. The impact of pneumatic compression on reduction of subcutaneous tissue depth is supposed to be maximized in the higher BMI person who has high percentage of body fat. The BMI and arm circumference change showed no significant correlation. It is assumed that there were some issues that circumference measurements have been affected by local structures, including blood vessels, muscles, and bone not only by subcutaneous tissue.
Several tools are available for evaluating stiffness in the clinical setting. In the present study, we used ARFI elastometry, which is a recently developed ultrasonography (US)-based modality, to objectively quantify tissue elasticity. ARFI—a promising elastography technique—can provide information on the elastic properties of the tissues in an efficient and convenient manner, which can complement US examination. We used the virtual touch tissue quantification response to measure the stiffness of subcutaneous tissue. Depending on the interactions between the waves and the transducer, a stiffer tissue has been found to exhibit a greater SWV. 40 In particular, the SWV is proportional to the square root of the tissue elasticity; hence, the quantitative implementation of ARFI can generate objective and reproducible data.14,41 To our knowledge, this is the first study to quantify the stiffness of tissue to evaluate lymphedema.
We investigated the changes in tissue thickness using US as an indicator to assess clinical improvement; however, the values for thickness obtained using US can differ according to the examiner. Nevertheless, US is known to have outstanding reliability when evaluating subcutaneous tissue elasticity in lymphedema. 42 Moreover, it has been reported to have excellent reliability when measuring soft tissue thickness in the forearm. 43 Although it is possible to assess actual clinical improvement based on the decrease in circumference and thickness, our study results indicate that changes in the arm circumference and tissue thickness measured by US may not always be consistent. Hence, the changes in elasticity and changes in edema volume may not always be consistent and are in fact mutually independent assessment methods.
Despite the effect of immediate IPC on lymphedema reduction and our results regarding optimal compression pressure, we believe that the findings need to be confirmed by a large sample, multicenter randomized controlled trial. Moreover, we only assessed the immediate effect of a single IPC session in the present study. Future studies should investigate the long-term effect of multiple IPC sessions to clarify the optimal compression pressure to reduce lymphedema.
Conclusion
The stiffness measured by ARFI and thickness of the subcutaneous tissue reduced immediately after IPC in patients with PMLE. A compression pressure of 45 mmHg does not lead to an increased extent of edema and stiffness reduction. In fact, a pressure of 35 mmHg was most effective for edema reduction. Nevertheless, systematic research based on a large number of participants is essential to further clarify the possible effects of pneumatic compression in the treatment of lymphedema.
Footnotes
Author Disclosure Statement
No competing financial interests exist.