
Abstract
Abstract
Purpose:
Lymphedema can have a negative impact on the function and quality of life (QOL) of patients, but most studies have examined lymphedema as a binary variable, rather than a multidimensional disease that ranges in severity. This study explored the potential impact of lymphedema severity on function and overall QOL.
Methods and Results:
Of the 54 lymphedema patients recruited, 40 reported their most severe swelling to be in a limb. These participants underwent bioimpedance measurement (L-Dex®) and completed either the disabilities of the arm, shoulder, and hand (DASH) questionnaire or the lower extremity functional scale (LEFS). All participants completed the lymphedema quality of life questionnaire (LYMQOL) and were categorized for severity using International Society of Lymphology (ISL) stage. Mild (Stage 0-I), moderate (Stage IIa), and severe (Stage IIb-III) lymphedema accounted for 22%, 50%, and 28% of the participants, respectively. The median [inter-quartile range (IQR)] L-Dex score was 17.8 (6.6–52.7) for arm participants and 36.4 (15.9–93.5) for leg participants. Apart from a mild difference in LYMQOL ARM Appearance domain (p = 0.046), ISL staging did not have any relationship with DASH, LEFS, and LYMQOL domains, or overall QOL. Higher L-Dex was related to poorer function (DASH p = 0.015; LEFS p = 0.019), but was not related to overall QOL of limb lymphedema participants (p > 0.05).
Conclusions:
Lymphedema severity did not appear to impact QOL. ISL staging may not be used alone to describe lymphedema severity. Other methods such as bioimpedance, imaging, and self-report of symptoms are required to fully evaluate the impact of lymphedema severity on function and QOL.
Introduction
L
There have been a number of studies examining the relationship between lymphedema, physical function, and quality of life (QOL). Breast cancer-related upper limb lymphedema features heavily in these studies, with most reporting the presence of lymphedema to have a negative impact upon patients' function and QOL.4–10 Other studies have also reported a poorer function and QOL in patients with lymphedema secondary to other tumors such as head and neck, 11 and gynecological cancers. 12 Typically, lymphedema in the arm can affect glenohumeral joint function, with an increased weight and traction on the rotator cuff tendons, and disruption in scapulohumeral rhythm. 13 Lymphedema in the leg can alter gait and mobility. 14 Head and neck lymphedema may be serious enough to disrupt speech, swallowing, and sleep.15,16 The negative impact on function has been associated with the deterioration of QOL in lymphedema patients.9,11
For many of the above studies, the objective severity of the patients' lymphedema is unknown.6,13,14 Despite some studies measuring lymphedema signs using circumferences or volumes of limbs, analyses of QOL have typically examined lymphedema as a binary variable, using different cutoff points for definition of lymphedema and simply recording its presence or absence.6,8,14 This is not helpful for many lymphedema patients who suffer from mild lymphedema, who may be below the thresholds for some definitions of lymphedema. 17 It is also unhelpful for patients with severe lymphedema to be grouped with patients who have mild lymphedema as prognosis of function and QOL may vary significantly depending on lymphedema severity.
Lymphedema is also a multidimensional disease and its signs are not restricted to circumferential or volumetric increases in limb size. The tonicity or firmness of the swelling may impact the ability to move body parts or it may affect levels of pain and discomfort. 17 The absence or presence of lymphorrhea and skin-related changes may also have a direct impact on the frequency of skin infections, the associated need for antibiotic use, and wound management. 18 It is possible to have these changes in the swollen limb without circumferential change. A measurement scale that categorizes lymphedema severity based on these lymphedema signs is the International Society of Lymphology (ISL) staging system that is commonly used by medical doctors and lymphedema therapists. 3
This study primarily aims to explore the potential impact of lymphedema severity, based on measurable signs identified by the ISL stage, on overall QOL. In addition, bioimpedance, which detects a change in extracellular fluid using L-Dex®, will be examined for its relationship with function and QOL. Finally, functional questionnaires for limb lymphedema will be examined for its relationship with QOL in lymphedema patients.
Materials and Methods
Participants were recruited from lymphedema clinics in two cancer treatment cancers, Royal North Shore Hospital and Melanoma Institute Australia, in Sydney, Australia. Eligible patients identified from the clinic database were posted a letter of invitation and a Participant Information Sheet. Expressions of interest were followed up with a phone call from one of the investigating health professionals to confirm eligibility and organize a suitable time to attend the clinic to give written consent, complete the questionnaires, and for clinical examination.
Eligible patients had to be over 18 years of age and identify themselves to have lymphedema, and be able to read and communicate in English for the completion of the required questionnaires. They could have secondary lymphedema from any cancer, in any area of their body. Limb lymphedema was to be unilateral as an unaffected side was required for bioimpedance measurement. Human ethics approval was gained through the institutions' ethics committee in accordance with the Helsinki Declaration. 19 Both male and female patients were invited to participate.
Participants were seen by two qualified lymphedema physiotherapists, accredited by the Australasian Lymphology Association's National Lymphedema Practitioners' Register. Physiotherapists examined the participant's area of “most swelling,” and staged the severity of their lymphedema using the ISL staging (Table 1). Bioimpedance measurement was also performed using either ImpediMed U400 or XCA machines (ImpediMed Ltd, Brisbane, Australia). These machines measure extracellular fluid impedance by passing a small electrical current through adhesive skin electrodes following a standardized measurement protocol.20–23 A Lymphedema Index, or what it known as L-Dex, was calculated by the machine, which is reflective of the impedance ratio between affected and unaffected limbs. Previous research has shown that the results from the XCA or U400 devices are comparable. 24
ISL, International Society of Lymphology.
Participants with limb lymphedema also completed a physical function questionnaire; disabilities of the arm, shoulder, and hand (DASH) 25 or lower extremity functional scale (LEFS), 26 and all participants completed the lymphedema quality of life questionnaire (LYMQOL). 27 The DASH and LEFS were chosen because they have been previously validated for the assessment of upper 28 and lower limb function, 26 respectively, and the LYMQOL questionnaire has been validated as a QOL assessment tool for use in the lymphedema cohort. 27 All questionnaires were scored according to their respective, recommended scoring guide.25–27
Data analysis
Statistical analysis was performed using IBM® SPSS® Version 23. Kruskal-Wallis tests were used to evaluate the relationship between lymphedema severity, function, and QOL. Linear regressions were used to determine the relationship between L-Dex and function and QOL. Similarly, linear regressions were used to determine the relationship between functional questionnaires and QOL. Significance was set at p < 0.05.
Results
Fifty-four patients were recruited, but only participants with arm or leg lymphedema (n = 40) were included for analysis of DASH and LEFS, because these questionnaires are not validated for use in patients with head, neck, or chest lymphedema. Some participants had lymphedema affecting more than one body part; however, data presented in this study is of the body area with the most swelling on the day of clinical examination. Our sample was overwhelmingly female (female n = 46, male n = 8). Median (IQR) QOL score for all participants was 7 (5.50–8.50) and no differences could be found in the QOL scores when separated by the area of lymphedema, sex, age, and time since surgery (Table 2).
p < 0.05.
IQR, inter-quartile range; QOL, quality of life; SD, standard deviation.
ISL stage 0 and I were combined for analyses because the participants (n = 12) in these groups would have “mild” lymphedema that responds to elevation. Stage IIa remained as a single category for analyses because participants (n = 27) in this stage would have “moderate” lymphedema with significant pitting. Stage IIb and III were combined because the participants (n = 15) in these groups would have “severe” lymphedema where pitting is minimal or absent.
The majority of participants had moderate or Stage IIa lymphedema (Fig. 1). The Median (IQR) L-Dex score was 17.8 (6.6–52.7) for participants with arm lymphedema and 36.4 (15.9–93.5) for participants with leg lymphedema.
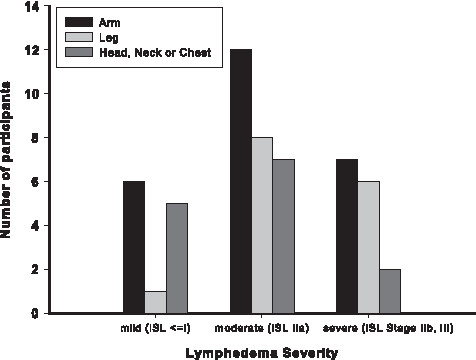
Lymphedema severity of participants.
Relationship of ISL stage to function and QOL
No differences were found between lymphedema severity groups for overall QOL in arm, leg, and head/neck/chest lymphedema participants (Table 3). There was only one patient with mild lymphedema in the leg; hence Kruskal-Wallis tests were performed only for moderate and severe leg lymphedema groups. Lymphedema severity groups did not have any relationship with LEFS, DASH, LYMQOL ARM, or LYMQOL LEG function, symptoms, mood, or overall QOL. LYMQOL ARM appearance differed between severe lymphedema and mild/moderate lymphedema groups, with the more severe group indicating greater concerns with appearance. There was no suggestion of differences between severity groups for LYMQOL LEG appearance.
p < 0.05.
DASH, disabilities of the arm, shoulder, and hand; LEFS, lower extremity functional scale; LYMQOL, lymphedema quality of life questionnaire.
Relationship of L-Dex to function and QOL
For every one point increase in L-Dex, there was a 30% increase in the DASH score (p = 0.015) (Table 4), corresponding with an increased arm and shoulder disability. L-Dex was not significantly related to any of the domains on LYMQOL arm, including QOL.
p < 0.05.
L-Dex was significantly related to LEFS. For every point increase in L-Dex, there was a 32% reduction in LEFS, corresponding with a reduced lower extremity function. For every point increase in LEFS, there was around 10% increase in LYMQOL leg function, appearance, and mood score. L-Dex was not related to LYMQOL leg symptoms and overall QOL (Table 4).
Relationships between functional questionnaires and QOL
Higher disability on the DASH corresponded with lower overall QOL, B = −0.07 (95% CI: −0.12 to −0.02), p = 0.014 (Fig. 2A). Higher function on the LEFS corresponded with higher overall QOL, B = 0.08, (95% CI: 0.04–0.12), p = 0.002 (Fig. 2B).
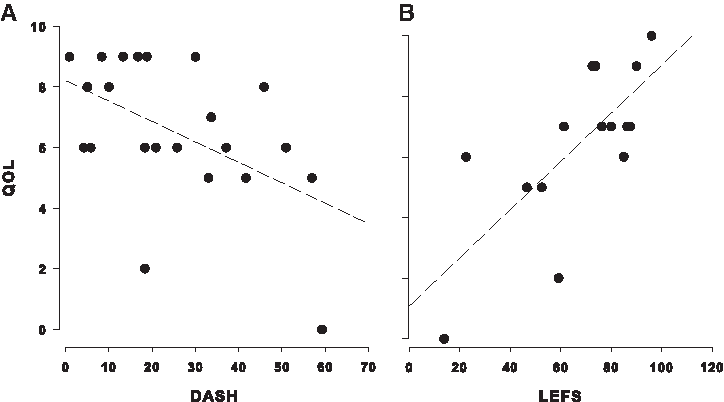
Relationships between functional questionnaires and QOL. Panel A—DASH and QOL; Panel B—LEFS and QOL. QOL, quality of life.
Discussion
Severity of lymphedema did not appear to have a significant relationship with QOL in this study. Participants with moderate and severe lymphedema appeared to retain a high QOL, comparable to that of a participant with mild lymphedema. Neither lymphedema severity based on ISL staging nor L-Dex score was related to overall QOL in arm or leg lymphedema participants. DASH and LEFS were found to be related to QOL in our lymphedema participants, consistent with previous studies. 29
It is possible that ISL categories were not sensitive enough to detect changes in participants' functions and QOL. ISL categories overlap and are not entirely distinct. For example, patients can have a lymphedematous limb that pits (Stage IIa) and also have fatty fibrosis and skin changes present on the same limb (Stage III). It is also acknowledged that patients may have acute on chronic lymphedema, whereby pitting edema exists on top of tissue that has previously undergone a fibrotic change. Patients may also have parts of their lymphedematous limb responding to elevation and other parts of the same limb that do not respond. The overlapping nature of lymphedema signs makes it a challenging disease to classify and these signs may need to be examined individually, irrespective of ISL staging, to truly identify the dimensions that may or may not impact function or QOL. The ISL did suggest, in 2003, a more detailed and inclusive classification should be formulated to include underlying pathophysiologic imaging and testing, 30 but this appears to be still lacking more than a decade down the track. Correlation of ISL staging to existing dermal backflow scales, derived from lymphedema imaging, may improve accuracy in the future.31,32
L-Dex is a measure of extracellular fluid impedance, which works best in detecting early changes in lymphedema, whereas ISL staging is based on the signs of lymphedema and its changes from nonpitting early lymphedema, to pitting lymphedema, and to nonpitting fatty fibrosis. Our results demonstrate that L-Dex is significantly related to DASH and LEFS. This may indicate that it is the actual accumulation of extracellular fluid and possibly the corresponding stretch on the tissue mechanoreceptors that is impacting symptoms, function, and disability, as opposed to the differences that may occur in the physiological tissue change from pitting edema to fatty fibrosis. It is known that tissue mechanoreceptors in the interstitium can also act as nociceptors, thereby, its excitability may result in a greater sensation of pain and discomfort for some lymphedema patients. 33 In contrast, it is possible that patients with chronic lymphedema who have a soft, fatty limb have less stretch on their interstitial tissue mechanoreceptors and thereby less symptomatic pain and discomfort impacting on their function and QOL.
Reduction in function of the lymphedematous arm was related to a reduction in overall QOL of the lymphedema sufferer. In this study, we did not have sufficient numbers to be able to further analyze the data based on arm dominance, but it is probable that an affected dominant arm has a greater impact on function and QOL compared to an affected nondominant arm.34,35 An affected dominant arm would impact on both bilateral and unilateral activities of daily living involving the upper limbs. In addition, patients' arm use related to their employment may affect overall QOL. 36 For example, a house painter with an affected dominant arm may have reduced function with a greater bearing on their employment and QOL compared to a sedentary office worker with an affected dominant arm.
Better lower limb function was related to higher overall QOL in leg lymphedema participants. Gait and mobility dictate independence, and independence is known to directly impact QOL. 37 This is consistent with studies examining patients after hip and knee replacements and corresponding improvements in function and QOL after joint replacement surgery.38,39
The unexpected minimal impact of lymphedema on QOL is consistent with several other studies.35,40–43 Degnim 44 found that patients with symptomatic breast lymphedema to have surprisingly low levels of distress. This may be explained by the fact that lymphedema is a chronic health problem, similar to that of diabetes or osteoarthritis. Patients adapt to the problem and learn to live with their chronic health disability. Patient's personality and their social and coping skills are also important factors to consider when evaluating QOL.35,45 Some patients may not be well equipped psychologically to cope even with mild forms of lymphedema, while others with moderate and severe lymphedema cope remarkably well with increased resilience following survival of cancer. 46 The presence or absence of support at home may also play a crucial role in the way a patient perceives their QOL. Normal activities of daily living such as dressing, cooking, and housework can highlight functional deficits and add frustration to their condition if there is no care giver or significant others available to share or help with some of these tasks.
Future studies may need to look at the time since diagnosis of lymphedema, as time since surgery does not necessarily relate to the time of onset of lymphedema, which may occur years after cancer treatment.47,48 It is possible that patients who develop lymphedema years after cancer treatment are more traumatized by the late onset of this chronic disease, having assumed that their risk reduces with length of time since their cancer treatment. Time since commencement of lymphedema management may also help our understanding of whether appropriate management alters the function and QOL of lymphedema patients.
Limitation of study
It is acknowledged that this study had a small sample size and its results cannot be extrapolated to all lymphedema patients. Future studies should include arm dominance, employment status, occupation, and time since onset of lymphedema in their evaluation of lymphedema. In addition, for true identification of lymphedema signs, imaging such as lymphoscintigraphy, lymphography, or magnetic resonance imaging may be required.
It is also important to consider that our participants in this study were under the care of a lymphedema clinic. They had all been assessed by lymphedema physiotherapists; some participants were undergoing treatment and others have undergone lymphedema treatment recently. The QOL of patients with lymphedema who have not received management under a lymphedema clinic may be different. They may have poorer outcomes with reduced function and QOL, as it is clear that unmanaged lymphedema leads to higher risk of cellulitis and hospital admissions. 49 Furthermore, appropriate management of lymphedema may give patients tools for self-efficacy, resulting in higher perceived coping skills and better QOL for the lymphedema patients. 50
Conclusions
Lymphedema participants in this study generally reported a high QOL irrespective of the severity of their lymphedema. Bioimpedance measurement was superior to ISL staging when establishing the relationship between increased lymphedema severity and poorer limb function. There may be other factors such as employment and limb dominance that further influence the impact that lymphedema severity has on function and QOL. It is also possible that ISL staging alone is not sensitive enough to describe lymphedema severity. To increase its sensitivity, ISL staging may be used in conjunction with other methods such as bioimpedance, imaging, and self-report of symptoms to fully evaluate the impact of lymphedema severity on function and QOL.
Footnotes
Acknowledgments
The authors gratefully acknowledge the patients from Royal North Shore Hospital and Melanoma Institute Australia who participated in this study.
Author Disclosure Statement
No competing financial interests exist.