
Abstract
Abstract
Background:
Detection of upper limb lymphedema following treatment for breast cancer typically relies on interlimb circumference-based differences. Normative-determined criteria from an Australian population have high sensitivity and specificity for detection of mild lymphedema in Australian women. It is unknown whether these criteria are applicable to Chinese women whose body habitus is different from Australian women. The aims of this study, therefore, were to determine the normative-based interlimb circumference and volume differences in a Chinese population and whether specific population-based thresholds are required.
Methods and Results:
Arm circumferences at the wrist and at 10 cm intervals proximally to 40 cm were measured on both the dominant and nondominant limb in 484 healthy women, aged ≥20 years. Absolute interlimb differences and interlimb ratios were determined for the circumferences and derived 10 cm volume segments. Analysis of variance determined if the differences varied, depending on location. The absolute interlimb circumference difference from 10 to 30 cm did not vary significantly, enabling determination of a single threshold applicable to all three circumferences. The interlimb ratios varied less, requiring only a threshold for the wrist and one for 10–40 cm and one ratio for interlimb volume segments. The interlimb thresholds determined in the Chinese population were within 2 mm to that reported in the Australian study.
Conclusions:
Even though the habitus of Chinese women living in China differed to the women living in Australia, similar normative-based thresholds for the detection of lymphedema were identified.
Introduction
L
Detection of lymphedema within a limb is commonly determined from interlimb circumference differences. 3 Each limb is measured at standardized locations along the limb and the interlimb difference determined. 4 Alternatively, the circumference measurements are used to approximate limb volume and similarly, the interlimb absolute and relative differences determined. 4 The interlimb difference is compared to a threshold, over which it is considered that lymphedema is present.4,5 The commonly used interlimb circumference difference for the arms is 2 cm, regardless of whether the dominant or nondominant limb or location along the limb is affected, whereas the commonly used interlimb volume difference is 10% or 200 mL. 3 A recent proposal is to use normative-based thresholds that account for location and limb dominance, 6 as these were superior to the commonly used ones for detection of mild lymphedema when compared to a strong reference standard. 5 However, as the normative-based thresholds were based on an Australian population, 6 it is unknown whether these values are generalizable to other populations.
To date, it is presumed that thresholds for detection of lymphedema are generalizable, regardless of body habitus. For example, 2 cm interlimb differences has been used as a threshold for the detection of lymphedema following treatment for breast cancer for studies conducted in Australia, 7 United States,8–11 Italy, 12 Brazil, 13 Turkey, 14 and South Korea 15 among others. As the body habitus is different between populations,16–18 it is important to clarify whether the normative-based thresholds for the detection of lymphedema are appropriate for other populations, for example, Chinese population.
The aim of the current study was to determine (i) what are the normative-based interlimb circumference and volume differences in a Chinese population; (ii) the impact which age and body weight has on the interlimb difference; (iii) to determine population-specific thresholds for Chinese women; and (iv) whether specific population-based thresholds are required.
Methods
Participants
The participants were healthy women recruited from a variety of community settings in both urban and regional areas in Shanghai, China. To be included, women had to be over 20 years of age with no self-reported history of breast cancer or lymphedema. We excluded women if they had experienced any recent upper limb injury that may have affected their upper limb or ability to position their limbs for testing, or were pregnant.
We purposely recruited women to ensure sufficient cases for each of the five age groups of interest. Overall, 484 women met our criteria, with 55 aged 20–39 years; 79 aged 40 to 54 years; 203 aged 55 to 64 years; 125 aged 65 to 74 years; and 22 aged 75 years or older, providing sufficient cases for describing normative data. 1 Participant characteristics are reported in Table 1. The participants' ages ranged from 20 to 84 years; the average (standard deviation [SD]) age was 57.2 (13.0) years. Body mass index (BMI) ranged from 13.5 to 36.9 kg/m2 with the 65–74-year age group showing the largest average BMI. Overall, eight women reported that they were left-hand dominant.
Mean (standard deviation) shown.
BMI, body mass index.
All participants gave written informed consent before participation in the study. The study was approved by the Huashan Hospital Ethics Committee in Shanghai, China.
Protocol
All participants attended a single session, at which their height, weight, and arm circumferences were measured. Height was determined using a stadiometer and weight using an analog scale; BMI was calculated from these measurements.
Arm circumferences measurements were undertaken as previously described. 4 Women were positioned in sitting at a table with the extended pronated arm resting at 90° of forward flexion on a measuring grid. Arm measurements were undertaken using a retractable Jobst nonstretch soft tape measure commencing at the midpoint of the ulnar styloid set as the “0 cm” mark and then at 10 cm intervals up to 40 cm proximal to the ulnar styloid. Trained research assistants, who had physiotherapy backgrounds, completed all the measurements.
Segmental limb volumes were derived from adjacent arm circumference measurements using the truncated cone formula
4
:
where V is the volume of the segment, C1 and C2 are the circumferences at each end of the segment, and h is the distance between the two circumferences, that is, 10 cm. The arm segments were designated as follows: the ulnar styloid to 10 cm was Segment A (Seg A), 10 to 20 cm was Segment B (Seg B), 20 to 30 cm was Segment C (Seg C), and 30 to 40 cm was Segment D (Seg D). Segment D was not available for two participants due to insufficient limb length. The limb volume segments were summed to determine the total limb volume.
Data analysis
All data are presented as mean ± SD for the dominant and nondominant arm separately for each circumference measurement location and limb segments. Interlimb differences were expressed as mean (95% confidence intervals [CI]). Multivariable analysis of variance (ANOVA) determined whether limb and location along the limb affected the circumference or volume measurement. Duncan's post hoc tests identified where significant differences occurred.
The absolute and relative interlimb differences for the circumference and volume measurements for each location along the limb were calculated. The absolute differences were determined by subtraction of the limb circumference or volume from that of the respective circumference or volume of the other limb, whereas the relative difference was determined by expressing the circumference or volume of one limb as a ratio of that from the respective volume or circumference of the other limb. The interlimb difference was tested for outliers using Tukey “far out” test. Univariate ANOVA determined whether the absolute and relative differences differed, depending on location. When differences were identified, Duncan's post hoc analysis was used to determine where the differences occurred. Regression analysis was undertaken to determine if age, height, or BMI were related to the interlimb differences in circumference or volume.
Finally, the thresholds for classifying women as to whether or not they likely had lymphedema were determined for circumference and volume measurements for both the right and left limb. These thresholds were established using the previously reported approach, in which the diagnostic cutoff is set at the mean plus two and three times the SDs, thereby, encompassing >95% of the population.7,8 Data were analyzed using SPSS for Windows (version 22, IBM) and Microsoft Excel (2013).
Result
Effect of limb dominance and location along the limb
The limb circumferences of the dominant limb were significantly larger than the comparable measurement of the nondominant limb and increased significantly from the wrist to the 40 cm measurement location (Table 2; Limb: F1,4796 = 9.2, p = 0.002; Location: F4,4796 = 4820.3, p < 0.001). There was not, however, an interaction effect between limb and location. Duncan's post hoc analysis revealed that the five circumference locations differed significantly from each other. Similarly, limb volumes were larger on the dominant side than the nondominant side and increased along the length of the limb measures (Table 2; Limb: F1,3840 = 6.6, p = 0.01; Location: F3,3840 = 2598.2, p < 0.001) with no interaction identified. Duncan's post hoc analysis revealed that segmental volumes of each location differed significantly to each of the others.
Circumference measures commence at the wrist and proceed by 10 cm proximally to 40 cm. Volume measures derived for 10 cm segments, commencing at the wrist (Seg A) and proceeding by 10 cm to Seg D (30–40 cm proximal to the wrist).
Whole limb, that is, 0–40 cm.
IQR, interquartile range; SD, standard deviation; segment; Seg A Segment A, wrist to 10 cm proximal to the wrist; Seg B Segment B, 10–20 cm proximal to the wrist; Seg C Segment C, 20–30 proximal to the wrist; Seg D segment D, 30–40 cm proximal to the wrist.
Absolute and relative differences
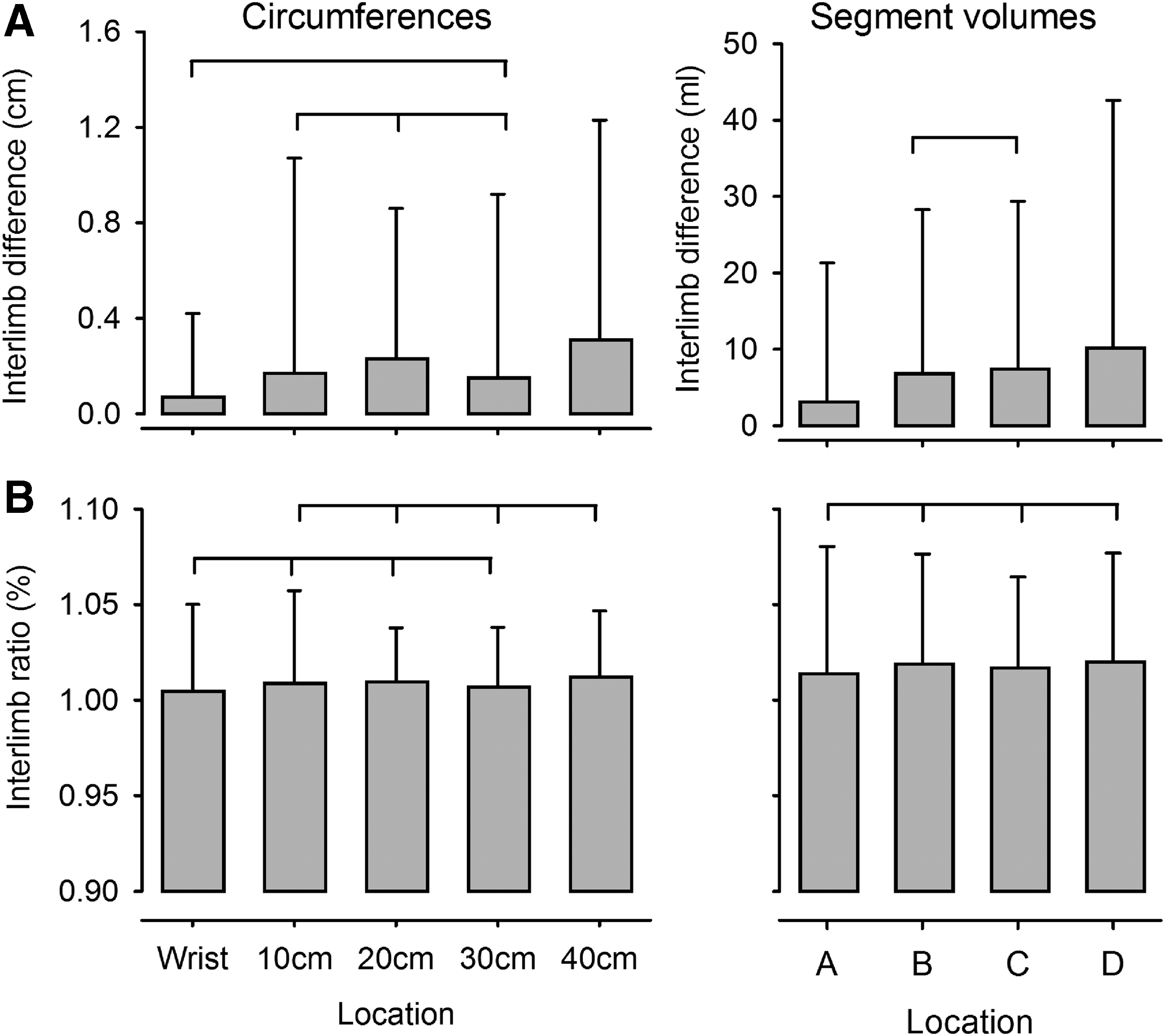
The absolute interlimb differences were screened for outliers, resulting in eight cases removed. The absolute mean interlimb differences in circumferences were significantly different, ranging from 0.06 cm (95% CI: 0.03–0.10 cm) at the wrist to 0.32 cm (95% CI: 0.23–0.41 cm) 40 cm proximal to the wrist (Table 3). Post hoc analysis revealed no significant differences among the 10, 20, and 30 cm interlimb absolute differences as well as no difference between the wrist and 30 cm interlimb absolute difference (Fig. 1).
Absolute
Panel A is based on absolute differences, in which the measurement from one limb is subtracted from the respective measurement of the other limb. Panel B is based on relative differences, in which the measurement from one limb is expressed as a ratio to the corresponding measurement from the other limb. The thresholds are calculated by summating the mean with either two (2SD) or three (3SD) times the standard deviation.
proximal to the wrist.
Whole limb, that is, 0–40 cm.
Seg A, wrist to 10 cm; Seg B and C, 10–30 cm proximal to the wrist; Seg D, 30–40 cm proximal to the wrist; 2SD = mean + (2 × SD); 3SD = mean + (3 × SD); LE, lymphedema.
The absolute interlimb volume differences among the segments differed, with the least mean difference in volume identified in Seg A (3.1 mL; 95% CI: 1.6–4.7 mL) and the greatest mean difference identified in Seg D (10.2 mL; 95% CI: 7.4–13.0 mL). Post hoc analysis revealed that the interlimb volume difference was not significantly different between Seg B and Seg C and between Seg C and Seg D (Fig. 1).
The mean interlimb circumference ratios (relative differences) differed significantly along the limb, ranging from 1.005 (95% CI: 1.001–1.009) at the wrist to 1.012 (95% CI: 1.009–1.015) at the 40 cm location. Post hoc analysis revealed that the wrist was significantly different to the 40 cm measure but not to the other circumference measurements, and similarly, the 40 cm measure was significantly different to the wrist but not to the other circumference measurements. Volume ratios were not significantly different along the length of the arm, ranging from 1.013 (95% CI: 1.008–1.020) to 1.020 (95% CI: 1.015–1.025; Fig. 1).
Effect of age and bodyweight on interlimb difference
Age, bodyweight, and BMI did not affect interlimb absolute differences in circumferences or volume, after accounting for location along the limb.
Determination of thresholds for detection of lymphedema
For both the dominant and nondominant limb, the calculated cutoffs were defined at two or three SDs above the mean difference between the limbs.6,19,20 Where there were no significant differences between the absolute or relative interlimb differences, data were collapsed to a single threshold. For example, as there were no significant differences between the interlimb circumference differences at 10, 20, and 30 cm, these were collapsed for a single cutoff point. The calculated 2SD cutoffs for the dominant arm, commencing at the ulnar styloid and moving proximally, were 0.7 cm at the wrist, 1.8 cm for 10 to 30 cm, and 2.3 cm for 40 cm proximal to the wrist; in contrast, the 2SD cutoffs for the nondominant arm were 0.6, 1.4, and 1.6 cm, respectively. The thresholds for the right and left limb absolute and relative thresholds for circumference and volume measurements are shown in Table 3.
Discussion
Detection of mild lymphedema following treatment of breast cancer is challenging, particularly in cases where there are no presurgery measurements. Clinically, detection is commonly based on surpassing a predetermined threshold. Previous research, conducted in Australia, first determined interlimb thresholds based on an Australian population, 6 and second, established that these thresholds had higher sensitivity and specificity in detection of mild lymphedema than commonly used thresholds. 5 The current study evaluated the generalizability of normative-based thresholds derived from an Australian population to a Chinese population. Not surprisingly, and similar to the Australian study, the interlimb absolute differences varied according to the location along the limb as well as whether the limb was dominant or nondominant. In contrast, the segmental volume ratios did not vary along the limb and may provide a simplified approach to detection of lymphedema.
The current study was undertaken to ascertain whether the validated thresholds identified by Dylke et al. 6 in an Australia-based study were applicable to Chinese women. Comparison of the anthropometric data revealed that the Chinese women were shorter and weighed less than the Australian cohort. The mean BMI of the Australian women was in the “overweight” range whereas that of the Chinese women was in the “normal” range. Consequently, the upper limb circumferences in the Australian cohort were larger than the Chinese cohort. For example, the Australian cohort's mean circumferences for the dominant limb were larger by 2.4 at 20 cm proximal to the wrist; and 5.4 at 40 cm proximal to the wrist compared with the Chinese cohorts comparable means.
Although the limb circumferences differed between the Australian and Chinese population, the absolute interlimb differences between the Chinese and Australian cohorts were similar (Fig. 2). Notably, the 2SD single interlimb circumference thresholds for the Chinese cohort were within 2 mm for the 2SD thresholds determined from the Australian cohort, and within normal measurement error. 21 However, the current study simplified the thresholds. In the current study, analysis revealed that interlimb circumference differences did not differ significantly at the 10, 20, and 30 cm locations, and those for interlimb volume differences were not significantly different between Seg B and Seg C. As a consequence, only a single threshold is needed for the range over which there was not a significant difference.

Dominant arm thresholds for detection of lymphedema based on interlimb circumference differences exceeding 2SD above the mean for Chinese (filled) and Australian (open) women. SD, standard deviation.
Interlimb ratios are also used to ascertain whether an individual presents with lymphedema. Typically, a threshold of 10% interlimb differences are used. 3 While this ratio has good specificity, it had poor sensitivity for detection of mild cases of lymphedema. 5 In other words, a person over the threshold of 10% interlimb volume difference likely has lymphedema; however, a negative result does not enable confirmation that the person does not have the disease. In the current cohort, the 2SD threshold for the interlimb whole arm ratio was 11% for the dominant side but 7% for the nondominant arm. Confirmation of these thresholds against a reference standard is required.
Slight differences in absolute circumference thresholds were found between the Chinese and Australian cohort. These differences may be explained, in part, due to measurement error. In the Chinese study, a narrow nonelastic tape measure was used, and the study employed five assistants to collect data. Although all assistants underwent training, there may be an issue related to interrater reliability. In contrast, in the Australian study, a single measurer, using a perometer, collected the data. While there is high concordance between perometry and tape-measure-based measurements, there is a 5% bias in favor of perometry, 4 indicating they are not identical. The other difference was in relation to limb dominance. In the Australian study, 6% self-reported that their dominant limb was their left limb; in contrast, less than 1% of the Chinese cohort self-reported that their left hand was their dominant limb. This may reflect a cultural effect, in which everyone was required to write with the right hand; in future, rather than asking for limb dominance, it may be better to ask which hand they are asked to do a particular task such as using chopsticks.
The current study provides guidance on determining the presence of lymphedema in a Chinese population, for which there is no presurgical data available. One of the issues, however, is that normatively determined “absolute” thresholds will not identify all patients. Change in circumference from a baseline measure allows better identification of cases of lymphedema. 22 The limitation of absolute diagnostic thresholds for detection of lymphedema was recognized in development of criteria using bioimpedance spectroscopy. 23 In addition to presenting absolute thresholds, a change score was also identified, based on three times the SD. For BIS, this was equivalent to a change in interlimb ratio of 0.10. Adoption of both criteria does identify additional cases of lymphedema. 24 This approach may also be appropriate for circumference-based measures. For example, in the current study, two times the SD of the difference at 10–30 cm is equivalent to a change score of 1.6 cm, regardless of the initial difference. Prospective studies in both Australian and Chinese cohorts are required to determine the utility of this approach.
Conclusion
In conclusion, although Chinese women were shorter and weighed less than an Australian cohort, the interlimb differences were similar, with similar thresholds. However, the current study provides a simpler approach for detection of mild lymphedema, taking into account the lack of difference between some measures. These revised thresholds are likely appropriate for detection of lymphedema for western and eastern women.
Footnotes
Acknowledgment
We acknowledge the assistance provided by Na Xie, Junyu Chen in data collection.
Author Disclosure Statement
No competing financial interests exist.