
Abstract
Abstract
Objective:
Describe inpatient resource utilization trends in children with lymphatic malformations using a national database.
Data source:
Kids' inpatient database, years 2000–2009.
Methods:
Subjects included children 18 years and under with International Classification of Diseases (ICD), 9th revision code: 228.1–lymphangioma, any site. Data elements were extracted and used to calculate related inpatient costs and trended over time.
Results:
No significant increase in admission rates was noted over time, p = 0.5128. Average total charges per admission were $30,995. There is a clear and increasing trend of total charges per admission; even when adjusted for inflation, this has increased disproportionately. In 2009, the mortality rate increased to 2.58%, which was significantly higher than in previous years, p = 0.0346. In multivariate analysis for mortality, the only factor that was noted to be significant was between survey years 2000 and 2009. The odds ratio (OR) for mortality was 2.97, 95% CI: [1.423–6.202], which indicated that there was an almost three times higher likelihood of mortality in 2009 than in 2000.
Conclusions:
Admission rates appear to remain stable for pediatric inpatients with lymphatic malformations but resource utilization related to charges has been increasing from 2000 to 2009. Controlling for inflation does not explain our observed trend in total charge increases. Previously, surgical resection was the most commonly performed procedure, and now the trend has shifted away from operative intervention. Mortality rates, while low, experienced a rise in 2009. Further investigation may be warranted.
Introduction
M
Improvements in surgical technique with facial neurophysiologic monitoring and more experience with sclerotherapy techniques have been described and have allowed greater control of symptoms related to head and neck lymphatic malformations in children.1,3 Given that these lesions, affect multiple different organ systems and areas of the body, and may present with clinically complex management problems, there has been growth in the development of multidisciplinary vascular anomalies teams all over the country.4,5 We sought to update our understanding and to describe resource utilization trends over the past decade to assess how pediatric admissions and procedures have evolved. We hypothesize that admission rates and resource utilization will have decreased over time with development of widespread multidisciplinary vascular anomalies groups with experience managing these difficult cases in children and mortality rates will have improved.
Methods
The Kids' inpatient database (KID) is a pediatric inpatient care database in the United States included in the Healthcare Cost and Utilization Project (HCUP), which started publishing data in 1997. This study examined inpatient admissions for pediatric patients with lymphatic malformations in years 2000, 2003, 2006, and 2009 using the KID, HCUP, Agency for Healthcare Research and Quality. 6 It is the only all-payer pediatric-specific database in the United States and each year contains weighted information from two to three million hospital stays. The database is updated every 3 years. The content of the KID is de-identified and conforms to Health Information Privacy and Portability Act (HIPPA). Duke University Institutional Review Board approval was obtained before this investigation.
Included cases were identified using DX1-DX25 (the first 25 listed diagnoses) and the ICD-9-CM codes: 228.1–lymphangioma, any site. The HCUP data elements that were assessed as individual variables included the following:
1. AGE 2. DIED–mortality during hospitalization 3. FEMALE (indicates gender) 4. HOSP_LOCATION 5. HOSP_REGION 6. ORPROC 7. PAY1 (3)–private insurance payer and (1,2,4,5,6)–public/uninsured/other 8. PRCCSn 9. RACE (black, Hispanic/Asian/other, white) 10. TOTCHG–Total charges
The KID database from years 2000 to 2009 were used because not all of the data elements were available in the first year of publication in 1997. Trends over time were also assessed. As such, because of the coding methodology adopted by the KID database in 2012, trending of data was not able to be performed. Thus, we chose to exclude those data.
Sample weights, stratification levels, and survey design were taken into account to extrapolate the sampled data to national level. A univariate logistic regression model was used to examine whether there was any significant change in admission rates from 2000 to 2009. A simple linear regression model was fit to assess the temporal trend of total charges per patient. Multivariate logistic regression analysis was used to model the probability of dying during hospitalization as function of the following variables: year of survey, age, ethnicity, insurance payer, hospital location, and teaching hospital status. The adjusted Wald F test was used for analyzing independence between payer, surgical procedures, and the survey year. Statistical analyses were conducted with SAS software (SAS Institute, Inc., 2015, Cary, NC). In all cases, the threshold for assessing statistical significance was set to level α = 0.05.
Results
Annual estimations of inpatient admissions for children with lymphatic malformations in 2000, 2003, 2006, and 2009 were 1689, 1544, 1678, and 1563, respectively (Table 1). Admission rates for each survey year are displayed in Figure 1. No significant increase in admission rates was noted over time (p = 0.5128). Admissions rates varied from 1 to 4 cases per 10,000 inpatient admissions and were relatively evenly distributed across geographic region (Fig. 2). Average total charges per admission were $30,995 and more detailed charge data can be found in Table 1. There was no difference in total charges per admission between 2000 and 2003 (p = 0.3405). However, the total charges per patient in 2006 and 2009 were significantly higher (p < 0.001). There is a clear and increasing trend of total charges per admission; the annual increase from 2000 to 2006 was $13,981 and from 2000 to 2009 was $25,931. This analysis did not control for the inflation rate during the period under consideration. Overall inflation rose about 28% over the time period examined. 7 Even when controlling for the inflation rate, there was a significant increase for overall charges per inpatient admission. There was also a significant increase in the ratio of nonprivate insurance payers across time, and an increasing proportion of these inpatient admissions were associated with nonprivate insurance payers (p = 0.0245).

Admission rate of children with lymphatic malformations.
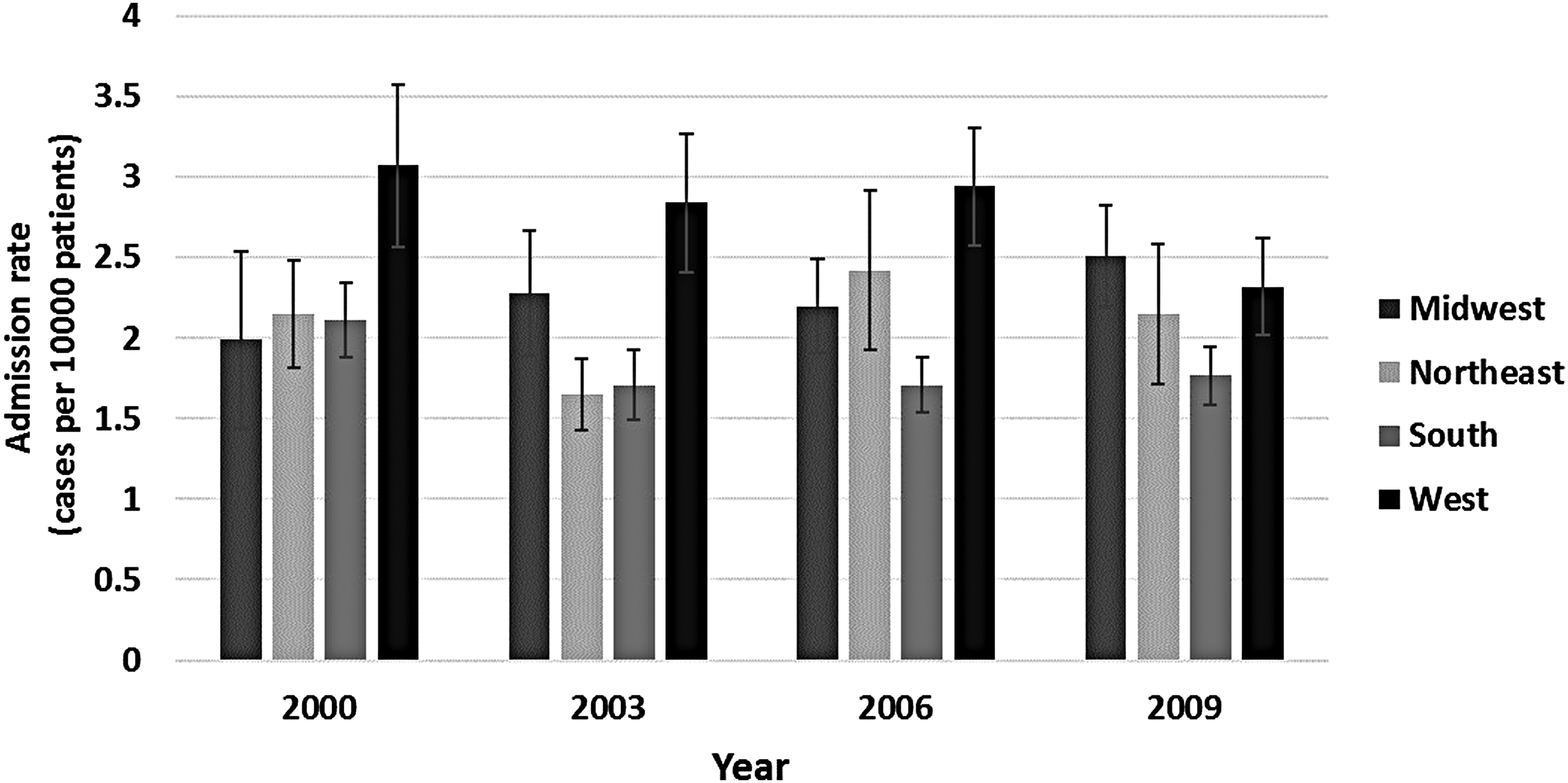
Admission rate of children with lymphatic malformations by geographic region.
The mortality rate due to lymphatic malformations between 2000 and 2009 was overall 1.48%. However, in 2009, the mortality rate increased to 2.58%, which was significantly higher than in previous years and found to be statistically significant (p = 0.0346). The multivariate regression analysis of factors related to mortality indicated that age, insurance payer, hospital location, and teaching hospital status are not significant predictors. The only factor noted to be significant was between survey years 2000 and 2009. The odds ratio (OR) for mortality was 2.97, 95% CI: [1.423–6.202], which indicated that there was an almost three times higher likelihood of mortality in 2009 than in 2000, holding all other covariates constant.
The five most commonly associated procedures codes were as follows: other operating room (OR) therapeutic procedures on nose, mouth, and pharynx; other vascular catheterization, not heart; other therapeutic procedures; hematologic and lymphatic system; respiratory intubation and mechanical ventilation; and other therapeutic procedures (Fig. 3). There was a significant increase in trend over time for using procedure code 231 from 12% to 29% (p < 0.0001).

Five most common procedures performed.
Discussion
Over the past few decades, we have seen a shift in the management paradigm and our approach to lymphatic malformations. These are lesions that tend to be difficult to cure, and these lesions often involve and insinuate themselves intimately with critical neurovascular structures. As treatment of these lesions may lead to significant morbidity, the lens with which we often approach children with this pathology has shifted toward control of symptoms and restoration/preservation of function. 8 There is relatively little standardization in assessment and treatment outcomes. 9 However, relative agreement does exist in that vascular anomalies in children may be best suited to be managed in a multidisciplinary setting. 10 Sclerotherapy and other nonsurgical therapies have been described with reported improved morbidity, and there appears to be a greater proclivity with these minimally invasive options in selected cases over open surgical resection.9,11,12
Our understanding of the scope of the problem and healthcare resource utilization at this time is very limited. One of the last attempts occurred over 10 years ago, an initial report using the KID database by Harsha et al. reported that treatment trends were relatively stable between 1997 and 2000 but hospital charges were increasing over time. The number of inpatient cases and associated costs were relatively low, with only 3200 admissions during the years 1997 and 2000 combined, resulting in estimated national hospital charges of $26 million and $35 million, respectively. At that time, surgical excision was the most common procedure performed, and sclerotherapy was infrequently utilized. Airway endoscopy was the second most common procedure, which may have indicated that a significant proportion of these lesions affect the head and neck area. 13 Other authors have described that in the head and neck, lymphatic malformation treatment with primary surgery utilized equal resources and demonstrated similar effectiveness to primary sclerotherapy. 14 As the paradigm for management of lymphatic malformations has evolved and costs related to both surgery and interventional radiology techniques are similar, even with shifts one way or the other, if they continued to be implemented at the same rate, there should be no significant change in total charges. And with advancing technology, the hope is that the treatment outcomes may improve and potentially drive down associated charges, as these lesions tend to be chronic conditions.
Our results indicate that the estimated frequency of inpatient pediatric admissions with the diagnosis of lymphatic malformation has remained relatively stable over the decade under consideration. There has been a steady increase in the total charges from 2000 to 2009. When controlling for inflation rate using the consumer price index, 7 there still appears to be significant increases in charges per hospital admission over time. It appears that resource utilization for this problem in children continues to rise in regards to total charges and admission rates. One area of further study that may help to further clarify this observation is to try to determine whether there has been a shift in lymphatic malformation associated lymphocytopenia, which has been demonstrated to increase hospitalization requirements, rates of infection, and utilization of more intensive antibiotic therapy compared to nonlymphocytopenic lymphatic malformation patients. 15 Lymphatic malformations in children may also be chronic conditions. Changes in the paradigm for care, coordinated by a multidisciplinary team, may utilize significant resources, resulting in increasing hospital charges. However, there appears to be a notable shift in the primary insurance payer status for inpatient children with lymphatic malformations from private to nonprivate. With healthcare insurance coverage at the forefront of national politics, this may disproportionately affect these children.
Fortunately, it appears that lymphatic malformations in children are not frequently associated with mortality, but it is somewhat alarming that over time, in 2009, there was a significant jump in mortality rate. Our investigation is currently not suited to explain or understand why this happened or if it will be a continuing trend. It may be possible that increases in multidisciplinary care are maintaining inpatient hospital admission rates level, and those children with lymphatic malformations who are admitted may be more severely affected or sicker. Further investigation may be helpful in trying to identify clinical factors that may have caused this increase, in an attempt to improve treatment outcomes for pediatric patients with lymphatic malformations.
It is worth noting that of the most commonly performed procedures, only one involved the operating room, specifically involving the nose, mouth, and/or pharynx. This may indicate that the head and neck area may be a commonly involved area, and that pediatric care providers should be familiar with this clinical entity. The trend in rise of use of other therapeutic procedures is interesting, and it appears to indicate that there is a shift away from operative procedures or surgical resection. It is difficult to ascertain or interpret whether or not this is related to a change in coding techniques or a change in clinical practices related to shifts away from operative surgical resection or debulking to interventional radiology and drainage with or without sclerotherapy. Of note though, there were no other operative room procedure codes listed in the five most common, which appears to suggest that there has been a relative increase in nonoperative management for inpatient admissions in children with lymphatic malformations, and potentially a shift away from surgical resection. A shift away from surgical intervention for pediatric inpatients admitted with lymphatic malformations has not resulted in decreased hospital charges.
Conclusions
Admission rates and resource utilization related to total charges appears to remain stable for pediatric inpatients with lymphatic malformations from 2000 to 2009. Previously, surgical resection was the most commonly performed procedure, and now the trend has shifted away from operative intervention. Mortality rates, while low, experienced a rise in 2009; further investigation may be warranted to investigate potentially contributing factors.
Footnotes
Acknowledgments
J.R. was supported by the National Institutes of Health under award number K08-DK100534. A.E.F. and B.L. were supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR001117. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health (NIH).
Disclosure Statement
No competing financial interests exist.