
Abstract
Abstract
Background:
In this randomized controlled study, we aimed to evaluate the effect of shoulder flexion exercise using continuous passive motion (CPM) on lymphedema during the treatment of breast cancer-related lymphedema (BCRL).
Methods:
Thirty patients with BCRL were enrolled and completed the study. Fourteen patients were treated with complete decongestive therapy (CDT) and CPM in the intervention group, and 16 patients were treated with CDT alone (control group) for 15 sessions. The main outcome measures were included; the shoulder range of motion (ROM) assessed with a goniometer, limb volume difference measured using the water immersion method, function with the Disabilities of the Arm, Shoulder and Hand (DASH), and the quality of life using the Functional Assessment of Cancer Therapy for Breast Cancer (FACT-B4). Lymphedema volume measures were taken at baseline, on days 1, 2, 3, 4, 5, 10, and 15; and shoulder ROM, FACT-B4, and DASH were taken at baseline and on day 15.
Results:
All subjects were similar at baseline. After treatment significant improvement was found in ROM, volumetric differences, DASH, and FACT-B4 scores in both groups. No significant differences were observed in the volumetric differences, ROM, and the DASH, and FACT-B4 scores between the groups, except for the FACT-B4 physical well-being subscores, which were better in intervention group.
Conclusion:
Our study results showed that CPM did not contribute to the reduction of BCRL.
Introduction
B
BCRL is a chronic condition with gold standard of treatment being complete decongestive therapy (CDT) as recommended by the International Society of Lymphology. CDT consists of skin and nail care, manual lymphatic drainage, multilayer compression bandages, compression garments, instructions in self care, and exercise. Other adjunct management includes education, taping, intermittent pneumatic compression pump, laser, psychological support, and management of comorbidities.11–15 In addition, continuous passive motion (CPM) is often used as a supportive measure to orthopedic rehabilitation programs to prevent arthrofibrosis following surgical operations to the knee, elbow, and shoulder. It is known to reduce bleeding and edema during the postoperative period, in particular.16–18 It has been also shown to prevent or delay the accumulation of periarticular interstitial fluid. 19 To date, no study investigating the effect of CPM on lymphedema is available in the literature.
In this study, we aimed to evaluate the effect of shoulder flexion exercise using CPM on the lymphedema during the treatment of BCRL.
Materials and Methods
The study was approved by the local ethics committee. The study was conducted in accordance with the principles of the Declaration of Helsinki. 20 Between February 2014 and September 2015, 30 female patients who were diagnosed with BCRL by physiatrist at the outpatient clinic of the Physical Medicine and Rehabilitation Department at Dokuz Eylul University Hospital, Izmir, Turkey were randomly enrolled into the study. There was no suitable comparable study in the literature to use in the calculation of the sample size.
Inclusion criteria for the study were as follows: age between 25 and 75 years, presence of lymphedema for at least 6 months after and at most 8 years after treatment of breast cancer, the presence of unilateral lymphedema, and at least 2-cm difference at a point, between affected and unaffected arm. Exclusion criteria included prior treatment for lymphedema over the past year, local or distant cancer recurrence associated with breast cancer, active infection or deep venous occlusion, additional diseases or psychiatric disorders interrupting the follow-up schedule, history of bilateral mastectomy, and severe shoulder pain and frozen shoulder. The study was designed as a prospective, single blinded randomized controlled trial. Before the beginning of the study, an independent researcher (E.A.) provided a randomization scheme from a random number table using block randomization with four patients in a block. The eligible patients who had submitted a written informed consent were then referred to another researcher (E.S.) who was not involved in the selection and consent process. This researcher used the randomization scheme to assign patients into intervention or control groups. This process thus ensured allocation concealment.
Demographic characteristics, arm dominance, previous type of surgery, presence of lymph node dissection, presence or absence of arm pain, treatments received for lymphedema, and the duration of lymphedema for both groups were evaluated by a researcher (O.E.) blind to group allocation at the outpatient clinic of the Department of Physical Medicine and Rehabilitation. Angle measurements of shoulder range of motion (ROM), including the flexion, abduction, and internal and external rotation, were goniometrically obtained during the physical examination of the patients at baseline and on day 15. Lymphedema volume of the upper limb was measured using the water displacement volumetry. A water measurement cup was used to measure the water overflowing, after dipping the arm to a water level in the arm volumetry, at a sign which was placed 15 cm below the acromioclavicular joint from an anterior point of the patient arm. A volume difference of 200 mL or more between the affected and unaffected arms is typically considered to be a cutoff point to define lymphedema. The lymphedema stages were divided into four categories according to Common Toxicity Criteria Version 3.0 (CTCAEV3.0). The objective measure for each stage was primarily distinguished by limb volume differences: 5%–10% equal to grade 1, >10%–30% equal to grade 2, >30% equal to grade 3, and grade 4 described as progression to malignancy. 21
All patients were divided into two groups according to the randomization schedule for a duration of 15 sessions; the control group (n = 16) used the CDT program (self-manual lymphatic drainage, multilayer short stretch compression bandage, instructions in self-care, therapeutic exercise (supervised, ROM, and strengthening program were given by researcher), and meticulous education on skin and nail care). In the intervention group (n = 14), shoulder flexion directed passive ranging exercise program with CPM was applied after CDT was being performed (Fig. 1). Self manual lymphatic drainage was taught and shown individually to each patient for 20 minutes. The patients were subjected to CPM (Kinetec Centura Shoulder CPM model Michigan St. NE) with third-level speed plus flexion-directed exercise up to approximately 90% of the shoulder joint ROM for 20 minutes in the first five sessions and for 30 minutes in the next ten sessions. A researcher (AS) conducted all these treatments for 15 sessions, 60 minutes of CDT and 30 minutes of CPM per session on consecutive days at the outpatient clinic of the Physical Medicine and Rehabilitation Department at Dokuz Eylul University Hospital.

Shoulder flexion exercise with CPM. CPM, continuous passive motion.
Volumetric measurements were performed at baseline and on the 1st, 2nd, 3rd, 4th, 5th, 10th, and 15th treatment days. In addition, the functional evaluation was performed using the Turkish version of the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire. The DASH outcome measure is a 30-item questionnaire designed to assess musculoskeletal disorders of the upper limbs. 22 The DASH scores range from 0 to 100, with higher scores indicating a greater level of disability. 23 In contrast, the quality of life of the patients was evaluated using the Functional Assessment of Cancer Therapy for Breast Cancer (FACT-B4) questionnaire. The FACT-B4 questionnaire includes several sections, namely “Physical Well- Being,” “Social/Family Well- Being,” “Emotional Well- Being,” “Functional Well- Being,” and “Additional Concerns.” 24 Lower scores indicate a lower level of functioning. The FACT-B4 and DASH questionnaires were administered at baseline and at the end of 15 sessions. All measurements and questionnaires were made by a blind researcher (O.E.).
Statistical analysis
SPSS 22.0 software package (SPSS, Inc., Chicago, IL) was used for data analysis. Kolmogorov–Smirnov test was used to determine if the data were close to the normal distribution. Analyses of variance (ANOVA) in repeated measures (ROM and volumetric measurements) were used. Groups were compared for differences using the Mann–Whitney U test, and within-group differences were analyzed using the Wilcoxon signed-rank test for differences between baseline and follow-up days (1,2,3,4,5,10,15). A p-value less than 0.05 and a 95% confidence interval were considered statistically significant. All analyses were conducted on a per protocol basis. In the post hoc power analysis, performed using sample sizes, means, and SD values for the significance level (>) of 0.05, the power was calculated using the statistical DSS research program.
Results
Forty patients met inclusion criteria during their routine outpatient physical examination for lymphedema. After reviewing inclusion and exclusion criteria, 32 patients with BCRL who had submitted written informed consent were included in the study. Two patients in intervention group were lost at follow-up. Therefore, 30 patients completed the study (Fig. 2). During treatment, no complications were observed in the study groups. Fourteen of 30 patients were randomized into intervention group (CDT with CPM), while 16 patients were randomized into control group (CDT alone). Baseline characteristics are reported in Table 1 and the groups appear to be well matched. There was no significant difference in the age, body mass index, education status, duration of lymphedema, pain presence, stage of lymphedema, affected side, and dominance between the groups (p > 0.05) (Table 1). All participants in both groups had modified radical mastectomy, axillary lymph node dissection, (adjuvant/neoadjuvant) radiotherapy, and chemotherapy except for one patient in intervention group who had surgery only.
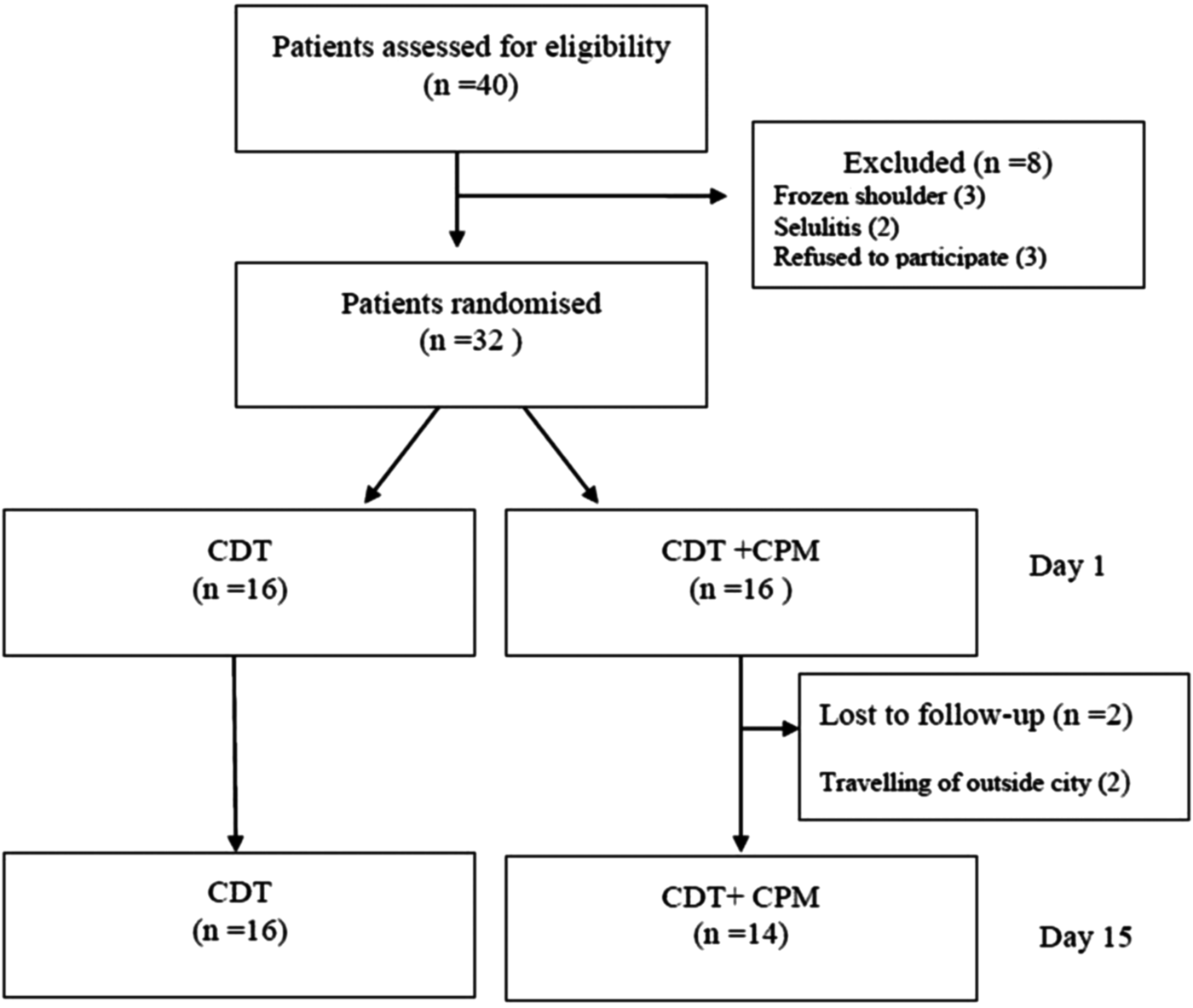
Flow diagram of patients.
Median (min–max).
Primary school and preprimary school/postprimary school.
BMI, body mass index; NALN, number of axillary lymph node; ER, estrogen receptor; PR, progesterone receptor; ROM, range of motion.
The shoulder joint ROM and volumetric measurements significantly improved during follow-up in both groups, compared to the baseline values (p < 0.05). However, there was no significant difference in these parameters at baseline and during all follow-up days of treatment (p > 0.05) (Tables 2 and 3).
ANOVA within-group measurements p < 0.001, between-groups p = 0.83.
ANOVA within group measurements; Flexion and abduction: p: 0.01, external rotation p: 0.02, internal rotation p: 0.009.
In addition, a significant improvement in the DASH and FACT B-4 scores was reported on the 15th day of treatment, compared to the baseline scores in both groups (p < 0.05). However, no significant differences were observed in the DASH and FACT B-4 scores between the groups (p < 0.05), except for the FACT B-4 physical well-being subscores (p = 0.03), which were better in intervention group (Tables 4 and 5).
p < 0.05.
p < 0.05.
In the post hoc power analysis, performed using sample sizes, means, and SD values for the significance level (alpha) 0.05, the power was found to be below 50% for physical well-being score and other outcome measurements.
Discussion
In this first randomized controlled study, although CPM and CDT were effective in decreasing volumetric lymphedema or improving the shoulder joint ROM, quality of life, and functional recovery, we were unable to show that addition of CPM to CDT was more effective compared to CDT alone in patients with BCRL. We suggest that CDT is an effective and safe treatment for reducing lymphedema. Our results showed that CPM does not have the additional effect of reducing lymphedema. Moreover, CPM may increase the time period and total cost of treatment. Although we did not find any statistically significant difference in the reduction of lymphedema between the two groups, numerically larger reductions were observed in intervention group. The sampling interval may have affected the statistical significance. Therefore, further controlled studies involving a greater number of patients over a longer period are needed to facilitate a more in-depth investigation of lymphedema treatment.
Lymphedema can also lead to serious conditions, such as cellulitis, lymphangitis, decreased ROM of the affected limbs, body image disturbance, and pain, while psychological problems, including anxiety, depression, and emotional distress, may adversely affect the quality of life of these patients.15,25 Shoulder dysfunction is a consequence of surgery, where scarring of the healed wound limits the movement of the operated side. Patients may have difficulties in moving that side in daily activities, such as reaching above the head or fastening clothes from behind. The reported prevalence of decreased ROM in the shoulder with breast cancer varies across studies from 1% to 67% in a systematic review. 26 In a recent study, prevalence of restricted shoulder ROM in patient with breast cancer was reported to be 23.9%. 27 In addition, decreased ROM and lymphedema are closely related, as the latter hinders the shoulder movement and becomes worse by itself in the meanwhile. A Cochrane review revealed that shoulder mobility exercises (i.e., lateral movements and forward flexion) significantly contributed to the improvement of shoulder ROM in women with breast cancer. 28 Similarly, we also observed an increased shoulder ROM in all patients although there was no significant differences between the groups.
In general, CPM has traditionally been used to reduce edema and bleeding of the joint and surrounding soft tissue in the postoperative rehabilitation in the orthopedic population, thereby improving the limitation of the extremity.17,18 Several studies have demonstrated that CPM is often used for the elbow, shoulder, and knee orthopedic rehabilitation.17–19 In a study evaluating the effects of the CPM on edema in 16 hemiplegic patients with arm edema, the effect of including 30-minute treatment with CPM and elevation on volume was investigated, and CPM significantly contributed to the reduction of edema. 29 Furthermore, CPM and elevation were reported to together markedly increase lymphatic and venous drainage, thereby reducing edema.29,30 However, the protein content of edema was reported to be associated with viscosity and that treatment response could be reduced in conditions where the duration of edema was prolonged. In literature, Vignes et al. 31 reported that duration of lymphedema before intensive phase of decongestive physiotherapy and BMI were two predictors influencing reduction of lymphedema volume. According to a study, patients with lymphedema duration less than 2 years had more volume reduction than those with duration greater than 2 years after lymphedema treatment. 32 In our study, mean duration of the patients were longer than 2 years. The expected effect of CPM on lymphedema could not have been attained, as a result of this prolonged period.
In another uncontrolled study, including patients with BCRL, myolymphokinetic exercise-facilitating devices were reported to reduce edema at the end of 1-hour exercise program, compared to the baseline without reducing the therapeutic effect. 33 In another prospective study of 21 patients with BCRL, the active exercise-facilitating mobile flexion bar was used and edema reduced volumetrically following a 12-minute application, compared to the baseline. 34 In these two studies, active exercises had been given with different devices in patients with BCRL. However, we used a passive exercise with CPM for decreasing lymphedema. CPM, which provides repetitive movement of a joint either through full or partial ROM and elevation, may have potential for reducing edema. This study is the first randomized controlled trial to investigate the short period effect of CPM in the treatment of BCRL. However our results showed that CPM did not contribute to the reduction of BCRL. Passive exercises are preferable to active exercises as they demand less energy. 35 However, active exercises are important to assist in maintaining the muscle trophism and maintaining the efficacy of contractions. We think that CPM may choose for patients with BCRL which have shoulder pain or weakness.
As breast cancer patients commonly experience symptoms of fatigue, anxiety, and depression, both the disease and its treatment pose many challenges to physical, emotional, mental, and social well-being and the quality of life. In particular, limited shoulder ROM may adversely affect the functional capacity and quality of life of the patient.36–38 In our study, we observed an improved quality of life in both groups, compared to the baseline; however, statistically a higher number of patients undergoing CPM experienced physical well-being. We think this result may only be associated with a statistical outcome or may have contributed to reducing shoulder pain in patients with BCRL. Also it may be increasing in patient satisfaction through this way. However, we did not follow patient satisfaction and shoulder pain numerically.
In contrast, there are some limitations to this study. First, the study involved a small sample size in patients with BCRL. Also future study may explore use of CPM in people with early stages of lymphedema, short-term effectiveness of CPM to lymphedema, and contribution of passive ROM exercise with CPM in direction of abduction. Therefore, long-term effects of CPM should be investigated in further large-scale studies. In addition, it may be beneficial to examine a particular subgroup of patients with lymphedema (e.g., patients with shoulder pain/hemiplegic shoulder and difficulty performing active exercise may benefit from passive ROM exercise using CPM). Second, it would be unethical to include a placebo treatment group, or withhold treatment from patients; therefore an observation group would not be possible. Third we did not ask patient satisfaction treatment of CPM, it may be comfortable for patient.
In conclusion, CPM, when applied for 2 weeks, in combination with CDT, was no more effective than CDT alone. Both treatment groups demonstrated effectiveness in the reduction of lymphedema, improvement in shoulder ROM, quality of life, and function in patients with BCRL.
Footnotes
Acknowledgments
The authors wish to thank the people who participated in this study.
Author Disclosure Statement
We declare that we have no competing interests.