
Abstract
Abstract
Background:
Fibrosis can enhance the exacerbation of lymphedema, which becomes obvious in late stage II–III lymphedema. However, whether far-infrared radiation thermotherapy (FIRT) can cure lymphedema fibrosis is still lack of research. This research was to investigate the therapeutic effect of FIRT on tissue fibrosis in the treatment of Late stage II–III lymphedema.
Methods:
Patients accepted only FIRT for a total of 20 sessions. The treatment session duration was 2 hours, and a stable machine temperature of 42°C was maintained throughout treatments. Clinical evaluation and laboratory evaluation were conducted before and after FIRT. Clinical outcome measures included circumference of affected extremity, skin elasticity, ultrasound, patients' subjective assessment, and quality of life (QOL). Laboratory outcome measures included serum and local lymphedema tissue fluid concentrations of fibrosis associated cytokines, tissue growth factor beta-1 (TGF-β1), interleukin (IL)-1β, IL-4, IL-18, and caspase-1.
Results:
Between 2015 and 2016, clinical evaluation of 64 patients with late stage II–III lymphedema was conducted. From this group, 12 cases (18.75%) underwent simultaneous laboratory evaluation. Circumferences of affected extremities improved significantly following treatment (p < 0.001). Skin elasticity of the affected extremity improved significantly (p < 0.05). Ultrasound investigation showed reduced fiber and dense material in the affected tissue (increased gray level 6.322% ± 7.624%, p < 0.001). Patients reported a subjective improvement of their symptoms such as decreased tightness, heaviness, solidity, pain, discomfort, and numbness (p < 0.001, p < 0.001, p < 0.001, p < 0.001, p < 0.001, and p = 0.032, respectively) and improved QOL (p < 0.001). Laboratory results revealed a significant decrease in local tissue fluid concentrations of TGF-β1 (p = 0.041) and IL-18 (p = 0.049) after course completion.
Conclusion:
FIRT provides an effective treatment for lymphedema tissue fibrosis; it reduces the concentration of fibrosis cytokines in local lymphedema tissues. Consequently, this treatment can reduce the density of fibrosed tissue in the affected extremity, increase skin elasticity, significantly improve clinical symptoms, and improve QOL of patients.
Introduction
L
Due to limited effectiveness of surgical treatment methods for late stage II–III lymphedema with fibrosis, conservative treatment modalities are most commonly adopted.1,10 Conservative treatments include manual lymphatic drainage, hyperthermia, intermittent air pressure wave therapy, compression bandaging, and medical therapy.7,11,12 The best effects are seen with early intervention using combined conservative treatment modalities, both slowing the development of fibrosis and relieving symptoms. 13
Far-infrared radiation thermotherapy (FIRT), developed as a conservative treatment for lymphedema by Chang, 14 has significant radiation, resonance, and thermal effects on local soft tissues. Far-infrared rays are able to deeply penetrate skin layers and resonate with water and organic molecules of our body. The human body is composed of 60% water in adult males and 55% in adult females. As FIR interacts with water molecules, it causes a thermal reaction which increases tissue temperature. The human body reacts to this phenomenon by dilating blood vessels. In this way, blood circulation is improved and more oxygenized blood reaches the soft tissue region being treated and, at the same time, stimulates the removal of accumulated toxins.15,16 In addition to alleviating lymphedema, it also has controlling effects on DLA. Patients undergoing FIRT experience a significant decrease in tissue hardness, leading to the suggestion that FIRT can reduce the amount of soft tissue fibrosis associated with chronic lymphedema.17,18 However, whether single FIRT can cure lymphedema fibrosis remains a matter of debate. This research combines clinical and laboratory outcome measures to investigate the effects of FIRT in the management of chronic lymphedema fibrosis.
Materials and Methods
Ethics
The study was approved by the Review Committee at The Shanghai Ninth People's Hospital. Written informed consent was obtained from all patients before treatment and enrollment into the study.
Inclusion criteria
Inclusion criterion was late in stage II–III unilateral limb lymphedema as defined by the International Society of Lymphology (ISL) classification 10 with a disease duration of less than 3 years.
Stage 0 refers to a latent or subclinical condition where swelling is not yet evident despite impaired lymph transport, subtle changes in tissue fluid/composition, and changes in subjective symptoms. It may exist months or years before overt edema occurs (stages I–III). Stage I represents an early accumulation of fluid relatively high in protein content (e.g., in comparison with “venous” edema) which subsides with limb elevation. Pitting may occur. An increase in various proliferating cells may also be seen. Stage II signifies that limb elevation alone rarely reduces tissue swelling and pitting is manifest. Late in stage II, the limb may or may not pit as excess fat and fibrosis supervenes and stage III encompasses lymphostatic elephantiasis where pitting can be absent and trophic skin changes such as acanthosis, further deposition of fat and fibrosis, and warty overgrowths have developed.
Patients with clinical or radiological evidence indicating potential malignancy or with comorbidities that would prevent FIRT and follow-up were excluded from the study. In addition, patients with a contraindication to heat and compression bandage treatments, such as DLA or vascular thrombosis, as well as those unable to provide consent or whose limb size exceeded the capacity of the treatment machine, were also excluded.
Therapeutic intervention
The FIRT machine (Fig. 1) (70 × 120 × 75 cm), which has been independently researched by the Ninth People's Hospital and Shanghai Jiao Tong University, generates infrared radiation (exhibited high emissivity [>0.8] between 6.0 and 14.0 μm wavelength) using an internal ring of eight far-infrared quartz lamps. The stainless steel encasing is resistant to high temperatures (around 42°C) and a temperature control device allows temperature adjustment of the specialized treatment cabin. The temperature on the skin was 39.5°C ± 0.5°C in the treatment session. There was a rotary knob facing patient for setting temperature, as well as a small display screen showing the real-time temperature. There also was a switch for cutting off the power beside the rotary knob. A slideable holder was placed in the cabin for fixing the lymphedema extremities. The upper part of this machine was also slideable. When the upper part slid over the lower part, this machine became a relatively airtight container for treatment. If not, the power would be cut off for safety.
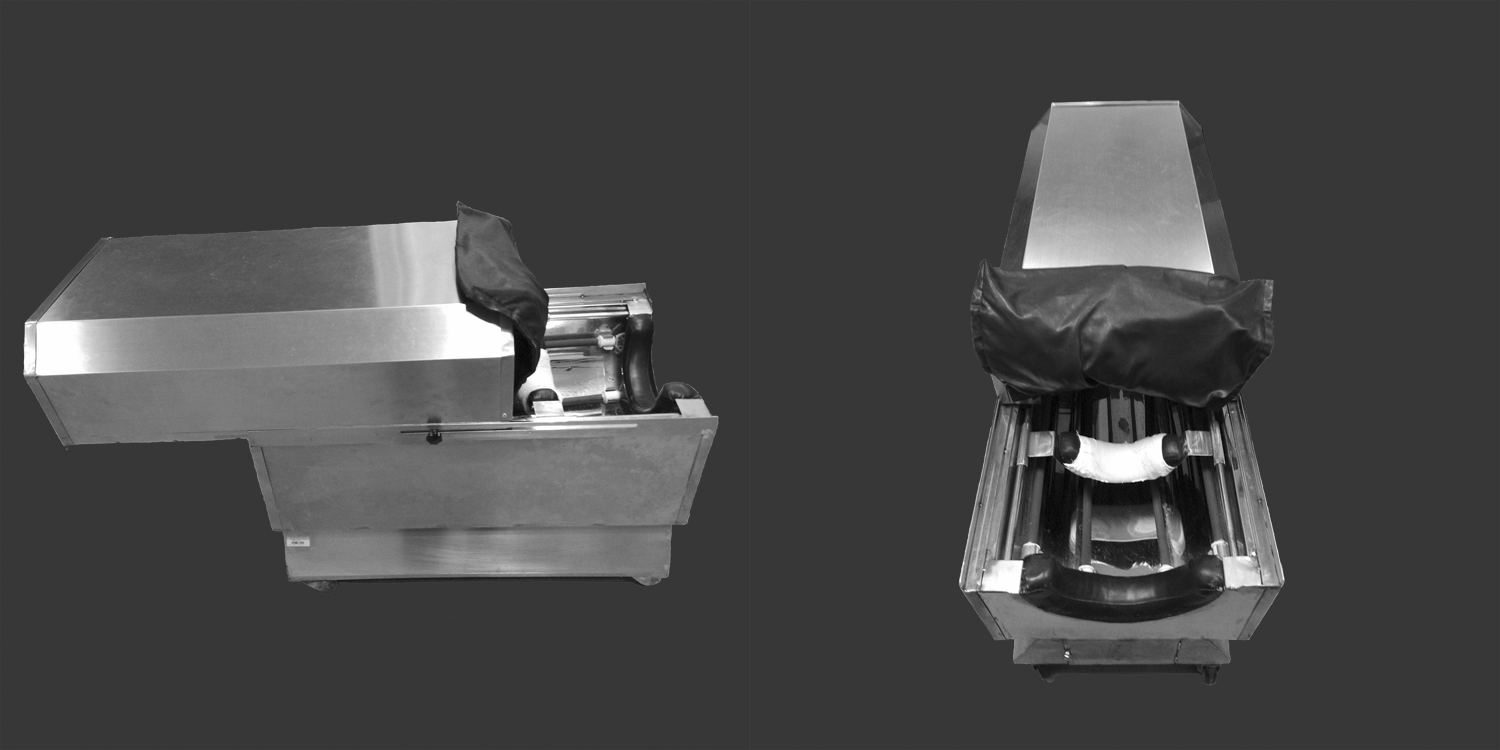
The machine used in our study can produce far-infrared ray (6–14 μm wavelengths) in its cabin made by the NO.9 hospital in Shanghai. Patients place their extremities in the cabin for treatment.
Patients underwent daily single far-infrared ray treatment for 4 weeks (5 working days per week) for a total of 20 sessions. The treatment session duration was 2 hours, and a stable machine temperature of 42°C was maintained throughout treatments.
Clinical evaluation
All clinical evaluations were conducted 1–2 days before the start of the treatment course and within 1–2 days of course completion. A total of five sites on the affected extremity were chosen for defined measurements: proximal third and distal third of the arm/thigh, proximal third and distal third of the forearm/leg, and middle of the dorsum of hand/foot (Fig. 2).
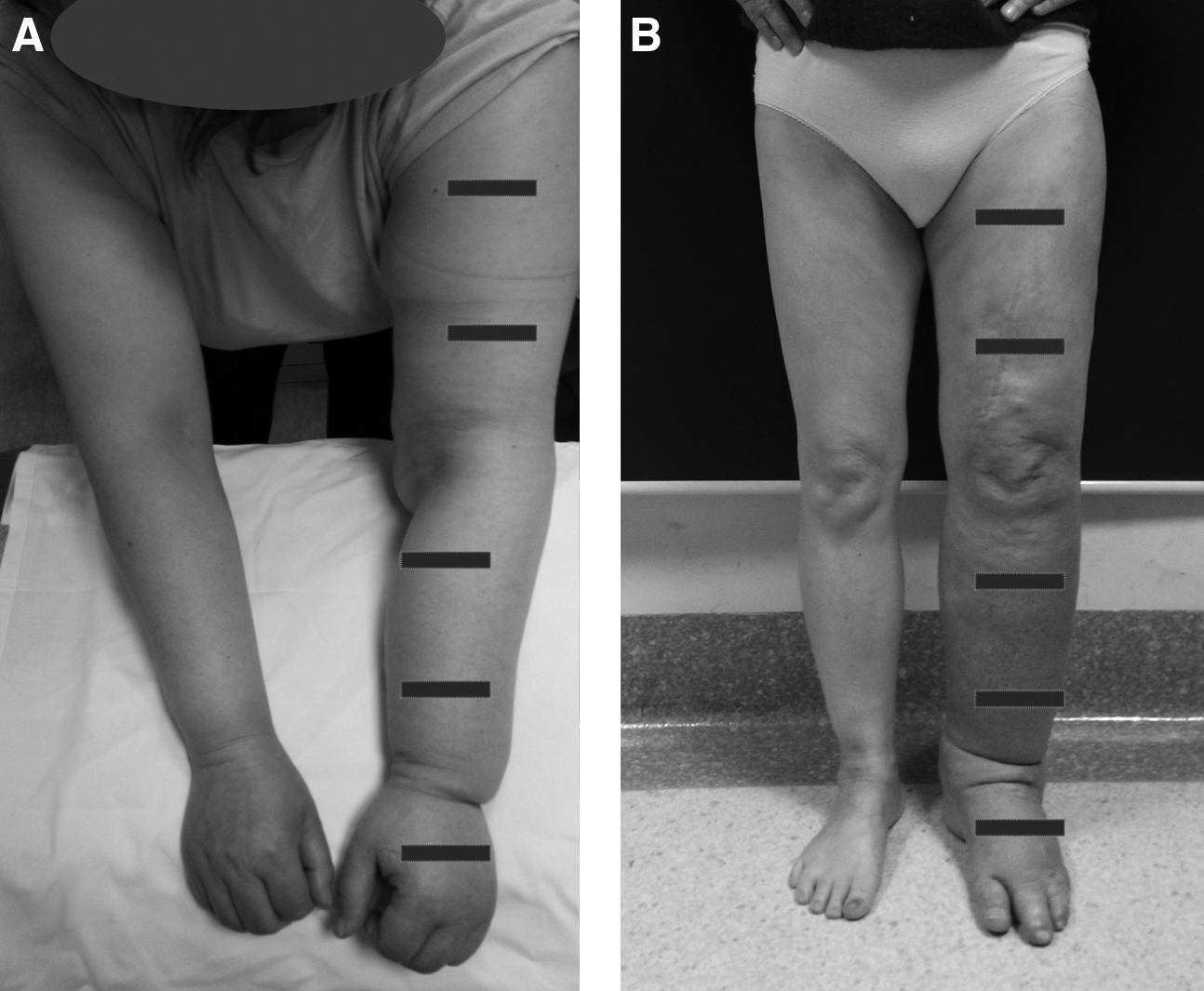
The exact detecting sites as marked on the extremities. A total of five sites on the affected extremity were chosen for defined measurements: proximal 1/3 and distal 1/3 of the arm/thigh, proximal 1/3 and distal 1/3 of the forearm/leg, and middle of the dorsum of hand/foot.
Circumference of affected extremity
The circumferences of the affected extremities on the five detection sites were measured with a tape by the same doctor. The data were recorded for final calculation.
Skin elasticity
Skin elasticity was assessed with a Cutometer® dual MPA 580 mounted with a 6 mm handheld probe. 19 The Cutometer assesses skin elasticity using a principle based on suction and elongation measurements. The device generates a negative pressure, drawing skin into the probe's central aperture, and estimates skin penetration depth using an optical measuring system. Constant Cutometer parameters used throughout the study were a vacuum pressure of 500 mbar, suction duration of 1 second, and a relaxation time of 1 second. Three repetitions of the measurement cycle were performed at each of the five sites along the affected extremity. Cutometer-specific elasticity parameters were recorded, and mean values were calculated. The Cutometer dual MPA 580 software plots a graph of skin deformation (mm) against time (second) from which R- and Q-parameters are calculated. R0 = Uf demonstrates the skin's elastic deformation ability; R2 = Ua/Uf measures gross elasticity; R5 = Ur/Ue measures net elasticity; Q0 also demonstrates the elastic deformation ability, positively correlates with R0, and negatively correlates with firmness.19,20
Ultrasound investigation
Dual images were obtained using Mindray Digital Ultrasound Imaging with a 10 MHz transducer 21 operated by the same doctor using same strength. The ultrasonic probe was under the same angle (vertical to the skin) during the examinations. Echogenicity measurements were taken using image gradiation scale analysis with Adobe Photoshop. Mean values were ascertained for skin and subcutaneous tissue.
Patients' subjective assessment scores
As no instrument for measuring changes in lymphedema-related symptoms exists, clinical symptoms were quantified using patients' subjective assessment of six lymphedema-related symptoms. These were as follows: tightness, heaviness, solidity, pain, discomfort, and numbness. 22 Visual analog scale (VAS) scoring ranged from 0 to 10 (0 = absent, 10 = worst).
It is universally acknowledged that quality of life (QOL) can be heavily influenced by the presence of chronic disease and, therefore, provides a useful tool for assessing treatment outcomes. QOL was scored on a scale adapted from Lee and Bergen's evaluation criteria which assesses the degree of physical, psychological, and socioeconomical limitation imposed on the patient by their lymphedema symptoms. 23 The scale ranges from 0 to 5 (0 = profound limitation, 5 = no limitation). Higher scores reflect a better QOL.
Adverse reactions
The treatment site was inspected daily to ensure that the occurrence of any adverse reactions, such as rashes, burns, or infection, was recorded.
Laboratory evaluation
For those patients undergoing laboratory evaluation, tissue fluid and venous blood samples were collected, under the sterile conditions of the operating room, within 48 hours preceding the first treatment and 1–2 days after the final treatment.
Tissue fluid collection
A 25G syringe needle was penetrated into skin for 3–4 mm. The doctor gently pressed the skin around the needle and made the tissue fluid outflow along the needle. Then he sucked up the tissue fluid with 1 mL syringes. Tissue fluid was obtained from three points, including proximal third of the forearm/leg, distal third of the forearm/leg, and middle of the dorsum of hand/foot. The samples were preserved in the Eppendorf (EP) tubes.
Venous blood collection
The venous blood was obtained from median cubital vein by 23G syringe needle and 5 mL syringes. The samples were preserved in the EP tubes.
Centrifugation was performed at constant temperature (4°C) on 0.5 mL tissue fluid and 0.5 mL blood samples at reactive centrifugal force (RCF) = 2.5 × 103 g for 10 minutes and then RCF = 12 × 103 g for 5 minutes to obtain supernatants for further analysis. Detection and measurement of cytokine concentration were performed using protein microarray (Radiation Biotech) for cytokines interleukin-1 beta (IL-1β), interleukin-4 (IL-4), interleukin-18 (IL-18), and tissue growth factor beta-1 (TGF-β1) and using ELISA (R&D) to detect caspase-1.
Statistical methods
The paired T-test was used to compare the changes in skin elasticity, skin ultrasound gradiation value, patients' subjective feedback scores for clinical symptoms and QOL, and the changes in fibrosis related cytokine concentrations before and after treatment with FIRT. All data analyses were conducted using SPSS version 19.0 (significance p < 0.05).
Results
Patients
A total of 64 patients were enrolled in the study (Fig. 3), of which 18 were diagnosed with upper extremity lymphedema and 46 with lower extremity lymphedema. In accordance with ISL classification, 40 patients (62.5%) were diagnosed with lymphedema in late stage II and 24 patients (32.5%) in stage III (Table 1).
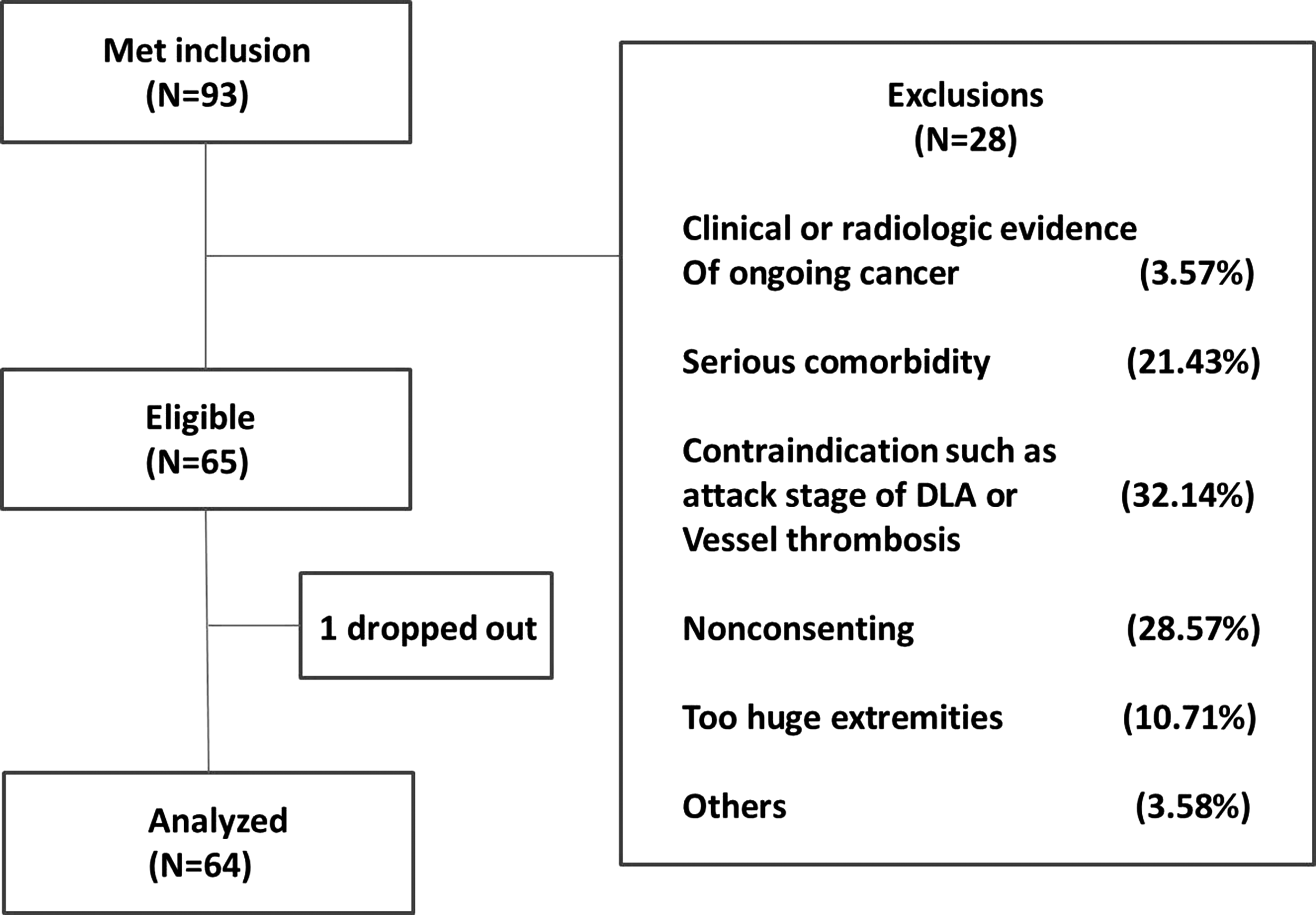
Consort diagram of patient flow. There were 93 patients meeting the inclusion, 28 of whom were excluded and 1 dropped out. Finally, 64 patients were analyzed. DLA, dermatolymphangioadenitis.
Circumference of affected extremity
The mean circumference of five examination sites in affected extremities in 64 patients before FIRT was 36.838 ± 11.194 cm. After FIRT, this mean circumference was 34.259 ± 11.115 cm. It showed that the circumferences of lymphedema extremities were improved significantly (p < 0.001).
Skin elasticity
Mean elasticity parameters for the affected extremity in our 64 patients at the start of the study were R0 = 0.020 ± 0.003 U, R2 = 0.354 ± 0.031 U, R5 = 0.736 ± 0.083 U, and Q0 = 4.153 ± 0.616 U. Results after receiving 20 sessions of FIRT over the 4-week treatment course period were significantly improved and the parameters increased as follows: R0 = 0.026 ± 0.003 U (p = 0.001), R2 = 0.434 ± 0.036 U (p = 0.031), R5 = 0.968 ± 0.096 U (p = 0.005), and Q0 = 5.364 ± 0.686 U (p = 0.001) (Fig. 4). These results show that FIRT increases skin elasticity for patients diagnosed with late stage II–III lymphedema with fibrosis.
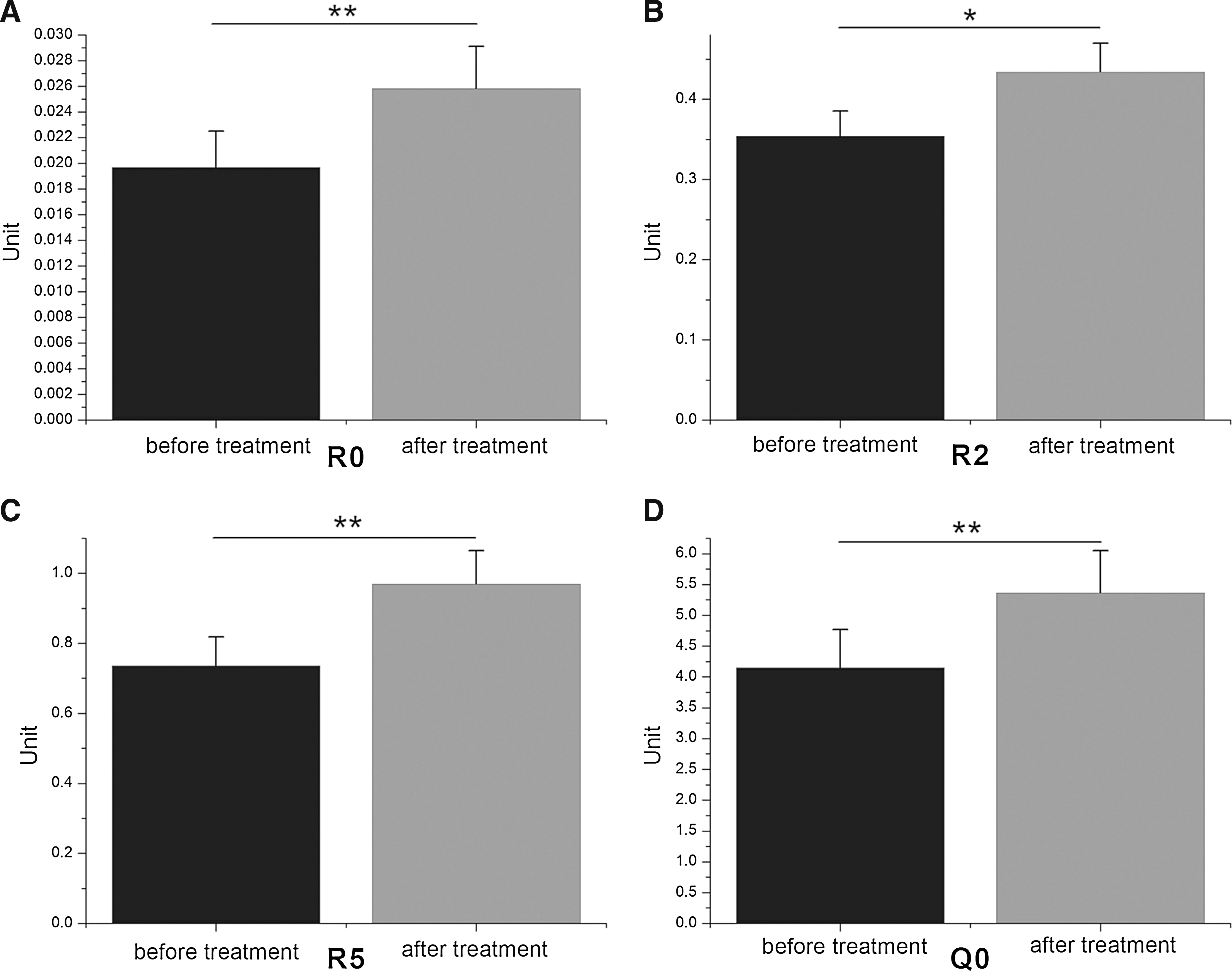
The results of detection for elasticity with Cutometer® (MPA580; Courage+Khazaka).
Ultrasound examination
The mean gradiation values at the five defined sites were 57.516% ± 5.934% before FIRT. After treatment, gradiation values were significantly increased 63.838% ± 7.83% (p < 0.001). A substantial reduction in the abundance of fibrous banding within subcutaneous tissues could be seen when comparing pre- and posttreatment images; an example is shown in Figure 5. These findings were consistent in image analysis for all of our patients.

The ultrasound images of lymphedema tissues and changes in gray scale of ultrasound images.
Patients' assessment scores
The mean VAS scores for tightness, heaviness, solidity, pain, discomfort, numbness, and QOL before FIRT were 7.313 ± 1.447, 6.438 ± 1.190, 7.031 ± 1.178, 4.906 ± 1.304, 6.938 ± 1.134, 0.188 ± 0.471, and 0.188 ± 1.600, respectively. After treatment, the scores for clinical symptoms were significantly reduced to 3.813 ± 0.896, 4.313 ± 0.896, 3.375 ± 0.942, 3.188 ± 0.965, 5.063 ± 0.982, and 0.000 ± 0.000 (p < 0.001, p < 0.001, p < 0.001, p < 0.001, p < 0.001, p < 0.001, and p = 0.032, respectively). The mean reported QOL score was higher (2.188 ± 1.120); this increase was significant (p < 0.001) (Fig. 6 and Table 2). These score changes for patients' reported symptomology and QOL indicate that FIRT can instigate subjective improvements in their condition.
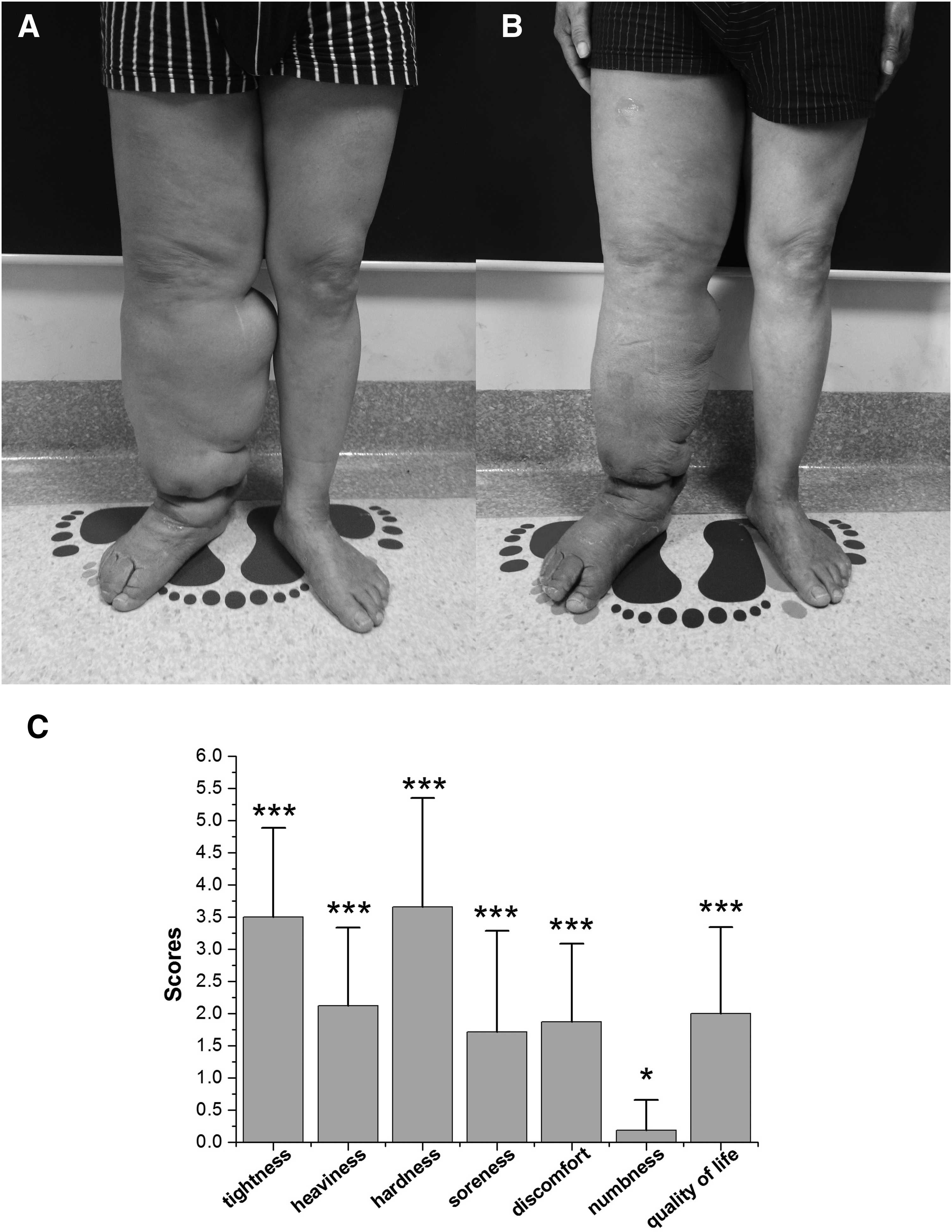
Improvement of patients caused by far-infrared treatment.
±VAS score/arbitrary units.
QOL, quality of life; VAS, visual analog scale.
Adverse reactions
No adverse reactions were reported during the study.
Laboratory results
For the group of 12 patients (18.75%), protein microarray and ELISA analysis revealed decreased IL-18 and TGF-β1 concentrations in lymphedema tissue fluid after FIRT (p < 0.05). The mean concentration ± standard deviation was 13.29 ± 25.416 pg/mL (p = 0.049) and 817.14 ± 1478.816 pg/mL (p = 0.041) for IL-18 and TGF-β1, respectively. The other cytokines were not found to be significantly lowered (p > 0.05) after treatment; mean tissue fluid concentrations ± standard deviations were as follows: IL-1β: 0.016 ± 0.075 pg/mL, IL-4: 0.001 ± 0.733 pg/mL, and caspase-1: 124.8 ± 422.03 ng/mL (Table 3).
p < 0.05.
IL, interleukin; TGF-β1, tissue growth factor beta-1.
Posttreatment serum cytokine concentrations were not found to be significantly changed from preliminary values (p > 0.05). These were −0.013 ± 0.049, −1.033 ± 5.282, −2.443 ± 7.866, and 0.257 ± 34.532 ng/mL for IL-1β, IL-4, IL-18, and caspase-1, respectively; TGF-β1 was not detected (Table 3).
The decrease in local IL-18 and TGF-β1 concentrations demonstrates that FIRT can have the effect of reducing the local concentration of specific cytokines associated with fibrosis in lymphedematous tissues; however, it does not have an obvious effect on the circulating blood concentration of fibrosis cytokines.
Discussion
Inflammation, fibrosis, swelling, and lymphatic regeneration are four main aspects of the pathophysiological changes seen in lymphedema patients.7–9 The extent of tissue fibrosis is proportional to the severity of the lymphedema; hence, it provides a useful tool when assessing the state of disease in those patients diagnosed with lymphedema. Laboratory investigations have shown that specific cytokines, such as TGF-β1, identified as having an influential role in fibrosis pathogenesis and fibrin deposition, are present in greater abundance in those patients with chronic lymphedema and fibrosis. Fibrosis inhibits the regeneration and recanalization of lymphatic vessels, which can worsen the symptoms.3–6 The clinical manifestations of lymphedema, including tissue and skin changes, swelling, inflammation, and pain, can impose overwhelming effects on the appearance and function of the affected extremity and, in doing so, impact upon patients' QOL.
As mentioned previously, far-infrared radiation exerts radiation, resonance, and thermal effects on tissues. Exposure to electromagnetic radiation of wavelengths between 3.0 and 1000 μm allows for both generation of free charge and ion oscillation, resulting in the breakdown of large molecules such as protein that are present in the local tissues. The thermal mechanism of effect arises through expansion of local blood and lymphatic vessels, improving flow in the microcirculation and increasing immune system activation.11,15 Liu and Olszewski demonstrated that local hyperthermia can activate Langerhans cells, macrophages, and endothelial cells and, through increased MHC II-antigen complex presentation to and activation of CD4+ T cells, lead to increased cytokine production. Increased nonspecific macrophage and natural killer cell activity enhances immune function and aids the alleviation of the local immune disturbance seen in lymphedema patients by promoting microcirculation reflux.11,18,24,25 In addition, activated macrophages phagocytose and hydrolyze excess proteins present in the lymphedematous tissues, reducing the colloid osmotic pressure and promoting lymph circulation. Hu and Li also confirm that local hyperthermia can increase the flow in the local microcirculation, reduce chronic inflammation, and promote self-repair.26–28
Therefore, we considered that FIRT may improve the fibrosis in lymphedema tissues by increasing the backflow of microcirculation, as well as decreasing the collection of inflammatory cells in local tissues. The reduction in pro-inflammatory cytokines would reduce the overreaction of fibroblasts and decrease the amount of TGF-β1 which could increase the production of collagen. Simultaneously, FIRT may result in the breakdown of proteins and contribute to the phagocytosis and hydrolysis of excess collagens by nonspecific macrophages.
Skin elasticity provides a meaningful quantitative measurement of skin quality.29,30 Nicoli et al. 31 reported that chronic lymphedematous tissue is prone to fibrosis and hardening of the skin leading to the loss of the clinical sign of pitting edema. It is assumed that the loss of the ability to reversibly change shape during the application of force can also be seen as a failure of skin elasticity due to the underlying tissue fibrosis.
In our research, we found that the skin elasticity parameters R0, R2, R5, and Q0 increased (p < 0.05) after treatment. These results confirm that FIRT can improve skin elasticity. We suggest that the mechanism of effect through which this change is brought about is twofold. First, the promotion of lymph circulation 11 and increased removal of fibrosis-associated cytokines lead to a reduction in local concentrations within lymphedema tissues. Second, FIRT can reverse immune dysfunction in the affected extremity by reducing the activation of inflammatory pathways involved in the production of fibrosis-associated cytokines. 32 We believe that the culmination of these effects allowed for the alleviation of fibrosis in our patients.
Tassenoy et al. advocate the use of ultrasound as a noninvasive, convenient, and cheap modality for detecting morphological changes in lymphedema patients.21,33,34 Our preliminary comparisons of lymphedema tissue with normal tissue revealed that ultrasound gradiation values for the tissue of the affected extremity were reduced. This is representative of the enhanced echogenicity and increased tissue density exhibited by fibrosed tissues. In addition, multiple hyperechoic strips depicting fibrous bands were detected providing further evidence of the condition of the fibrosed tissue.
In our research, we found that the ultrasound gradiation values of the affected tissues were significantly increased (p < 0.05) after FIRT treatment, as visible in Figure 5. Hyperechoic fibrous banding within the subcutaneous tissue was also reduced.
Common clinical symptoms of lymphedema include a sense of tightness, heaviness, pain, hardness, discomfort, swelling, weakness, and numbness. Tsai et al. describe these symptoms, excluding swelling and weakness, as being attributable to the presence of fibrosis. 22 Moreover, it is widely accepted that patients' QOL is significantly reduced by the persistence of lymphedema and the development of subcutaneous fibrosis. The quantitative criteria established by Lee and Bergan 23 allow for an effective assessment of QOL.
Our study showed that, after completion of a single FIRT course, the QOL scores and patient feedback scores for clinical symptoms both improved significantly (p < 0.05).
Avraham3,35–39 has identified TGF-β1, IL-1β, IL-4, IL-18, and caspase-1 as specific cytokines that promote the development of fibrosis. In line with the positive correlation between lymphedema disease progression and worsening fibrosis, Savetsky et al. 38 has demonstrated that TGF-β1 and IL-4 function can inhibit lymphatic regeneration which could lead to the exacerbation of lymphedema symptoms. Cao et al.17,18 noted that inducing local hyperthermia with heat treatment modalities decreases the gene expression of TGF-β1. Furthermore, they found that gene expression of collagen types I and III was also reduced, indicating the potential for local hyperthermia to improve tissue fibrosis.
Concurrently, our results show that FIRT can decrease local lymphedema concentrations of TGF-β1 and IL-18 (p < 0.05). The improvements recorded in those patients' subjective assessment of clinical symptoms and QOL, as well as improved ultrasonic examination results and increased skin elasticity, give further evidence to support the clinical picture of fibrosis alleviation. Our results support the hypothesis that FIRT functions to reduce the local concentration of fibrosis-associated cytokines, reduce tissue fibrosis, and promote lymphatic flow. 11 The reduction in cytokine concentration results from reduced macrophage deposition within target tissues, which thereby inhibits the production of fibrosis-associated cytokines by inflammatory mediators. 32
Limitation
The principle aims of this study were focused on the effect of far-infrared radiation on tissue fibrosis in the treatment of patients with chronic lymphedema. However, if patients did not accept any subsequent therapy, such as bandage treatment, for maintaining curative effect, the fibrosis must be serious again. Therefore, better treatment outcomes are most often achieved with combined conservative treatment modalities. 13 The reduction of lymph aggregation and increase in lymph circulation achieved by the application of external pressure have been described; Zaleska et al. 40 believe that the application of external pressure promotes the formation of new channels within lymphedema tissue. Therefore, we suggest a combination of FIRT and subsequent pressure treatment modalities for patients with chronic lymphedema, to achieve more satisfactory results.
Conclusion
To sum up, FIRT provides an effective treatment modality for chronic lymphedema with fibrosis. Our study demonstrates that FIRT reduces the concentration of fibrosis-associated cytokines within the local subcutaneous tissues. We believe that this leads to increased skin elasticity over the affected extremity and improves the clinical symptoms for patients affected by this chronic condition.
Footnotes
Acknowledgment
This research was supported by National Natural Science Foundation of China (81272146).
Author Disclosure Statement
No competing financial interests exist.