
Abstract
Abstract
Background:
Bioimpedance is a commonly used technique for detection of early lymphedema. The thresholds used for detection are based on impedance measurements obtained in Western populations. It is unknown whether these thresholds are applicable to a Chinese population.
Methods and Results:
Impedance measurements were obtained for both arms in 391 women, ranging in age from 20 to 84 years, using a standardized protocol. Frequency distributions of interlimb impedance arm ratios for both dominant:non-dominant and non-dominant:dominant were used to determine thresholds at two and three standard deviations (SDs) above the mean. Absolute impedance was significantly higher in the youngest group (20–39 years) compared to other age groups. However, there was no significant effect of age on impedance ratios. Similarly, there was no significant difference between impedance ratios determined in this study and those from recent studies in the Australia and the United States, which used similar protocols. New two and three SDs above the mean thresholds, using a weighted average from the pooled data of these studies are 1.108 and 1.153 for use when the dominant limb is at-risk and 1.072 and 1.116 when the non-dominant limb is at-risk.
Conclusion:
There was no effect of ethnicity on impedance ratios. Consequently, the proposed pooled thresholds can be used, irrespective of ethnicity.
Introduction
S
A variety of methods are used to measure change in arm volume, which is assumed to be indicative of lymphedema, including water displacement, and measurement of arm circumference with a tape measure or perometry.4,5 While a range of thresholds have been used to detect mild lymphedema, with the most common being either an absolute 200 mL interlimb difference or 10% interlimb difference irrespective of arm dominance, 1 Dylke et al. 6 demonstrated that normative-based circumferential measurements corrected for arm dominance were superior.
Bioelectrical impedance has also proven to be useful for the assessment of BCRL, especially at the early stage.7,8 It has the advantage of being specific for extracellular fluid (lymph) accumulation and is faster to perform than tape measurement. 7 Bioelectrical impedance measures the opposition of the tissues to the flow of an electric current. This measured impedance is quantitatively but inversely related to fluid volume. 9 Since the absolute value of the impedance varies with the individual, in unilateral cases of lymphedema, the impedance of an affected or at-risk arm is expressed as a ratio to impedance of the contralateral unaffected or normal arm. 9 Using the ratio also accounts for changes in arm volume that may occur independent of lymphedema. 9 Indication of presence of lymphedema relies upon comparison of this ratio to a reference range derived in healthy people. In practice, some instruments convert the ratio to a linearized index, such as the L-dex used by ImpediMed, Ltd. (Brisbane, Australia), for identification as to whether the ratio is within the healthy range. Reference data are available for Western populations.7,10,11 It is unknown whether these are applicable to women of different body habitus, for example, Asians. Impedance is determined by the inherent dielectric properties of tissues and the geometry of the body region being measured. Although dielectric properties of tissues are determined by underlying physiology, for example, ion status, which is not expected to vary between populations, recent evidence suggests that subtle differences do exist. 12 In addition, body geometry is known to differ between populations,13–15 and indeed within Asian populations. 16 Consequently, impedance varies between ethnic groups. 17
The aims of this study was to determine the normal variation in upper arm impedance values in adult women in China; determine a normative reference range for use in assessment of unilateral arm lymphedema by bioelectrical impedance and confirm whether normative-based impedance thresholds identified for Western women are appropriate for Chinese women despite the differences in body habitus.
Materials and Methods
Participants
Participants were self-reported healthy women recruited from both urban and regional areas in Shanghai, China. Recruitment was either from women attending a local community health surveillance program or by poster and internet advertising in local hospitals and the university. All participants were over 20 years of age with no history of breast cancer or lymphedema. Participants were excluded if fitted with a pacemaker (contraindicated for impedance measurement), were pregnant, taking diuretic medication, or recently undertaken activities that may have markedly altered their hydration status. All participants gave written informed consent before participation in the study. The study was approved by the Huashan Hospital Ethics Committee in Shanghai, China.
Participants attended a single session in which they were weighed, without shoes and in light clothing, to the nearest 0.1 kg and height measured using a stadiometer to the nearest millimeters. In addition, the impedance in each arm was measured with a single low frequency impedance device (XCA; Impedimed, Ltd.).
A total of 391 women were recruited, with 46 aged 20–39 years; 60 aged 40–54 years; 167 aged 55–64 years; 104 aged 65–74 years; and 14 aged 75 years or older, reflecting the age distribution of breast cancer cases in China. 18 Participant characteristics are reported in Table 1. Participants' ages ranged from 20 to 84 years; the mean (standard deviation [SD]) age was 57.2 (13.0) years. Body mass index (BMI) ranged from 13.5 to 36.9 kg/m2 with the 65–74 years age group showing the highest mean BMI.
Mean (SD) are displayed.
BMI, body mass index; SD, standard deviation.
Measurement of upper arm impedance
Measurement of impedance of arms has been described in detail elsewhere.5,19 Briefly, upper arm impedance (wrist to axilla) was determined according to the principles of equipotentials with participants positioned in supine on a nonconducting surface with limbs slightly abducted and palms facing down. All jewelry, including watches, were removed before measurement. The electrode locations were as described by Cornish et al., 20 that is, current drive electrodes on the dorsal surface of the third metacarpal of the hand and the dorsal surface of the third metatarsal of the foot and the voltage sensing electrodes on the dorsum of the wrists midway between the styloid processes and the dorsal surface of the ankle midway between the malleoli. Electrode sites were cleaned with an alcohol wipe before attaching the electrocardiogram-style Ag-AgCl gel electrodes.
Impedance was measured using a single low frequency impedance device (XCA; ImpediMed, Ltd.). Frequency of measurement is unspecified by the manufacturer but is <30 kHz. Data obtained with this single frequency device are highly concordant with data obtained with multi-frequency impedance spectroscopy devices. 19 The XCA device measures impedance for each arm and provides the impedance ratio between limbs. The impedance ratio, when the dominant arm is “at-risk,” is calculated as the impedance of non-dominant arm divided by the dominant arm, whereas when the non-dominant arm is “at-risk,” the impedance ratio is expressed as the impedance of the dominant to non-dominant limb.
Statistical analysis
All data are presented as mean ± SD. The impedances were tested for outliers using Tukey “far out” test resulting in eight cases (2%) being removed. Analysis of variance (ANOVA) and Duncan's post hoc test were used to determine whether participant characteristics or impedance data were significantly different between age groups. The effect of dominance on impedance was tested using paired t-tests. Regression analysis was undertaken to determine whether age, height, or weight were related to impedance ratios. Frequency distributions were determined for the raw impedance and interlimb impedance ratios; Cook's distance was used to determine the number of influential points, which could distort normality.
The thresholds for classifying women as likely to have lymphedema were determined for both the dominant and non-dominant arm. These thresholds were established using the previously reported approach in which diagnostic cutoffs are set at the mean plus two or three times the SD,8,11 thereby encompassing >95% of the population. The mean impedance ratios were compared to previously published data using ANOVA with post hoc tests when significant differences were identified. Data were analyzed using SPSS for Windows (version 22; IBM) and Microsoft Excel (2013).
Results
The participant characteristics and impedance data are presented in Table 1. ANOVA revealed significant differences in height between the age groups (F4385 = 17.21; p > 0.01) with Duncan's post hoc analysis showing that the youngest-aged group, 20–39 years, were significantly taller than the other cohorts. Significant differences in weight were also found (F4384 = 5.10; p = 0.001), again with the youngest group weighing significantly less than that of the 40–74 years age groups on Duncan's post hoc analysis. Consequently, BMI differed significantly across ages (F4384 = 11.79; p > 0.01), with the BMI of the youngest age group significantly lower compared to all other aged groups. There was a significant difference in the raw impedance for both the dominant (F4384 = 19.10; p > 0.01) and non-dominant (F4385 = 19.0.4; p > 0.01) arms between the age groups, with the impedance of the youngest group significantly larger than those of all other age groups on post hoc analysis. In all age groups, both impedance (t = 8.00; p > 0.01) and resistance (t = 6.50; p > 0.01) of the non-dominant arm was significantly greater than that of the dominant arm. Regression analysis revealed that age, height, and weight were not significantly related to the impedance ratio.
The impedances and impedance ratios distributions are displayed in Figure 1A–D. The normal probability plots (Fig. 1E, F) highlights the normal distribution of the impedance ratios. Cook's distance, set conservatively at 1.0, deemed only 2 of 391 points deviated from normality.
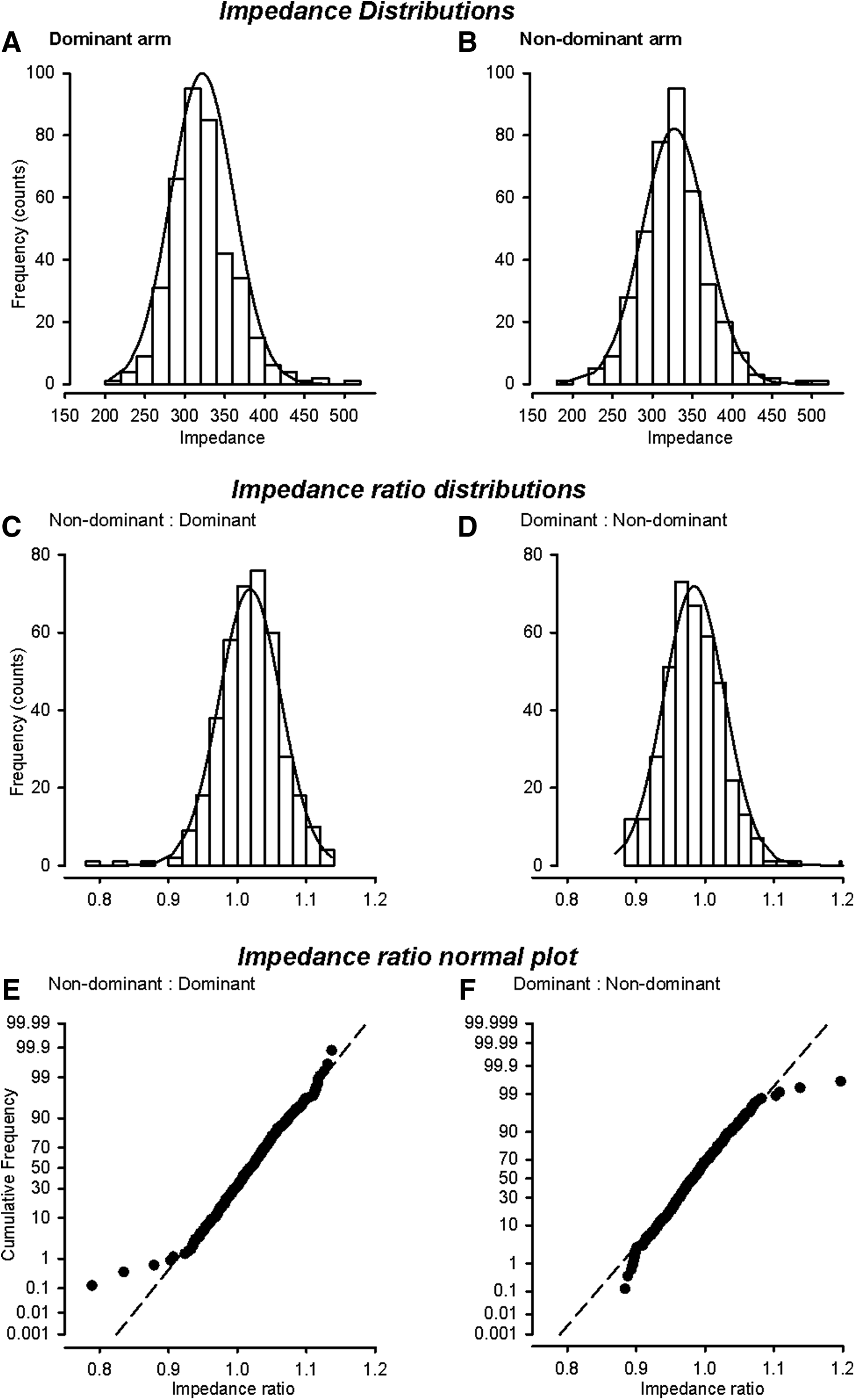
Impedance distribution plots for the dominant
The mean ± SD impedance ratio for when the “at-risk” arm is on the dominant side was 91.018 ± 0.045 and for when the non-dominant limb is at-risk, the impedance ratio was 0.984 ± 0.044 (Table 2). The mean plus two and three SDs thresholds for detection of lymphedema were therefore 1.108 and 1.153 for the “at-risk” dominant arm and 1.072 and 1.116 for the “at-risk” non-dominant arm. These values are not significantly different to those from Ward et al. 11 and Ridner et al. 10 but were significantly different than those published by Cornish et al. 8 (Table 2).
Data were not significantly different from each.
Data differed significantly to that from other studies (p < 0.01).
Proposed thresholds based on weighted averages from studies in which the data were not significantly different, that is, current study, Ward et al., 11 and Ridner et al. 10
Dominant/non-dominant arms.
cv, coefficient of variation.
Conclusions
The major finding from this study was that the impedance ratios for the dominant and non-dominant “at-risk” limbs in Chinese women were not significantly different to those from a similarly large Australian cohort 11 and a smaller American cohort. 10 However, ratios for both the Chinese and the large Western cohort differed significantly from the original smaller Australian cohort. 8 The reasons for these differences between the studies is not entirely clear. However, the protocol used in the original study by Cornish et al. 8 differed slightly to that used in the later studies. Cornish et al. 8 measured the impedance of a 40 cm segment of the arm, commencing at the wrist, and used an early version impedance instrument. The later studies used either an impedance or SFB7, which produce interchangeable measures, 19 and measured the impedance of the whole arm. Whole arm impedance measurements is based on the principle of equipotentials, a technique demonstrated to have greater technical precision than discrete segment measurements. 20
These observations raise the question as to which thresholds on which to base clinical decisions. Ward et al. 11 investigated the effect of choice of thresholds on the classification of a group of women with lymphedema. They found that adopting the newer threshold rather than those put forward by Cornish et al. 8 did not alter the classification of lymphedema in their lymphedema group. However, this may not be the case for participants whose ratio falls between thresholds determined by the different studies. As there was a lack of significance among the three most recent studies that followed similar measurement protocols, we generated weighted average thresholds for both the dominant and non-dominant limbs for both two and three SD above the mean (Table 2) for adoption in clinical practice, irrespective of ethnicity.
Despite the nonsignificance between the three most recent studies, there remains a degree of doubt over the certainty of classification when using absolute bioimpedance thresholds. Others have also raised concern over using an absolute threshold. For example, Cornish et al. 8 addressed this concern by requiring at least two consecutive positive impedance ratios, taken at least 2 weeks apart, to have greater confidence in the assignment of lymphedema. Dylke et al. 6 proposed combining alternative measurement approaches with impedance ratios using a nomogram to improve accuracy of prediction. Dylke et al. 6 found better positive likelihood ratios when three SD thresholds from Ward et al. 11 were used compared to those from Cornish et al. 8
A notable finding of the present study was the significantly larger absolute impedance values of the dominant and non-dominant limbs of the youngest cohort (20–39 years). This is presumably due to longer arm lengths in this population, impedance varies proportionately with length, since the youngest group were significantly taller than the other age groups. Despite this significant observation, their impedance ratios were not significantly different to the other age groups. This highlights the advantage of using impedance ratios rather than absolute impedance values for detection of lymphedema. 9
For the first time, criterion thresholds for the assessment of lymphedema using bioimpedance in Chinese women were determined and were shown not to be significantly different to those obtained in similarly conducted studies in Australia and the United States. New thresholds based on the weighted average from these combined studies are proposed for clinical adoption.
Footnotes
Acknowledgment
The authors acknowledge the assistance provided by Chen Junyu, Xie Na and Shao Peng in data collection.
Author Disclosure Statement
Author Ward provides consultancy service to Impedimed, Ltd. Impedimed has no input to this article. The other authors have no competing financial interests to declare.