
Abstract
Abstract
Background:
The therapeutic intermittent pneumatic compression (IPC) pressures are usually set arbitrarily at levels between 40 and 60 mmHg. However, it is not known how much force has been transferred to edema fluid. There is a need to know how high edema fluid pressures should be generated to evacuate the stagnant fluid. The externally applied compression force dissipates in hard tissues and only a portion of it is conveyed to tissue fluid. Simultaneous measuring of compression force using deep tissue tonometry and recording edema fluid pressures under a tonometer would give hints of how high should therapist or patient set IPC pressures to mobilize fluid.
Aim:
(1) To simultaneously measure the applied tonometer force and the generated edema fluid pressures under the tonometer, (2) to plot tonometer force against fluid pressure data to create a correlation curve for setting pressure of IPC at levels initiating fluid flow, (3) to work out a formula for setting pressures in the pneumatic device for individual patient, based on tonometry, (4) to prove the value of formula on a cohort of patients treated with IPC.
Methods:
Deep tissue tonometry force and tissue fluid pressures under the tonometer indentor were measured in lower limbs in a group of 20 patients with lymphedema stages I–III.
Results:
(1) Deep tissue tonometry penetrating to a depth of 10 mm provided data on pressure generated in tissue fluid under the tonometer indentor. (2) Plotting the applied tonometer force against the tonometer-generated tissue fluid pressures revealed that force to reach the threshold of 30 mmHg fluid pressure necessary for initiation of flow should be >1000 g/sq. cm. (3) A formula, based on tonometry values, for setting ICP pressures at levels generating pressures for initiating edema fluid flow was worked out. (4) Usefulness of the formula for setting IPC at effective levels was proved on a cohort of patients.
Conclusions:
Deep tissue tonometry of limbs is useful for setting IPC devices at compression pressures for mobilizing edema fluid.
Introduction
C
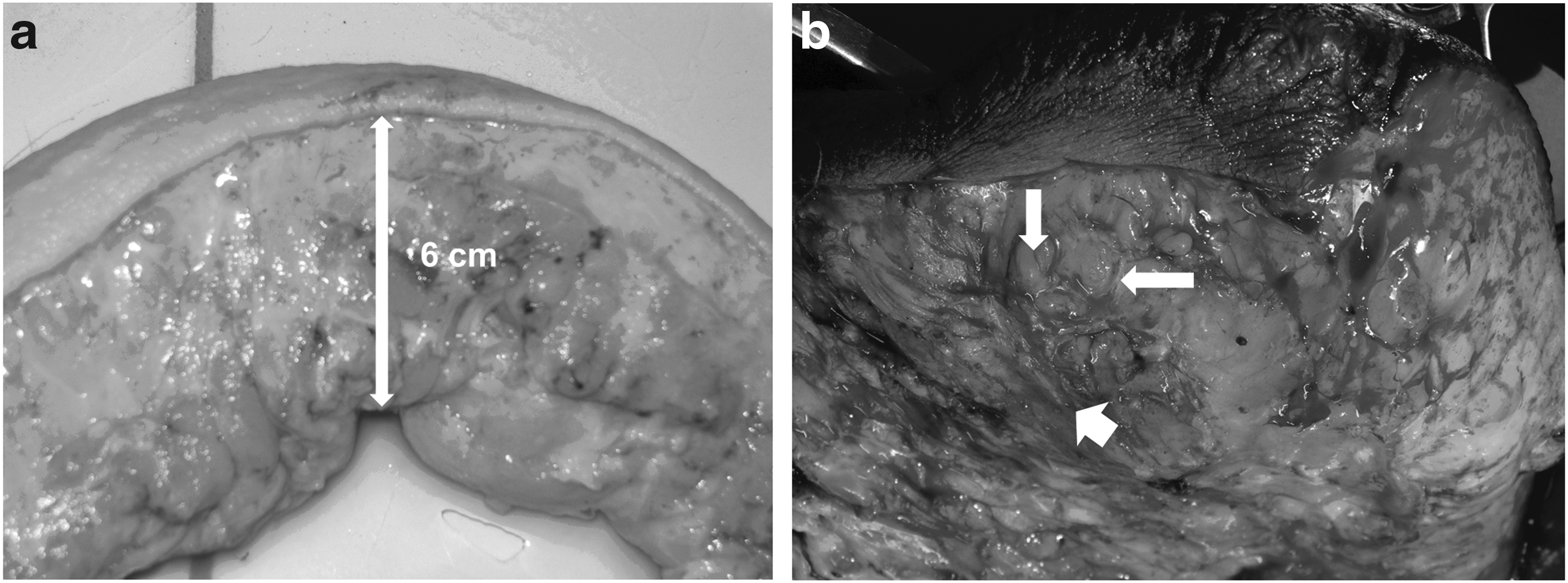
Skin and subcutaneous tissue have viscoelastic properties of a sponge. These properties depend on the density of cells and collagen and elastic fibers. Moreover, the blood microvasculature filled up with blood under the pressure of minimum 40 mmHg is another factor responsible for tissue turgor, in a mechanism similar to that observed in the corpora cavernosa. In lymphedema, there are additional physical factors that decrease tissue elasticity. One is excess stagnant tissue fluid located between collagen fiber bundles, others are hyperkeratosis and dermal and subcutaneous tissue fibrosis (Fig. 1). In advanced stages of lymphedema, the increasing cell and collagen mass outweighs the tissue fluid volume. Thickness of the subcutaneous tissue increases in some regions by 2–6 cm (Fig. 2a, b).

Schematic presentation of different proportions of fibrous tissue and mobile tissue fluid volume at various levels of the lymphedematous lower limb. In lymphedema, increased volume of limb is the sum of excess extracellular fluid (edema fluid) and increased cell and ground matrix mass.
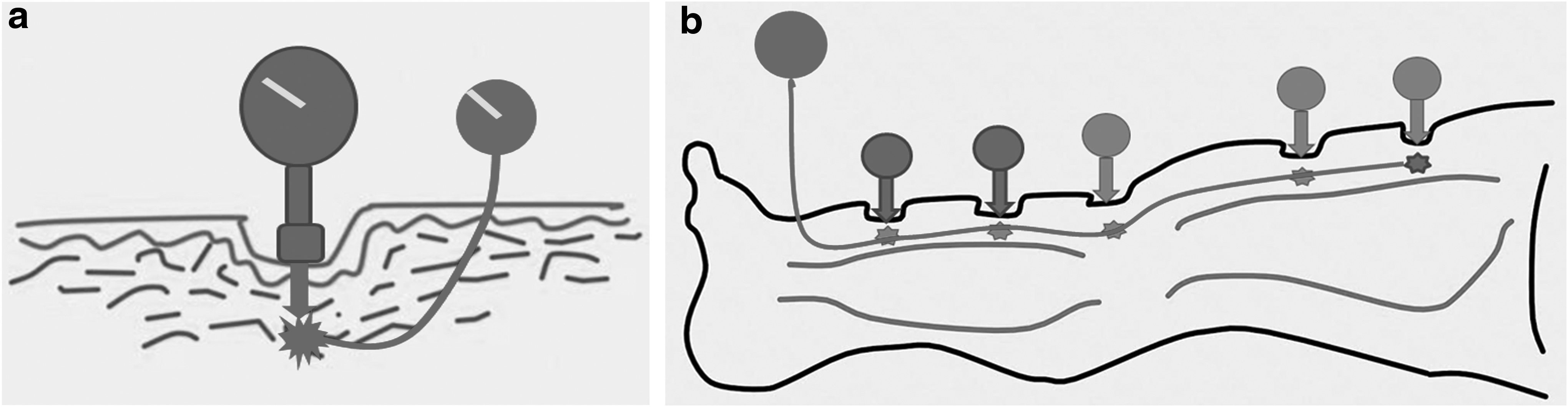
During therapeutic compression of limb, the external force is transmitted through the thick tissue layer from skin surface down to muscular fascia along solid structures as cells, collagen and elastic fibers, and ground matrix (Fig. 3). Deformation of these structures generates pressure that is conveyed to the edema fluid contained in the interstitial space. Fluid is squeezed out and flows away according to the pressure gradient and tissue hydraulic conductivity. Subsequently, its pressure drops. Thus, two different pressures can be observed in tissues during compression. One is that in solid tissue elements, another is that generated in tissue fluid by deformation of the solid elements. Tissue fluid pressure is always lower than that in solid elements. From the clinical point of view, the solid tissue pressure is not as important as that of edema fluid. Its high level generated by compression generates a gradient, enabling fluid evacuation.
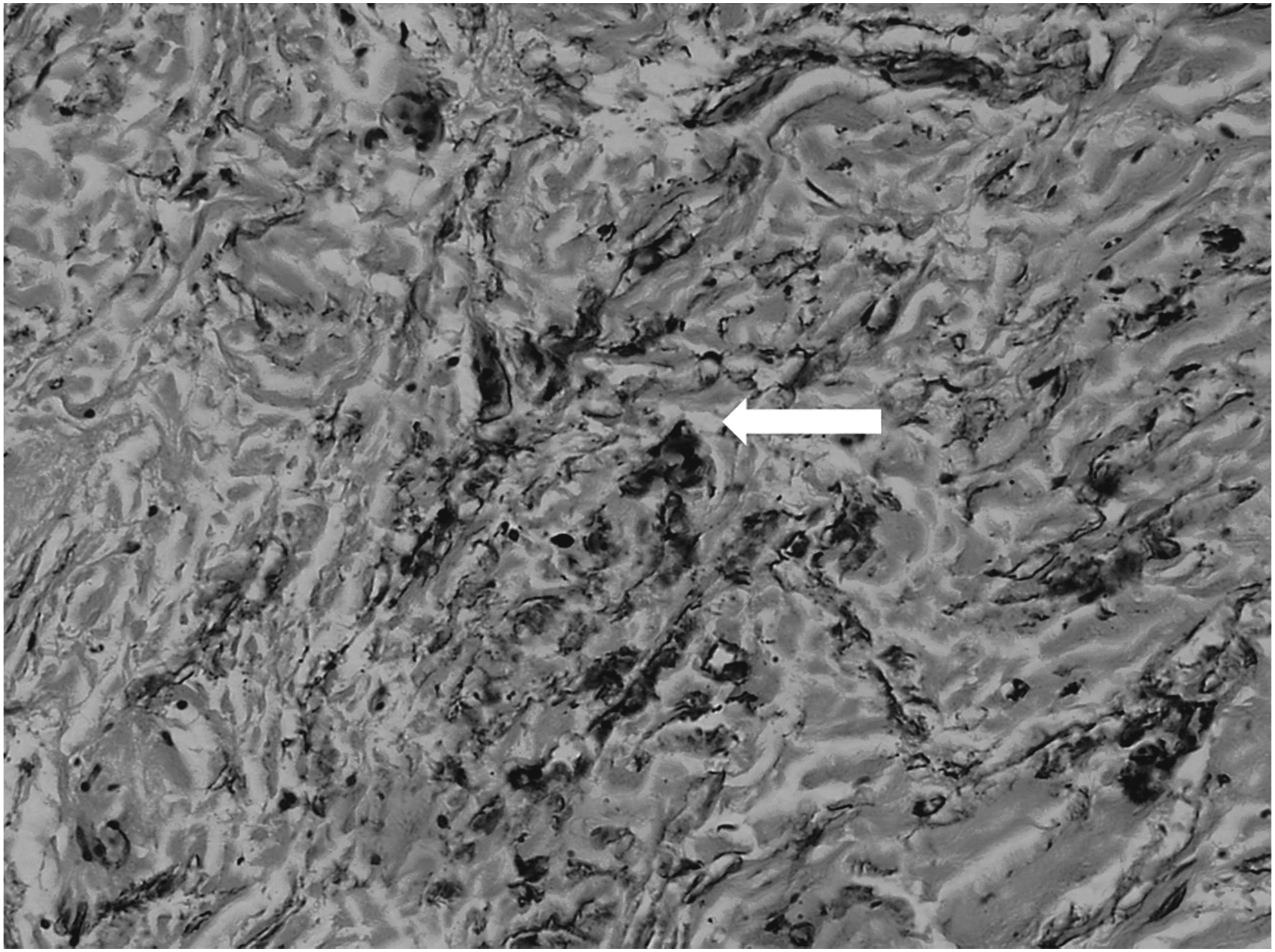
The structure of the subcutaneous tissue in lymphedema stage III. Bundles of collagen fibers dissociated by mobile edema fluid, forming tissue spaces and channels (arrow). Fluid pressure built up by external compression is measured in these channels.
The information on how high should the fluid moving pressure be in the lymphedematous tissue during pneumatic compression would be helpful for setting the compression device at an effective force. Such data could be obtained by measuring fluid pressure under the indenting tonometer. The tonometer should have an indentor long enough to penetrate deep tissues, force scale, and known surface area. The length of the experimental tonometer indentor was set based on the range of decrease of calf circumference after 1 hour of IPC at 50–120 mmHg. It was 6–10 mm. Accordingly, the length of tonometer indentor was set at 10 mm. It was assumed that force (pressure) used to put the tonometer indentor 10 mm deep should correspond to that needed for effective IPC.
A group of 25 patients with lymphedema of lower limbs stages I–III was studied. The aim of the study was (1) to measure the applied tonometer force and edema fluid pressures generated by the tonometer, (2) plot the tonometer force against the generated pressure data for creation of a correlation curve. Use of such a curve would be useful for setting pneumatic compression pressures at levels for initiating fluid flow, (3) based on the created curve, a simple formula was worked out for setting effective pressures in the pneumatic device for an individual patient, and (4) the compression effects of IPC set levels were evaluated based on that formula.
Material and Methods
Patients
The study was carried out on 20 patients, aged 28–62 years, mean weight 68 kg (58–76), mean height 168 cm (159–178), body mass index range 21–25, with diagnosis of lymphedema of one lower limb, stages I–III, duration of 2–15 years. Cases with acute inflammation, chronic venous insufficiency, and systemic etiology of edema were excluded from the study. The study was approved by the Warsaw Medical University Ethics Committee. Informed consent of patients was obtained.
Clinical staging
Staging was based on clinical evaluation: level of edema embracing the limb from foot to groin and degree of skin keratosis and fibrosis. In brief, in stage I, pitting edema was limited to the foot; in stage II, pitting edema affected the foot and lower half of the calf; in stage III, foot and calf were involved, with hard foot and ankle area skin; in stage IV, the whole limb was edematous with foot, and calf skin hyperkeratosis and papillomatosis of toes. 1
Lymphoscintigraphic staging was based on obtained images. In stage II, there was spread of tracer in the foot and lower part of calf, interrupted outline of a single lymphatic and few small inguinal nodes with irregular outline. In stage III, no draining lymphatics were seen with some inguinal nodes of irregular outline appearing after 2 hours since tracer injection. Stage IV was characterized by spread of tracer in the foot and entire calf without observation of collecting lymphatics and nodes. 2
Study setting
The study was carried out in three steps. In step 1, tonometry and tissue fluid pressures under the penetrating tonometer were measured, in step 2, tissue fluid pressures were recorded under the IPC sleeve, and in step 3, IPC device pressures were set for therapy based on the tonometry data, and compression effects were evaluated thereafter.
Tonometry
A deep tissue tonometer of our construction was used (Fig. 4). It was composed of a manometer (Wagner, Seattle, WA) connected to a 10 mm long round-bottom-shaped indentor of 1.13 cm diameter corresponding to 1 sq. cm (Fig. 5). It was pressed against tissues to the depth of 10 mm within 5 seconds. The applied force was read off on the manometer scale and expressed in g × 10(3)/sq. cm. To obtain accurate indentation of 10 mm, the two 2 cm long elastic metal wings were installed on the device with diodes at their end to light up upon contact with the surrounding skin (Fig. 6). In our method of tonometry, the penetration depth was fixed and the force values depended on the tissue elastic modulus. The tonometer was applied perpendicularly to the tissue surface. To avoid differences in data because of the use tonometer by various investigators, all measurements were taken by the same person.
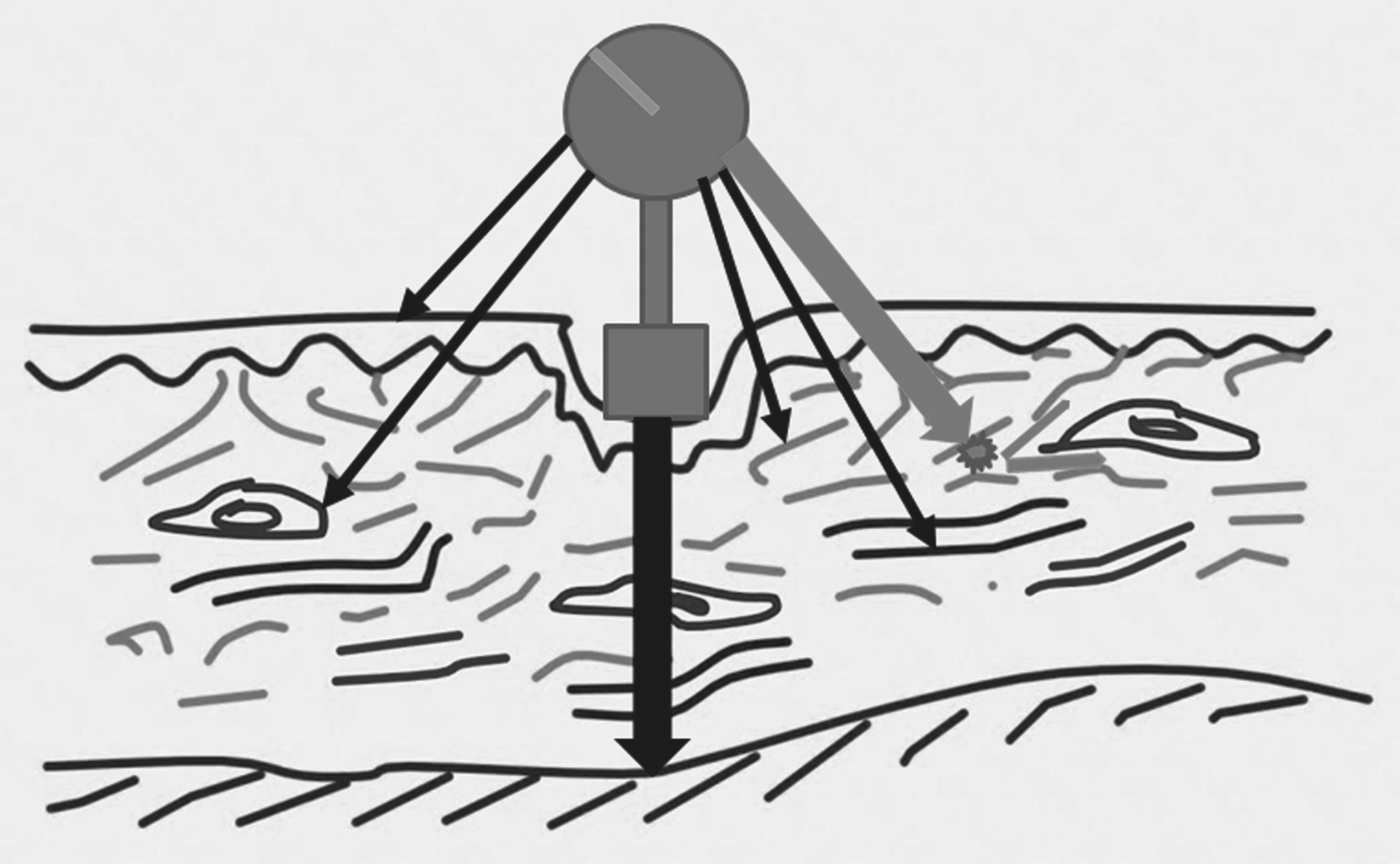
Tonometer measures the force necessary to overcome the resistance of epidermis, cells, collagen bundles, blood capillaries, and arterioles filled with blood under pressure of 40 mmHg and mobile tissue fluid (edema fluid) (thin arrows). Externally applied force (tonometer) is transferred through the solid tissue elements down to the fascia (thick vertical arrow) and pressure measured at this level will be that as applied on skin surface. This is as cells and fibers and fat globules are noncompressible and undergo only local deformation. The situation is different with mobile tissue fluid that, although noncompressible, moves away from under the tonometer through tissue spaces (thick oblique and two thin arrows). In effect, its pressure will be much lower than that measured in solid elements. Plotting applied force against tissue fluid pressure provides information how forceful should be pneumatic compression, bandaging, or garments.
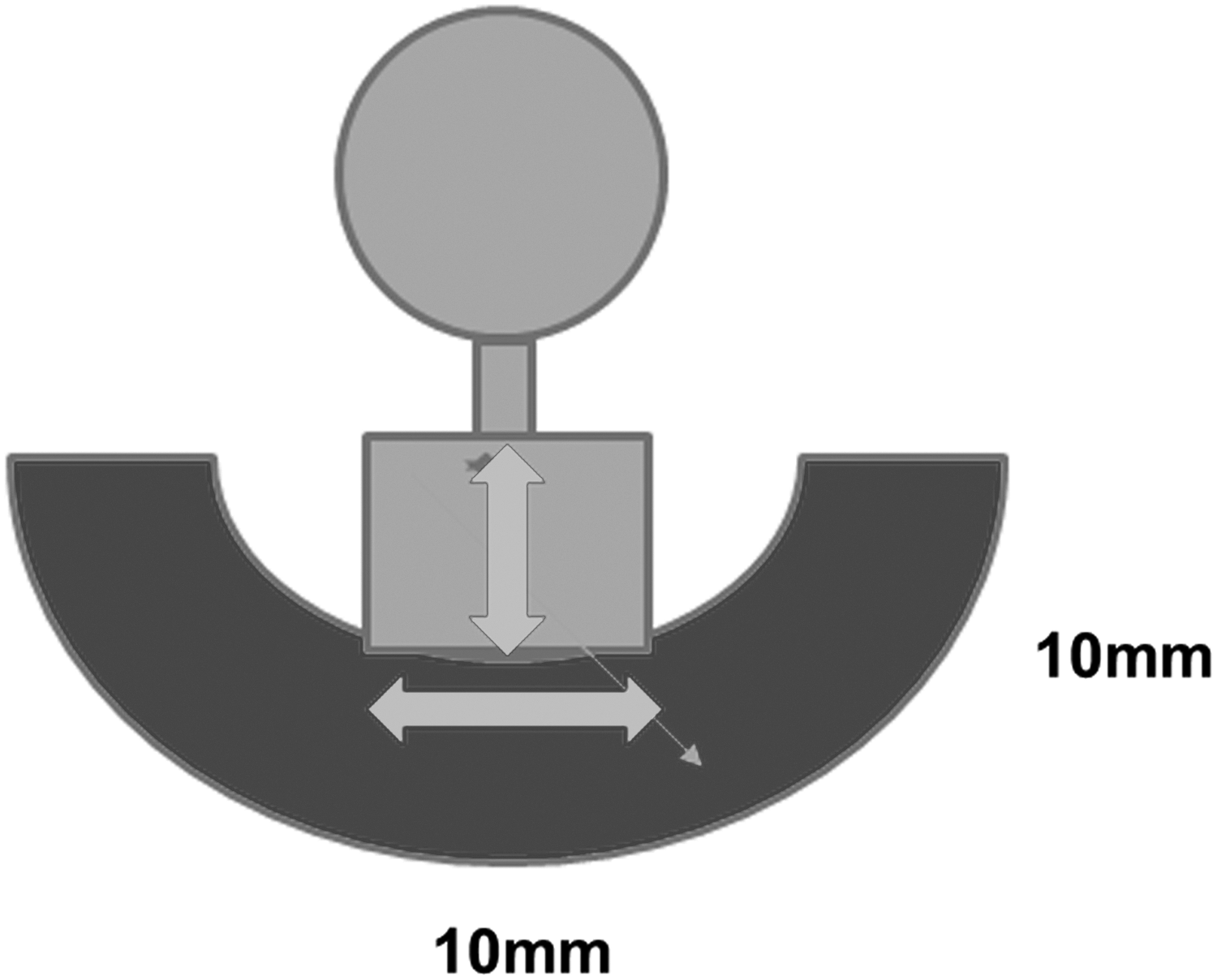
Scheme of a deep tonometer with 10 mm deep and 1.13 mm diameter indentor. The depth of 10 mm is the minimum to measure the compressibility of skin and upper layers of the subcutaneous tissue. Previously used tonometers penetrated 3 mm, which was the thickness of skin only, but not subcutaneous tissue containing edema fluid.

View of the tonometer penetrating to the depth of 10 mm with a surface of 78.5 sq. mm (10 mm diameter). Lateral wings with diodes lighting when the indentor reached the depth of 10 mm. At that moment, the applied force is read off from the scale in g/sq. cm.
Tissue fluid pressure measurement
The wick-in-needle technique was used as previously described. 3 Calf and thigh skin were disinfected with isopropyl alcohol. One milliliter of 2% xylocaine with 5 μg/mL adrenaline was injected intradermally and subcutaneously at five points of calf and thigh (Fig. 1). Adrenaline constricted arterioles and small veins, preventing blood leakage at the tip of the wick. An 8 gauge injection needle with a polyethylene tubing (outer diameter 1.34 mm) containing glass-wool wick protruding 5 mm from the tubing tip was introduced under the skin at the depth of 8–10 mm. The needle was withdrawn, whereas the wick-in-tubing remained in situ. A drop of antibiotic ointment was placed at the site of tubing entry to seal off the channel made by the needle. The outer part of the tubing was fixed to the skin by adhesive tape and connected to the pressure transducer (Honeywell, Elblinger, Poland). Recording was done using a three-channel device, pressure range −20 to +150 mmHg (Telsoft, Warsaw, Poland), and LabView software (National Instruments, Austin, TX). Position of the transducer was zeroed placing it exactly at the level of the subcutaneously located wick. The data were collected using Microsoft Excel program and were presented graphically on a pressure/time scale.
Tonometry and tissue fluid pressure measurement under the tonometer
For simultaneous tonometry and “tissue fluid under tonometer pressure” measurement, the indentor was placed exactly above the wick-in-needle introduced under the skin. The tonometer was pushed against the skin penetrating to the depth of 10 mm at five limb levels, and tissue fluid pressure was recorded (Fig. 7a, b).
Limb IPC set at pressures calculated from the formula based on tonometry values
A device with sleeve composed of eight chambers each 9 cm long was used; it was sequentially inflated, inflation pressures were regulated from 50 to 120 mmHg, gradient pressures were decreasing proximally by 20%. Inflation time was 50 s/chamber and total time was 400 seconds. There was no deflation of distal chambers. Deflation time of all chambers at the end of each cycle lasted 50 seconds. The sleeve embraced the whole limb up to the inguinal crease. One compression cycle lasted 1 hour. Pre- and postcompression tonometry was measured at five standard levels.
Statistics
Linear correlation coefficient was calculated for tonometry force against tissue fluid pressure. The double tail student t-test was applied for evaluation of pre- and postcompression tonometry. Data were presented as mean ± standard deviation (SD) and statistical significance at the level p < 0.05.
Results
Tissue fluid pressures under the tonometer indentor
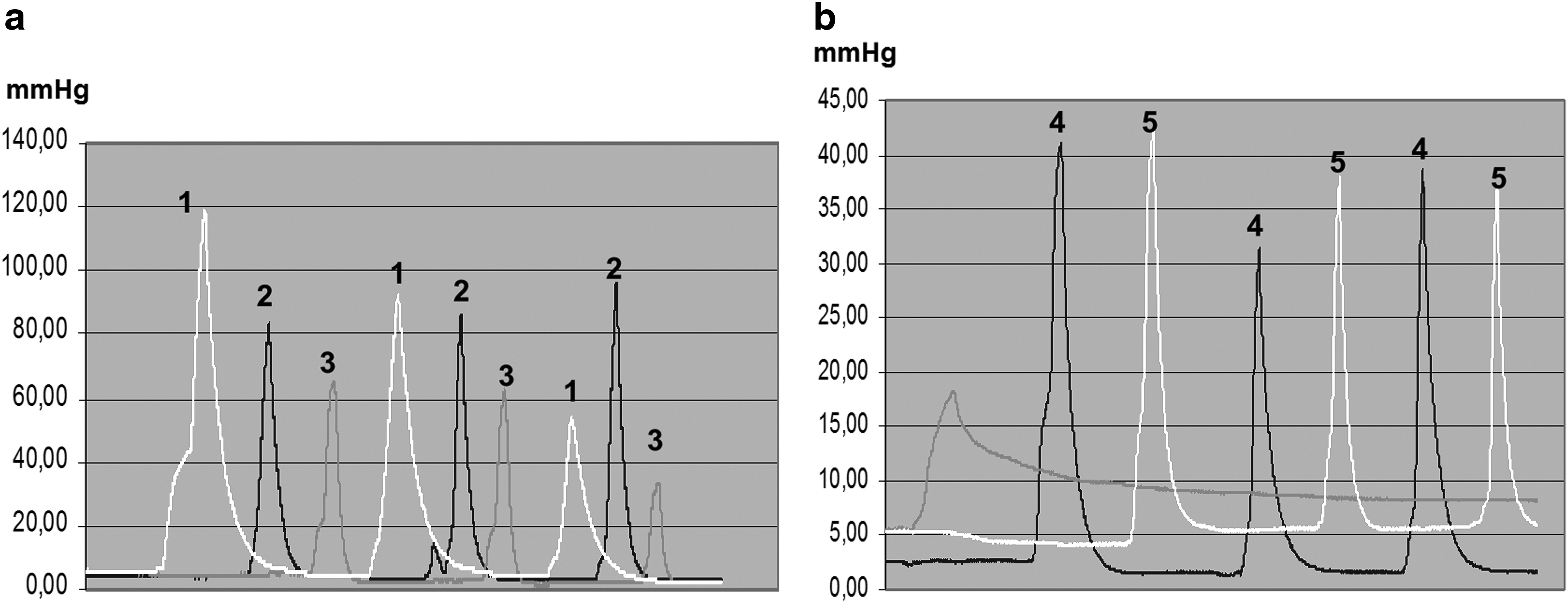
Pressures generated subcutaneously by the tonometer at the depth of 10 mm ranged between 30 and 120 mmHg, depending on the limb level and mass of soft tissue. High pressures were observed in regions with hard fibrotic tissue in the calf (Fig. 8a). They were lower in regions with soft, fatty tissue in the thigh. In these regions, pressures ranged only from 30 to 40 mmHg (Fig. 8b).
Correlation of tonometer force and tissue fluid pressure under tonometer indentor
Tonometry values were plotted against tissue fluid pressures for all lymphedema limb regions. The minimum tissue fluid pressure to move fluid in the limb subcutaneous tissue is 30 mmHg. 3 As has been shown on Figure 9a, in most cases, the applied force of 1000 g/sq. cm did not generate pressures reaching that level. In some cases, even force of 2000 g/sq. cm was not high enough. Pressures >30 mmHg generated by the tonometer pressing with force >1000 g/sq. cm were seen mostly in the thigh. The correlation coefficient for all measurements was 0.71, with few dispersed values originating from regions with very hard skin.

The indentation of 10 mm depth required a different force and generated different tissue pressures at various limb levels (Fig. 9b). The highest force had to be applied in the calf with hard tissues. There were major differences between patients; however, no direct correlation between staging and tonometry results was observed (data not included). Interestingly, tissue fluid pressure calculated per force unit of 1000 g/sq. cm was between 28 and 21 mmHg (Fig. 9b), similar for all levels, with the exception below the knee where fluid moves to the popliteal fossa. Large SD was because of major individual differences.
How to apply tonometer data for setting pneumatic compression pressures at levels generating tissue fluid flow? Calculations
Two parameters should be taken as basics for calculation of effective compression pressures in the compression devices. The first is the tonometer force value. The value necessary for initiation of fluid flow is >30 mmHg. 3 We found that tonometer force of 1000 g (1 kg)/sq. cm generated mean fluid pressures of 25 ± 13 mmHg (Fig. 9b). At sites with hard skin, the penetration of the indentor at 10 mm required 2000–3000 g (2–3 kg)/sq. cm to reach a pressure >30 mmHg. We decided that the number (on tonometer) of kg/sq. cm multiplied by 25 ± 13 mmHg to be used in calculations. The other parameter is the difference between pressures in the inflated chamber and fluid under the chamber. Our measurements revealed that tissue fluid pressures under the inflated compression device chamber in the midcalf and midthigh regions were on average 30 mmHg lower than that in the chamber. 3 Thus, 30 mmHg should then be added to calculations (see the formula hereunder).
Based on the two mentioned main parameters, we propose a formula for setting pneumatic compression pressures at a level guaranteeing tissue (edema) fluid flow.
where Pp is pump pressure in mmHg, T is the tonometer value (number) of kg/sq. cm indenting tissues by 10 mm, 25 + 13 mmHg is the mean tissue fluid pressure under the tonometer indentor/1000 g/sq. cm +1 SD, and C-30 mmHg is the mean pressure loss in tissues during pneumatic compression (difference between the inflated cuff and tissue fluid pressure) caused by tissue stiffness, for example, Pp = 2.0 × 38 + 30 = 106 mmHg in the inflated cuff (predicted tissue fluid pressure only 76 from 106 mmHg minus 30 mmHg tissue force loss).
The usefulness of tonometry for setting pressure levels and evaluation of effectiveness of IPC
Tissue tonometry before and after sequential pneumatic compression of the lymphedematous limb set at tonometer values showed evident softening of tissues in both the calf and thigh (Fig. 10). It also showed that more force was required to soften tissue by evacuation of excess fluid in the calf than in thigh.

Soft tissue tonometry before and after sequential pneumatic compression of lymphedematous lower limb (8 chambers, 120 mmHg, 1 hour, n = 12, mean ± SD, *p < 0.05). Evident softening of tissues both in the calf and in the thigh after compression. Tonometric data confirm the efficiency of compression therapy even when limb circumferences do not change significantly.
Discussion
The study brought the following information: (1) deep tissue tonometry provided data on the pressure generated in the tissue fluid under the tonometer indentor penetrating to the depth of 10 mm., (2) plotting applied force of the tonometer against generated tissue fluid pressures showed that the threshold pressure necessary for mobilization of fluid required a force of at least 1000 g/sq. cm., (3) allowed to work out a formula, based on tonometry values, for setting pneumatic compression pump pressures at levels generating tissue fluid pressures, enabling edema fluid flow, and (4) usefulness of deep tonometry for evaluation of changes in tissue stiffness after pneumatic compression.
We designed and are using a deep tonometer for measuring elasticity deep in tissues where the bulk of edema fluid is accumulated. 4 Various types of tonometers have so far been used. Clodius et al. and Piller and Clodius developed a tonometer with indentation depth depending on gravity and specifically loaded fixed weight. The depth was up to 3 mm deforming only superficial dermis, not reaching deep subcutis containing most fluid.5,6 Chen et al. used a specially designed but similar tissue tonometer in patients treated with multiple lymphaticovenous anastomoses, with a follow-up period of up to 18 months. It gave a quantitative measurement of “softness.” 7 Liu and Olszewski measured skin tonometry after hyperthermic therapy of limb lymphedema. Since the indentations were shallow, the obtained data were not significant, although limb circumferences decreased significantly. 8 Zhang et al. used an ultrasound apparatus to obtain indentation responses of the forearm soft tissues. The effective Young's modulus obtained was found significantly increased with underlying muscles contractions and repeatable. Indentor misalignment and indentation rate sensitivity were found to decrease as the tissue thickness increased. 9 Chen et al. used a skin tonometer and found differences in stiffness after compression therapy. 7 Kar et al. found that tissue tonometry appears to be a sensitive measure for assessing progression of both edema and fibroplasia in patients with peripheral lymphedema associated with filariasis, and, therefore, may be a useful tool to measure the efficacy of drugs commonly used to treat this condition. 10 Bates et al. used an electronic tonometer. 11 Bagheri et al. registered postoperative changes in tissue tonicity after liposuction in the upper arm, but not in the forearm, which also showed significantly higher absolute values. Probably this was caused by the high adipose tissue content with little or no free fluid, thus resembling the normal arm in tonicity. 12 Mayrovitz used a “tissue tester” composed of a force indicator coupled to the penetration depth indicator. Calculated surface contact pressure of the indentor was 93.6 mmHg/100 g of applied force. Indentation forces were recorded in gels and foams to confirm linearity and reproducibility, what is not the case in the heterogeneous limb lymphedema tissues. In clinical testing, the standard indentation test was 4 mm and the applied force in lymphedematous calves was only 420 g. 13
The so far used tonometers were measuring forces at the tonometer–skin interface. The investigators did not take into consideration that edema fluid is located in tissues centimeters deep. There the mobile tissue fluid pressures are lower than those recorded on the skin surface. What should also be underlined is that in using the tonometer, the measure differs between patients and sites of taking measurements, especially when tonometers penetrate only to the depth of 3 mm, which is more or less fibrotic skin thickness. Deeper penetration of the indentor provides data not only from skin but also from the subcutaneous tissue. Figure 8 presents an example of pressure recording in tissue underneath the indentor. Pressure could reach 120 mmHg and also only 40 mmHg depending on the limb region. These recordings clearly show that the effects of therapeutic compression will depend at each limb level on the height of inflated chamber pressures and that tonometry may provide the necessary data for setting inflation pump accordingly.
By measuring tissue fluid pressure under the indentor, we uncovered the so far not described hydromechanic events in the tissue, occurring also during compression. The main observation was that force as high as 1000 g/sq. cm did not generate fluid pressures >30 mmHg necessary for mobilization of edema fluid. In some cases with hard skin, the force of 2–3000 g/sq. cm was used to penetrate the 10 mm depth. In a few regions, fibrotic tissues contained no fluid and high force generated pressures <30 mmHg. In general, more force was needed for the indentor to penetrate the depth of 10 mm in the calf than in the thigh. This can be accounted for by more fibrous tissue in distal parts of limbs. Also higher tissue fluid pressures were observed in the calf than in the thigh. There was large SD of the data most likely brought about by a different degree of advancement of solidification of tissues between individuals, although no correlation with clinical and lymphographic staging was observed. Interestingly, when we calculated how high tissue fluid pressure is generated by a force unit of 1000 g/sq. cm, it turned out to range between 21 and 28 mmHg, irrespective of whether the measurements were made in the hard calf or in soft thigh regions.
Analogy of hydromechanics events occurring under the tonometer and inflated compression chamber was a basis for working out a formula that would allow to set the pump pressures at levels of moving fluid. The tonometry force in g/sq. cm and tissue fluid pressures in mmHg under the indentor, and changes in limb diameter and tissue fluid pressure generated by the inflated chamber were the parameters allowing to construct this formula. This is a rather rough approximation of data from tissue hydraulic events obtained with different methods: in one recording, force and generated fluid pressure under the indentor penetrating 10 mm deep; in another, inflated chamber indenting tissue (decreasing limb diameter) also by 10 mm. Nevertheless, we presume that the obtained data are the closest to the real and the only available using the contemporary measurement methods.
We followed the effects of therapeutic pneumatic compression on tissue elasticity, applying the worked out formula. The pre- and post-IPC recordings showed most decrease of stiffness (or increase in elasticity) in the calf in 100% of patients after one compression cycle. It corroborated previous data from the 3-year follow-up patients. 14
Limitations of the study were large variations in the stiffness (fibrosis) of tissues between patients not correlating with staging, variations in stiffness along the limb axis more expressed in calves than in thighs, and large dispersion of force and tissue fluid pressure data especially in patients at stage III. Nevertheless, our studies have shown, for the first time in the lymphedema literature, the value of tonometry and adjusted pneumatic compression forces on the tissue interstitial fluid pressures and subsequently flow. The so far published articles dealt with forces measured at the skin–tonometer or skin–compression sleeve interface. They did not take into consideration force dissipation in the tissues and recommended low therapeutic pressures, sometimes not reaching deep tissues. The formula proposed by us, although based only on an approximation of the hydromechanic events in the tissues recorded during tonometry and inflated chamber compression, was found to be useful in setting pneumatic compression parameters at rational levels.
Taken together, measuring elasticity using a deep tonometer provided useful data for setting pressures in IPC devices at levels allowing mobilization of edema fluid and its flow.
Footnotes
Acknowledgment
This work was partially supported by the National Science Centre in Poland under grant UMO-2013/11/B/ST8/03589.
Author Disclosure Statement
No competing financial interests exist.