
Abstract
Abstract
Background:
Lymphedema of limbs affects a large mass of tissues. Pathological changes develop in skin and subcutaneous tissue. Bacterial retention in edema fluid is followed by chronic inflammatory reaction. The question arises whether the chronic processes affecting a large mass of limb tissues are reflected in the serum by appearance of specific proteins accumulating and subsequently absorbed from the lymphedematous tissues
Aim:
To measure the concentration of serum proteins (1) participating in cellular disintegration such as caspase 1, sFas, high-mobility group box 1 (HMGB1), and serpin, (2) cell growth regulating factors such as cortisol, human growth hormone, keratinocyte growth factor, and insulin-like growth factor (IGF), and (3) angiogenic and growth factors such as angiopoetins 1 and 2, adiponectin, leptin, and transforming growth factor beta.
Results:
We found (1) increased concentration of serum caspase 1, sFas, serpin, and HMGB1 accounting for cellular destruction, (2) raised levels of cortisol and IGF, confirming active cellular processes, and (3) elevated concentrations of angiopoetin 1, adiponectin, and leptin, indicating proliferation of adipose tissue.
Conclusions:
Proteins appearing in serum in high concentrations in patients with lymphedema without systemic clinical and biochemical signs of inflammation indicate that multiple processes of destruction and rebuilding proceed in the lymphedematous tissues. Measuring concentration of caspase 1, sFas, serpin, HMGB1 protein, adiponectin, and leptin give insight into these processes. Lymphedema should be considered as tissue process characterized not only by increase in mobile tissue fluid volume but also tissue restructuring. Compression and drainage therapy should be complemented by anti-inflammatory medication.
Introduction
O
The question arises whether these chronic processes affecting a large mass of limb tissues can be reflected in the serum by appearance of specific proteins accumulating and released to circulation from the lymphedematous tissues. Although nonspecific, their increased concentration may be a hint on presence of an active tissue process in the lymphedematous limbs. An analogy can be drawn between myocardial infarction and troponin released to the serum.
Direct analysis of tissue fluid/lymph proteins collected from swollen tissues would have given a better insight into the physiological as well pathological changes in tissues.4–9 However, in advanced stages of lymphedema with excess hypertrophied fibroblasts and adipocytes, there is scanty mobile fluid and its volumes are not sufficient for clinical biochemical evaluation. This prompted us to carry out studies on serum concentration of three groups of proteins (1) participating in cellular disintegration such as caspase 1, high-mobility group box 1 (HMGB1), fas CD95 L, and serpin, (2) cell growth factors (GFs) such as cortisol, human growth factor (HGF), keratinocyte growth factor (KGF), and insulin-like growth factor (IGF), and (3) angiogenic and GFs such as angiopoetins 1 and 2, adiponectin, leptin, and transforming growth factor beta (TGF-β). Increased levels of these proteins would reflect the intensity of local processes in the lymphedematous tissues and prompt to control the inflammatory reaction. Studies were carried out in a group of patients with lower limb lymphedema, displaying predilection to infections with evidence of mutations of TLR2 and TLR4 hetero I homozygotes. 10
Patients
One hundred patients aged 21–62 (median 44) years were consecutively admitted to our Department of Surgery during the period 2011–2016, in an order as they were showing up, because of inflammatory processes of soft tissues in lymphedematous lower limbs stages II to IV of >3 years duration. There were 55 females and 45 males. Their body mass index (BMI) was <26 kg/m2. They underwent screening for identification of lymphatic obstruction. The initial etiology of lymphedema was soft bacterial tissue inflammation in calf or foot with a latent period of months or years of no edema. Edema appeared either spontaneously or after a minor trauma.
Inclusion criteria
Inclusion criteria were lower limbs swelling after foot or calf dermatitis with at least three episodes of acute DLA and recent in the past 12 months, lymphographic confirmation of lymphatic collectors' obstruction. Additional qualifications to the study were genetically proved predilections to inflammatory responses because of mutations of TLR2 and TLR4 hetero I homozygotes. 10
Biochemical evaluation for exclusion of actual acute systemic inflammatory or metabolic processes
The serum levels of CRP were 2.7 ± 1.8 ng/mL, insulin 46 ± 39 pmol/L, TSH 1.8 ± 1.1, T3 3.0 ± 0.7, T4 1.5 ± 0.3, and transferrin 239 ± 37 mg%, all in a normal range.
Exclusion criteria
Venous thrombosis on ultrasound investigation, previous limb trauma, cancer surgery, and/or radiotherapy afflicting limbs, cardiac insufficiency, lipedema, and diabetes.
The study protocol was approved by the Institute's ethics committee. Informed consent was obtained from patients.
Diagnosis of lymphedema
Clinical evaluation
In brief, level of edema embracing limb from foot to groin and degree of skin keratosis and fibrosis. In stage II, pitting edema affected foot and lower half of the calf, in stage III, foot and calf were involved, with hard foot and ankle area skin, in stage IV, the whole limb was edematous with foot and calf skin hyperkeratosis and papillomatosis of toes. 11
Lymphoscintigraphic evaluation
The evaluation of main lymphatic pathways was done on lymphoscintigraphic pictures. The 99 mTc Nanocoll was injected into toeweb and sole and imaging was done 10 and 60 minutes later after standard walking at 3 km/h. In stage II, delayed outline of calf lymphatics and small inguinal node appeared 30 minutes after injection. In stage III, small fragments of draining lymphatics were seen in the calf and thigh with a few inguinal nodes of irregular outline after 1–2 hours of walking. Stage IV was characterized by epifascial spread of tracer in the foot and entire calf without observation of collecting lymphatics and nodes. In none of the investigated patients did the tracer pass on the affected side above the inguinal crease level. 12
Fluorescent lymphography evaluation
The evaluation of superficial foot and calf lymphatic pathways with indocyanine green lymphography confirmed lymph stasis at the subepidermal level. Combination of isotopic and fluorescent lymphographies provided evidence for obstruction of the superficial and deep anatomical lymphatic systems and formation of collateral subepidermal lymph flow pathway, necessary for diagnosis of lymphedema in contrast to other types of limb edema.
Blood collection for serum
Blood samples were collected in all patients between 3 and 5 pm at least 4 hours after the last meal. Ten milliliters of blood was withdrawn from the cubital vein, clotted, spun down, and serum frozen at −20°C for further studies.
Measurement of serum protein concentration
The investigated proteins were divided into three groups. Group 1: proteins released from tissues undergoing inflammatory reaction, Group 2: hormones participating in tissue reconstruction, and Group 3: proteins participating in adipose and fibrous tissue growth. The R&D systems (Minneapolis) immunoassay test was applied according to the manufacturer's instructions. The investigated proteins are given in Table 1.
Statistical evaluation
The protein concentration data from lymphedema patients were compared with those obtained from our studies in normal subjects (15–30), standard values cited by the manufacturer, and also with those contained in the WHO Consultation on Global Measurement Standards and their use in the in vitro Biological Diagnostic Field and pertinent literature. Mean standard values were calculated. Student t-test with difference significance at p < 0.05 was used.
Results
Group 1: proteins released from tissues with inflammatory reaction.
Serum caspase 1 level was increased approximately twice compared with normal (Fig. 1), whereas soluble proapoptotic Fas/CD95 was 10 times higher (Fig. 1). The level of serin protease inhibitor serpin was found twice more than the normal values. In 22% of patients, it was higher over mean and 1 standard deviation. HMGB1 playing a role in autophagy and the autophagic clearance of dysfunctional mitochondria reached levels twice as high as in normal serum (Fig. 1). In 22% of patients, it was higher over mean and 2 standard deviations.
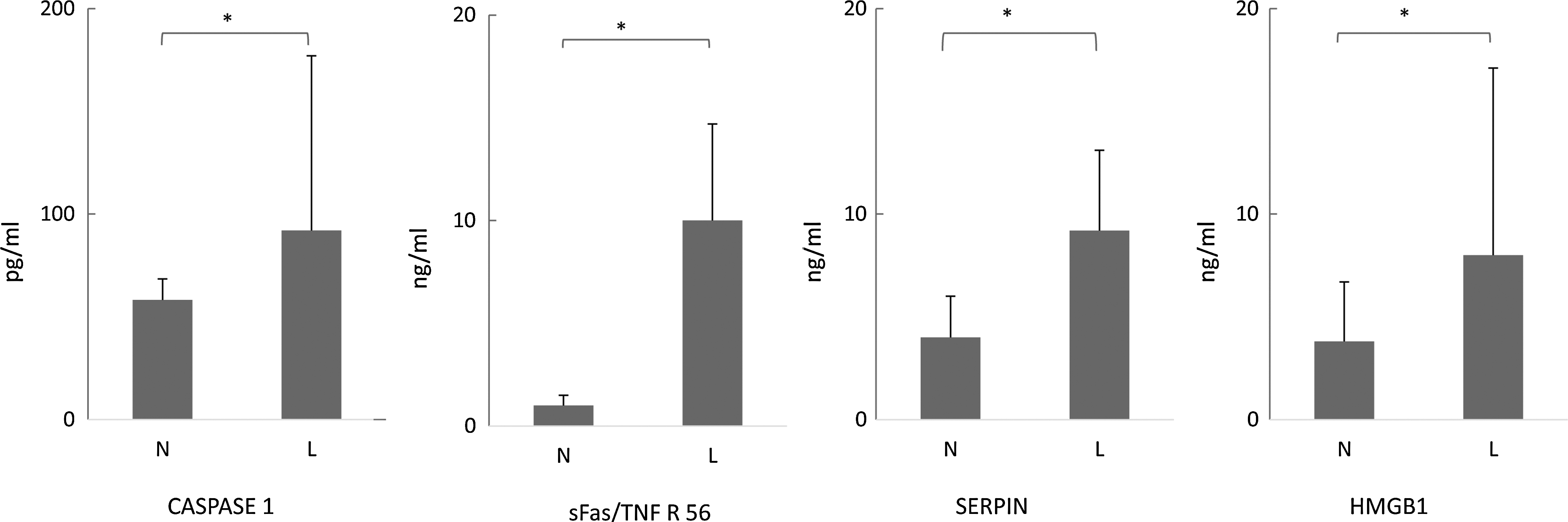
Proteins participating in cellular disintegration: caspase 1, HMGB1, fas CD95 L. HMGB1, high mobility group box 1. *p < 0.05.
Group 2: hormones regulating tissue reconstruction.
Serum cortisol level was slightly elevated, whereas the insulin-like GF level was four times higher (Fig. 2). In 12% of patients, the values exceeded mean by 1 standard deviation. The values of HGF and KGF remained within normal limits (Fig. 2).

Cell growth factors: cortisol, HGF, KGF, IGF. HGF, human growth factor; IGF, insulin-like growth factor; KGF, keratinocyte growth factor. *p < 0.05.
Group 3: hormones participating in fibrous and adipose tissue growth.
Angiopoetin 1 level was increased by a factor of 2, and in 14% of cases it exceeded mean and 1 standard deviation. Adiponectin level was twice as high as normal (Fig. 3). In 14% of cases, it exceeded mean by 1 standard deviation. Leptin levels were also increased by a factor of 2 and in 18% it exceeded 1 standard deviation. The values of angiopoetin 2 and TGF β were in normal limits (Fig. 3).

Angiogenic and growth factors: angiopoetins 1 and 2, adiponectin, leptin, and TGF-β. TGF-β, transforming growth factor beta. *p < 0.05.
Discussion
This study has provided the following results: (1) increased concentration of serum caspase 1, sFas, serpin, and HMGB1 proteins accounting for cellular apoptosis, (2) raised levels of cortisol and IGF, confirming active cellular processes, and (3) elevated concentrations of angiopoetin 1, adiponectin, and leptin but not of TGF-β, indicating proliferation of adipose tissue. Elevation concentrations of these proteins were found in patients who did not reveal any signs of acute systemic inflammatory reaction. This means that the reconstructive proliferative processes in the lymphedematous tissues proceed locally in an autonomous manner. However, some regulatory proteins contained in tissue in excess may have reached circulation and were detected. Although nonspecific, their increased concentration may be a hint on the advancement of tissue processes in the lymphedematous limbs. An analogy can be drawn between myocardial infarction and troponin absorbed to the serum. Interestingly, high standard deviations were observed for most proteins. This was because of very high values in ∼20% of patients, indicating that the processes proceed although at various intensities.
Of primary interest remains the source of excess proteins detected in patients' serum. In general, proteins are synthesized and produced in the liver and lymphoid organs. However, quite a large volume can originate from local nonlymphoid tissues and immune infiltrating cells. Our previous studies have shown generally higher concentrations of cytokines, and GFs and enzymes in lymph than in serum, both under normal conditions and in lymphedema.5–9 This indicates that, in addition to proteins filtered from blood, local cells contribute to lymph concentration by their own production, depending on the actual cell requirement. This suggests existence of a local autonomous regulatory humoral mechanism in tissues, not reflected in serum. The proinflammatory cytokine levels had the lymph/serum (L/S) ratios higher and the anti-inflammatory lower than in serum. The L/S ratio was also high for chemokines and tissue protease inhibitors but low for metalloprotease 9. The values for GFs were high except for interferon (IFN)-gamma. The L/S ratio for angiogenic factors and leptin was >1, but low for adiponectin. Since obtaining large volumes of lymph from lymphedematous limbs is impossible, especially in advanced stages of the disease, we decided to rely on serum samples, however, focusing upon selected proteins that participate in the process of rebuilding of tissues with lymph stasis. Hereunder we briefly point to the possible function of investigated proteins in lymphedematous tissues.
Caspase 1/interleukin (IL)-1 converting enzyme (ICE) is an evolutionarily conserved enzyme that proteolytically cleaves other proteins, such as the precursors of the inflammatory cytokines IL-1β and IL-18. It plays a central role in cell immunity as an inflammatory response initiator. The two inflammatory cytokines activated by caspase 1 are excreted from the cell to further induce the inflammatory response in neighboring cells.13,14 The concentrations of caspase 1 differ in the normal population between individuals from 0 to >200 pg/mL as the subclinical inflammatory processes are not recognized by the individuals. In the highly selected well-diagnosed group of normal subjects, the values remain around 60 pg/mL. 15 In our lymphedema group, high levels reaching 170 pg/mL were observed and in 20% of cases they exceeded mean by 1 standard deviation.
Fas ligand (FasL or CD95 L) is a type-II transmembrane protein that belongs to the tumor necrosis factor (TNF) family. Its binding with its receptor induces apoptosis. Fas ligand–receptor interactions play an important role in the regulation of the immune system. Fas forms the death-inducing signaling complex upon ligand binding. Fas-induced apoptosis and the perforin pathway are the two main mechanisms by which cytotoxic T lymphocytes induce cell death in cells expressing foreign antigens. Apoptosis pictures are seen in the lymphocyte infiltrates and lymph nodes in the lymphedematous tissues. 16 sFas serum levels in our patients reached high values. This may reflect apoptotic processes in lymphedematous tissues.
Serpins are a superfamily of proteins with similar structures that were identified for their protease inhibition activity. The acronym serpin was originally coined because the first serpins to be identified act on chymotrypsin-like serine proteases (serine protease inhibitors). Protease inhibition by serpins controls coagulation and inflammation. Its high levels point to a chronic inflammatory process in tissues. 17 Our data on increased levels of serpin confirm it.
HMGB1 is among the most important chromatin proteins in the nucleus. HMGB1 interacts with nucleosomes, transcription factors, and histones. It is secreted by immune cells (such as macrophages, monocytes, and dendritic cells) through leaderless secretory pathway. Activated macrophages and monocytes secrete HMGB1 as a cytokine mediator of inflammation. Antibodies that neutralize HMGB1 confer protection against damage and tissue injury during ischemia, sepsis, and endotoxemia. 18 We found highly increased levels of HMGB1 in serum of most patients, and in 20% of patients they exceeded mean by 1 standard deviation. High levels of this protein may be the result of destruction of cellular nuclei in the local cytotoxic processes.
Cortisol functions to suppress the immune system response. Cortisol prevents the release of substances in the body that cause inflammation. It inhibits production of IL-12, IFN-γ, IFN-α, and TNF-α by antigen-presenting cells and T helper (Th1) cells, but upregulates IL-4, IL-10, and IL-13 by Th2 cells. The activation of the stress system (and resulting increase in cortisol and Th2 shift) seen during an infection is believed to be a protective mechanism that prevents an overactivation of the inflammatory response. 19 This is how we try to interpret the increased concentrations of cortisol in our group of patients. Since all patients had blood samples taken in the afternoon during down of the cortisol diurnal curve, its high levels pointed to an active immune reaction.
Human growth hormone (hGH), also known as somatotropin is a peptide hormone that stimulates growth, cell reproduction, and cell regeneration in humans. It is thus important in human development. It is a type of mitogen that is specific only to certain kinds of cells. 20 Stimulates the immune system growth hormone (GH) levels are low, usually <5 ng/mL for most of the day and night. In our studied group, the mean values were 6.5 ng/mL.
KGF, also known as FGF7, is a GF present in the epithelialization phase of wound healing. In this phase, keratinocytes are covering the wound, forming the epithelium. KGF binds to fibroblast growth factor receptor 2b (FGFR2b). In lymphedema, hyperkeratosis is the typical consequence of lymph stasis. In an indirect way, KGF also stimulates fibroblasts proliferation.21,22 We did not observe increased serum levels of KGF. It is possible this GF is most active in a paracrine manner and inactivated in serum.
IGF-1 generated in the liver is the anabolic effector and linear growth promoting hormone of the pituitary GH. IGF-1 acts on the proliferative cells. IGF-1 also induces organ and tissue growth. We noticed a four times increase in IGF-1 level. 23 The exact molecular process regulated in the lymphedematous tissues remains unknown.
Angiopoietin is part of a family of vascular GFs that play a role in embryonic and postnatal angiogenesis. Angiopoietin signaling most directly corresponds with angiogenesis, the process by which new arteries and veins form from preexisting blood vessels. Angiogenesis proceeds through sprouting, endothelial cell migration, proliferation, and vessel destabilization and stabilization. Interestingly, angiopoietin levels provide an indication for sepsis. Research on angiopoietin 2 has shown that it is involved in the onset of septic shock. The combination of fever and high levels of angiopoietin 2 is correlated with a greater prospect of the development of septic shock. 24 In the lymphedematous tissues, angiopoetin may participate in angiogenesis of adipose tissue. We observed evidently increased levels of angiopoetin 1 but not angiopoetin 2.
Adiponectin is a protein exclusively secreted from adipose tissue, mainly subcutaneous, into the bloodstream and is very abundant in plasma relative to many hormones. Adiponectin is secreted into the bloodstream where it accounts for ∼0.01% of all plasma protein. Adiponectin displays no great fluctuations in the bloodstream, which means that its release is not acute but regulated by long-term metabolic changes. 25 Adiponectin levels were evidently higher in our group of patients than in average controls.
Leptin is involved in the regulation of the inflammatory response. It has been further theorized that leptin's role as an inflammatory marker is to respond specifically to adipose-derived inflammatory cytokines. In terms of both structure and function, leptin resembles IL-6. 26 Growth of adipose tissue in the lymphedematous limbs is a well-known phenomenon. The mechanisms by which postoperative lymphedema develops in obese patients and the mechanisms by which leptin regulates lymphatic endothelial cell homeostasis such as tube formation and cell proliferation remain unknown. 27 High levels of serum leptin in our group of patients would fit to the pathomechanism of fat deposition. It is worth underlining that our patients remained in the normal BMI group.
TGF-β acts as an antiproliferative factor in normal epithelial cells and at early stages of oncogenesis. It is secreted by many cell types, including macrophages. TGF-β appears to block the activation of lymphocytes and monocyte-derived phagocytes. 28 Interestingly, the TGF-β serum levels remained low in our group of patients. This may be accounted for by its binding by fibroblasts.
Limitations of this study may be a low number of investigated patients, difficulties in detection of transient subclinical inflammatory processes in the group of apparently normal control subjects, variations in the standard values of many types of proteins depending on the detection methods, enzymatic disintegration of specific short-life regulatory proteins, and diurnal variations in concentration of various proteins. To avoid the inaccuracies, we strictly selected a group of patients without overt acute inflammatory biochemical changes, included only those who revealed presence of TLR mutations and dermatolymphangioadenitis in the past, and collected serum samples at the same time of the day.
Taken together, proteins appearing in serum in high concentrations in patients without systemic clinical and biochemical signs of inflammation indicate that in the lymphedematous tissues, multiple processes of destruction and rebuilding proceed. Measuring concentration of caspase 1, sFas, serpin, HMGB1 protein, adiponectin, and leptin gives an insight into these processes. Lymphedema should be considered as tissue process characterized by not only increase in mobile tissue fluid volume but also tissue restructuring. Compression and drainage therapy should be complemented by anti-inflammatory medication.
Footnotes
Acknowledgment
This work was supported by project number NN404 0851 40 funded by National Science Center, Poland.
Author Disclosure Statement
The authors declare no conflict of interest.