
Abstract
Abstract
Background:
We evaluated a modified L-Dex score by using the right arm as a reference (LDS rarm ), to determine whether it could be used for the assessment of leg edema in place of the usual L-Dex score calculated by using the contralateral normal leg as a reference (LDS cont ).
Methods:
Bioimpedance analysis was performed in the legs and right arms of 38 patients with unilateral leg edema and in 42 healthy volunteers by using a standard equipotential electrode arrangement.
Results:
The impedance ratio in the right arms of patients (2.6 ± 0.4) was lower than that in their contralateral normal legs (3.0 ± 0.8, p < 0.05), but it was similar to that in the legs (right: 2.4 ± 0.7, left 2.5 ± 0.8) of normal subjects. There was a significant correlation between LDS cont and LDS rarm in legs with edema (right: r = 0.80, left: r = 0.93). No such correlation was found in the legs of normal subjects, but the mean ± 2 standard deviation of their LDS rarm ranged from −3 to 37, which was similar to LDS rarm values in legs with edema corresponding to the normal range of LDS cont (−10 to 10), that is, from 1 to 34.
Conclusions:
LDS rarm could be used as an alternative for LDS cont in the assessment of leg edema.
Introduction
B
Patients and Methods
This study was approved by the Institutional Review Board of Yamaguchi University Hospital (Ube, Yamaguchi, Japan). All participants provided signed, informed consent before enrollment. The subjects included in the current study were 38 patients with unilateral leg edema who attended our clinic between April and September 2015, and 42 healthy volunteers. Subject characteristics are summarized in Table 1.
BMI, body mass index; NS, not significant.
A bioimpedance spectrometer (U-400; Impedimed Ltd., Brisbane, Australia) was employed to determine impedance. The details of measurement were as described in a previous report. 10 First, the impedance in an edematous leg (the right leg in normal subjects) was normalized to the contralateral normal leg (the left leg in normal subjects), and used to obtain the ratio of ECF resistance (Re), which is equal to R0 described in introduction, to intracellular fluid resistance (Ri), that is., Ri/Recont and LDS cont by using a standard equipotential electrode arrangement. Next, the impedance in a leg with edema (the right leg in normal subjects) was normalized to the right arm, and Ri/Rerarm and LDS rarm were obtained.
In patients with leg edema, extremity volume was calculated from tape measurements at 10-cm intervals from the groin to the ankle, as described by Casley-Smith. 11
Statistical analysis
The results are expressed as mean ± SD or count, unless otherwise indicated. The Mann–Whitney U test was used to compare subject characteristics based on BIS and leg volume measurements. Simple linear regression analysis was used to study the correlation between LDS rarm and LDS rarm , LDS rarm in the right and left normal legs, LDS cont and Ri/Recont, LDS cont and leg volume, LDS cont and the ratio of Ri/Recont or leg volume of the legs, LDS rarm and Ri/Rerarm, LDS rarm and leg volume, and LDS rarm and the ratio of Ri/Rerarm of the legs. Statistical analyses were performed by using JMP 11.0 (SAS Institute, Cary, NC). A p < 0.05 was considered significant.
Results
The results of bioimpedance and leg volume measurements are summarized in Table 2. In normal subjects, Ri/Recont and Ri/Rerarm were similar in both legs. These values were also similar to Ri/Re in the right arm. In patients with unilateral leg edema, Ri/Recont and Ri/Rerarm were not significantly different between both legs. However, Ri/Re in the right arm was significantly lower than Ri/Recont and Ri/Rerarm in the legs (p < 0.05 each), and it was similar to the value in normal subjects. In contrast to Ri/Rerarm, mean LDS rarm was significantly different between the leg with edema and the contralateral normal leg.
Versus contralateral normal leg.
Versus normal right leg.
LDS cont , L-Dex score calculated by using the contralateral leg as a reference; LDS rarm , L-Dex score calculated by using the right arm as a reference; Ri, intracellular fluid resistance; Re, extracellular fluid resistance; Ri/Recont, Ri/Re measured by using the contralateral leg as a reference; Ri/Rerarm, Ri/Re measured by using the right arm as a reference.
The correlation between LDS cont and LDS rarm for each leg is shown in Figure 1. In a right leg with edema, LDS cont and LDS rarm showed a good linear correlation (r = 0.80). Values of LDS rarm for these legs corresponding to −10 and 10 for LDS cont , that is, a normal range, calculated from the regression line were ∼1 and 31. LDS cont and LDS rarm for the left leg similarly showed a good correlation (r = 0.93). The values of LDS rarm for the left leg corresponding to a normal range for LDS cont were ∼9 and 34. In the normal right leg, no significant correlation was found between LDS rarm and LDS cont . LDS rarm for these legs ranged from −3 to 36, and mean ± 2 SD was 17 ± 20 (i.e., −3 to 37). LDS rarm for the normal left leg was almost the same as that for the normal right leg (Fig. 2).

Correlation between LDS cont and LDS rarm in legs with edema and right legs in normal subjects. LDS cont , L-Dex score calculated by using the contralateral leg as a reference; LDS rarm , L-Dex score calculated by using the right arm as a reference.
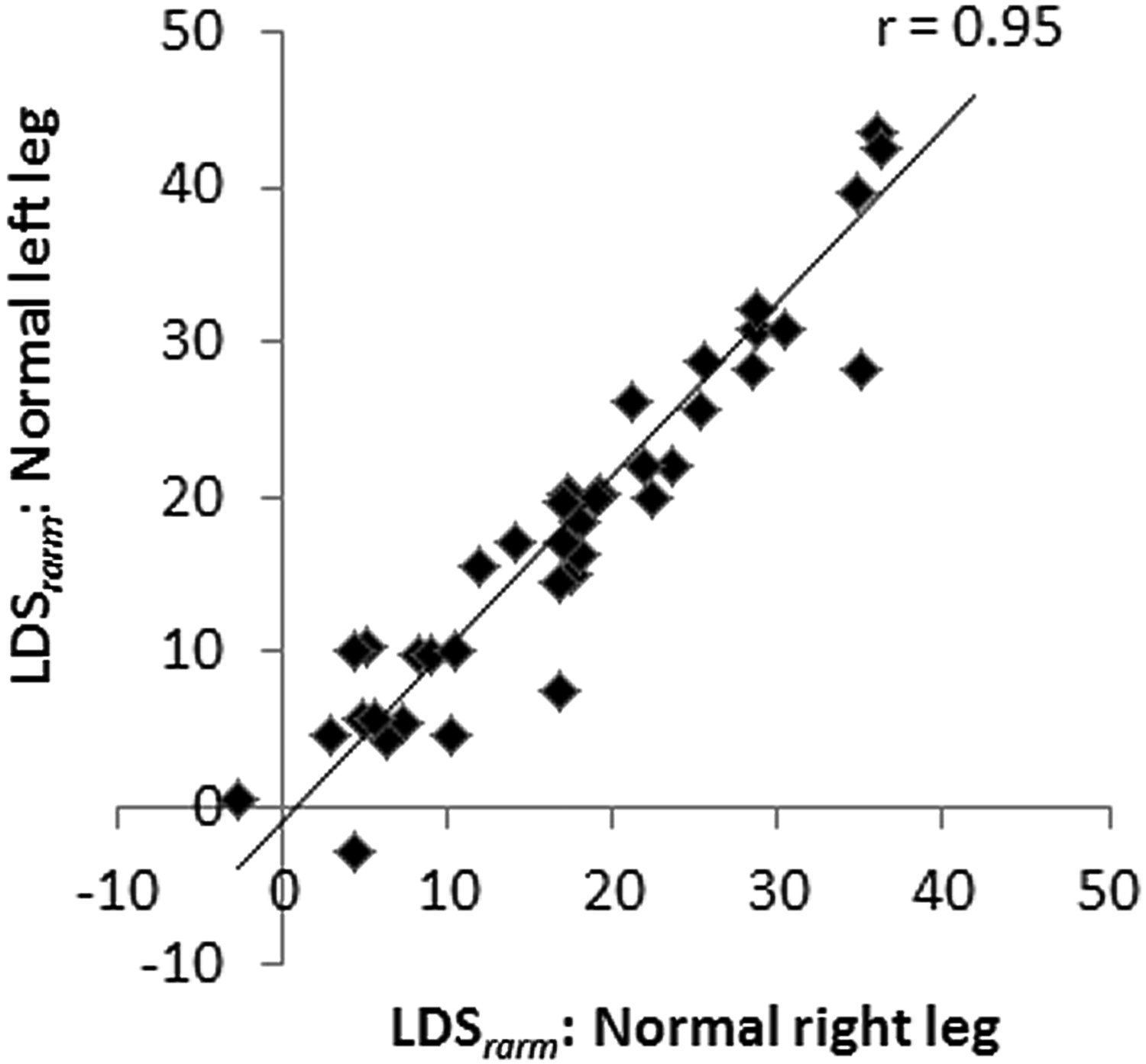
Correlation between LDS rarm in right and left legs in normal subjects. LDS rarm , L-Dex score calculated by using the right arm as a reference.
Discussion
We demonstrated that the use of LDS rarm might be a feasible alternative to that of LDS cont .
Ri/Recont and Ri/Rerarm reportedly show a very good linear correlation regardless of the presence of edema, 10 and bilateral leg lymphedema can be sensitively discriminated from normal legs using Ri/Rerarm. 7 However, it is also known that Ri/Re can be affected by various factors such as systemic disease 12 or aging. 7 Accordingly, it was not surprising that mean Ri/Rerarm in legs with edema was not statistically different from Ri/Rerarm in contralateral normal legs. Since systemic factors affect both legs, it seems reasonable to use the contralateral normal leg to cancel out these factors when calculating a parameter to indicate fluid status in a leg with edema. Although the formula used to calculate L-Dex score is not open, we speculate that this is more or less what is required to obtain the L-Dex score. It is also true that leg edema is more commonly seen in older people; therefore, the contralateral leg may not serve as a good control in this population. However, Ri/Re in the arms of older patients was as low as that in the legs and arms of younger normal subjects. Thus, it seemed reasonable to utilize the arm as a reference to calculate the L-Dex score. Moreover, mean ± 2 SD values for LDS rarm in normal right legs ranged from −3 to 37, and LDS rarm values corresponding to the normal range of LDS cont ranged from 1 to 34. Because these ranges were similar, it was speculated that the normal range of LDS rarm corresponding to the normal range of LDS cont might be suitable for use in detection of abnormal fluid status; this was also roughly the case for the contralateral normal legs in the current patients.
Limitations
The number of subjects included in this study might be too small to draw definite conclusions. The confirmation of unilateral nature of the leg edema was very difficult. For instance, the patient with post-thrombotic syndrome in whom the unilateral iliac vein is incompetent should have unilateral edema. However, risk factors such as obesity may cause venous stasis and, therefore, venous edema can occur in the other side. In unilateral lymphedema, the seemingly normal side should have more or less reduced lymphatic transport capacity, and, therefore, may cause minimal edema. Perfect exclusion of these conditions may be impossible as of present. In this study, control subjects were not age-matched with the patients. However, one third of the patients in this study were in their 70s or 80s, and, therefore, it was difficult to find “normal” age-matched controls in the hospital.
Conclusion
The use of LDS rarm seemed to be suitable as an alternative to that of LDS cont in the detection of abnormal fluid status in the leg.
Footnotes
Author Disclosure Statement
No competing financial interests exist.