
Abstract
Abstract
Background:
Although genital lymphedema is a challenging disease, its mechanism is unclear. The aim of this study was to identify the lymphatic flow in genital lymphedema and establish a suitable examination for genital lymphedema.
Methods:
We injected phytic acid or albumin labeled with 99mTc at the bilateral first web spaces of the feet of 47 patients for lymphoscintigraphy. For indocyanine green (ICG) lymphography, we injected ICG into the first web spaces of both feet and other points if necessary. We established a genital pathway score (GPS). In GPS 0, there was no dermal backflow in genitalia. In GPS 1, dermal backflow was observed in the genitalia, but not in the groin. In GPS 2 and 3, splash pattern and stardust pattern were in the genitalia, respectively, with dermal backflow in the groin.
Results:
Twenty-eight patients (59.6%) reported subjective symptoms of genital lymphedema. Accumulation of isotope in the genital region was observed on 32 sides (34.0%) in lymphoscintigraphy. On ICG lymphography, 37 sides were classified as GPS 0. Nine sides were GPS 1, which indicated that the lymphatic accumulation in the genitalia seemed to flow from the contralateral side. Twelve sides were GPS 2, and 36 were GPS 3. Dermal backflow was observed in 60.6% of patients. Chi-square tests showed a significant relationship between prior radiotherapy and the presence of genital lymphedema (p = 0.046).
Conclusions:
A pathway from the inguinal lymph nodes to the genital region was observed on lymphoscintigraphy in genital lymphedema. The sensitivity was greater with ICG lymphography than lymphoscintigraphy.
Introduction
G
Few articles have reported imaging findings in genital lymphedema. Yamamoto et al. reported the results of indocyanine green (ICG) lymphography in genital lymphedema, and described a genital dermal backflow stage. 3 However, in patients with severe lymphatic dysfunction in their limbs, it is difficult to evaluate genital lymphedema with conventional ICG lymphography because ICG cannot reach the genital region or even the thigh in severe cases. And there are only case reports to present the results of lymphoscintigraphy in genital lymphedema. 4
In this study, we performed lymphoscintigraphy for lower limb lymphedema. We also performed modified ICG lymphography and compared the results with those for lymphoscintigraphy. By clarifying the mechanism of genital lymphedema, it would be easier to select suitable treatment, including physiotherapy or surgery.5–9 The aim of this study was to identify the lymphatic flow in genital lymphedema and establish a suitable examination for genital lymphedema.
Patients and Methods
We performed lymphoscintigraphy and ICG lymphography of the lower limb in consecutive lymphedema patients who were hospitalized in Saiseikai Kawaguchi General Hospital from November 14, 2016, to March 9, 2017. This study was approved by the institutional ethics committee (approval no.: 26-6), and written informed consent was obtained from each patient.
The subjective symptoms of genital lymphedema were obtained for each patient. And the experienced lymphatic surgeon (H.H. and M.M.) diagnosed the presence of edema in the genital region.
We injected phytic acid or albumin labeled with 99mTc at the bilateral first web spaces of the feet for lymphoscintigraphy as previously reported.10,11 Scintigrams were performed 15, 30, 60, and 90 minutes after injection. We took the images 60 minutes after injection for the evaluation, as it seemed desirable to evaluate both the inguinal and genital regions. Lymphoscintigraphic findings were typed according to the Maegawa classification 12 : decreased number of lymph nodes and collateral lymphatic vessels in type 1, dermal backflow in the thigh in type 2, dermal backflow in the whole limb in type 3, dermal backflow in the lower leg in type 4, and no dermal backflow in type 5. We judged the result as “positive” when accumulation of isotope was observed in the genital region.
For ICG lymphography, we injected 0.1 mL of ICG (0.5% Diagnogreen; Daiichi Pharmaceutical, Tokyo, Japan) into the first web spaces of both feet. If ICG did not reach the groin region due to severe lymphatic dysfunction, we injected additional ICG in the lower leg or thigh, which are alternate locations for ICG lymphography. We waited at least 2 hours until the ICG was fixed and observed the lymphogram* with an infrared camera (Photodynamic Eye; Hamamatsu Photonics, Hamamatsu, Japan). The findings in the genital and inguinal regions were recorded as splash or stardust patterns, when present.
We established a genital pathway score (GPS) to evaluate the severity of genital lymphedema (Fig. 1). In GPS 0, no dermal backflow was observed in the genital region. In GPS 1, dermal backflow was observed in the genital region but not in the inguinal region. In GPS 2, a splash pattern was observed in the genital region, with dermal backflow in the inguinal region. In GPS 3, a stardust pattern was observed in the genital region, with dermal backflow in the inguinal region.
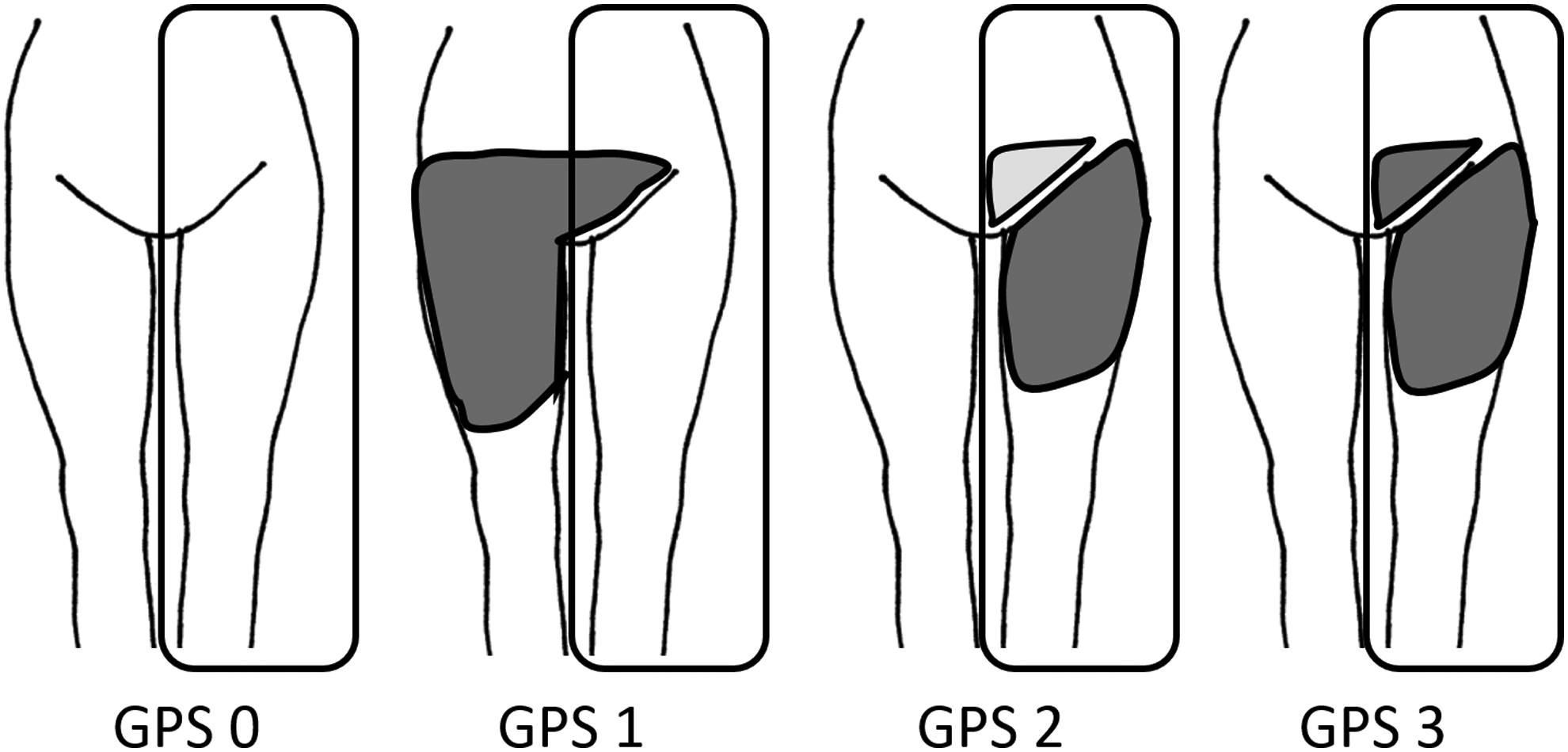
Schematic presentation of the GPS. In GPS 0, no dermal backflow is seen in the genital region. In GPS 1, dermal backflow is observed in the genital region, but not in the inguinal region. In GPS 2, a splash pattern was observed in the genital region, with dermal backflow in the inguinal region. In GPS 3, a stardust pattern was observed in the genital region, with dermal backflow in the inguinal region. GPS, genital pathway score.
We diagnosed genital lymphedema if patients had subjective symptoms, isotope accumulation on lymphoscintigraphy, or dermal backflow in ICG lymphography. We compared the results with those in patients previously treated for cancer with lymph node dissection, radiotherapy, and chemotherapy. We performed chi-square tests with a significance level of 0.05.
Results
We performed lymphoscintigraphy and ICG lymphography in 48 patients. We could not obtain lymphoscintigraphic images in one patient and thus investigated 94 sides of 47 patients (right side and left side of genital region were separately counted).
The average age was 59.3 years (range 31–82), and all patients were females. The causes of lymphedema were cervical cancer in 23 patients, ovarian cancer in 12 patients, uterine body cancer in 7 patients, and rectal cancer in 1 patient. Six patients had primary lymphedema. Three of them were classified as praecox, and the others were tarda, in Kinmonth classification. One of the patients underwent lymphadenectomy for vertebral tuberculosis when she was 3 years old. Forty patients (85.1%) underwent lymph node dissection, 10 (21.3%) underwent radiotherapy, and 20 (42.6%) underwent chemotherapy for cancer. Twenty-eight patients (59.6%) reported subjective symptoms of genital lymphedema and all of them were diagnosed as genital lymphedema based on the clinical appearance.
Based on the Maegawa classification, 34 limbs were type 1, 17 were type 2, 22 were type 3, 14 were type 4, and 8 were type 5. In some patients, accumulation of isotope and a pathway from an inguinal to a genital lymph node could be observed (Fig. 2). Accumulation of isotope in the genital region was observed on 32 sides (34.0%) and absent in 62 (66.0%) (Fig. 3). Among 20 sides with Maegawa type 4 or 5, 19 (95.0%) showed no isotope accumulation, and 1 was positive for isotope accumulation; the latter appeared to have collateral lymphatic flow from the contralateral genital region. The difference in the percentage of isotope accumulation between Maegawa types 1–3 and types 4 and 5 was statistically significant (p = 0.002).

Lymphoscintigraphic images of genital lymphedema. Pathways from the inguinal lymph node to the genital region are observed (white arrows). Black arrow indicates lymphatic stasis in the genital region.
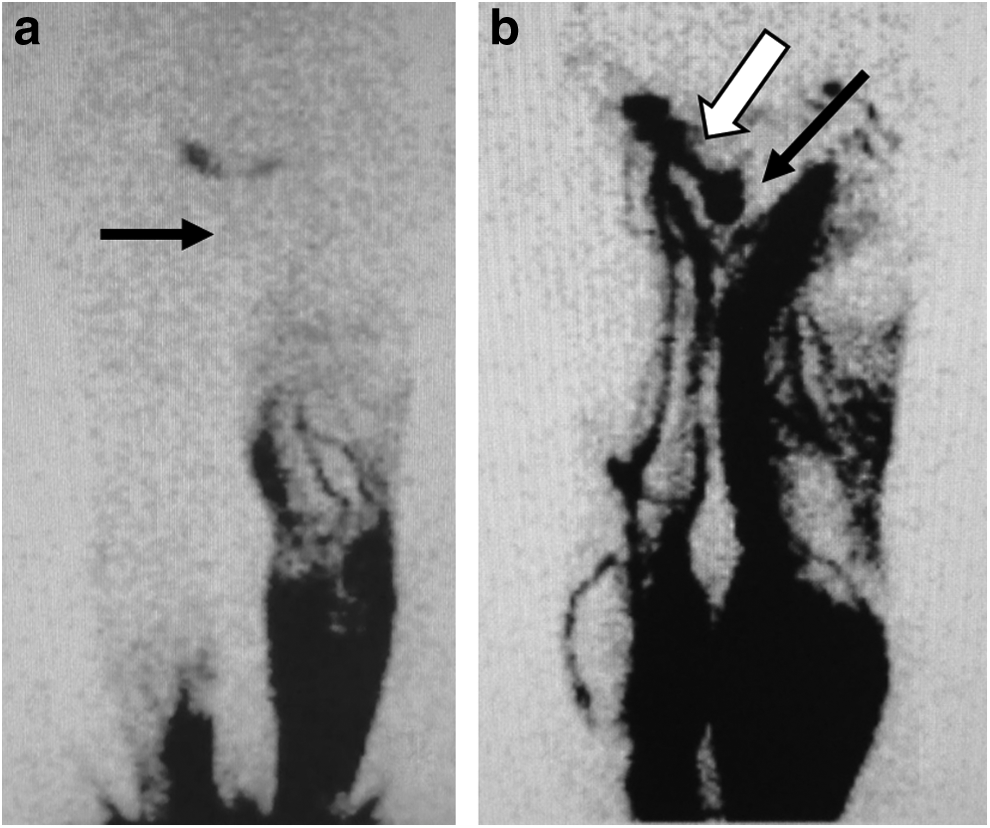
Lymphoscintigraphic images.
On ICG lymphography, among 94 sides of 47 patients, 37 (39.4%) did not have dermal backflow in the genital region and were classified as GPS 0 (Fig. 4). Nine sides were classified as GPS 1 (9.6%), with no dermal backflow in the inguinal region (Fig. 5). The lymphatic fluid accumulation in the genital region seemed to flow from the contralateral side. Twelve sides were classified as GPS 2 (12.8%), and 36 were classified as GPS 3 (38.3%). Dermal backflow was observed in 60.6% of patients. The sensitivity and specificity were 0.88 and 0.70, respectively. In 13 sides of 11 patients, despite their lack of awareness, ICG lymphography indicated genital lymphedema; stardust pattern in seven sides, which indicated moderate lymphedema, and splash pattern in six sides, which indicated mild lymphedema. In six sides, no dermal backflow was observed, although the patients and we noticed abnormal swelling in the genital region. All of them had secondary lower limb lymphedema. Among 12 sides of 6 primary lymphedema patients, 1 side had obvious genital lymphedema with dermal backflow in ICG lymphography, and 2 sides had dermal backflow in ICG lymphography without an obvious clinical appearance of lymphedema.
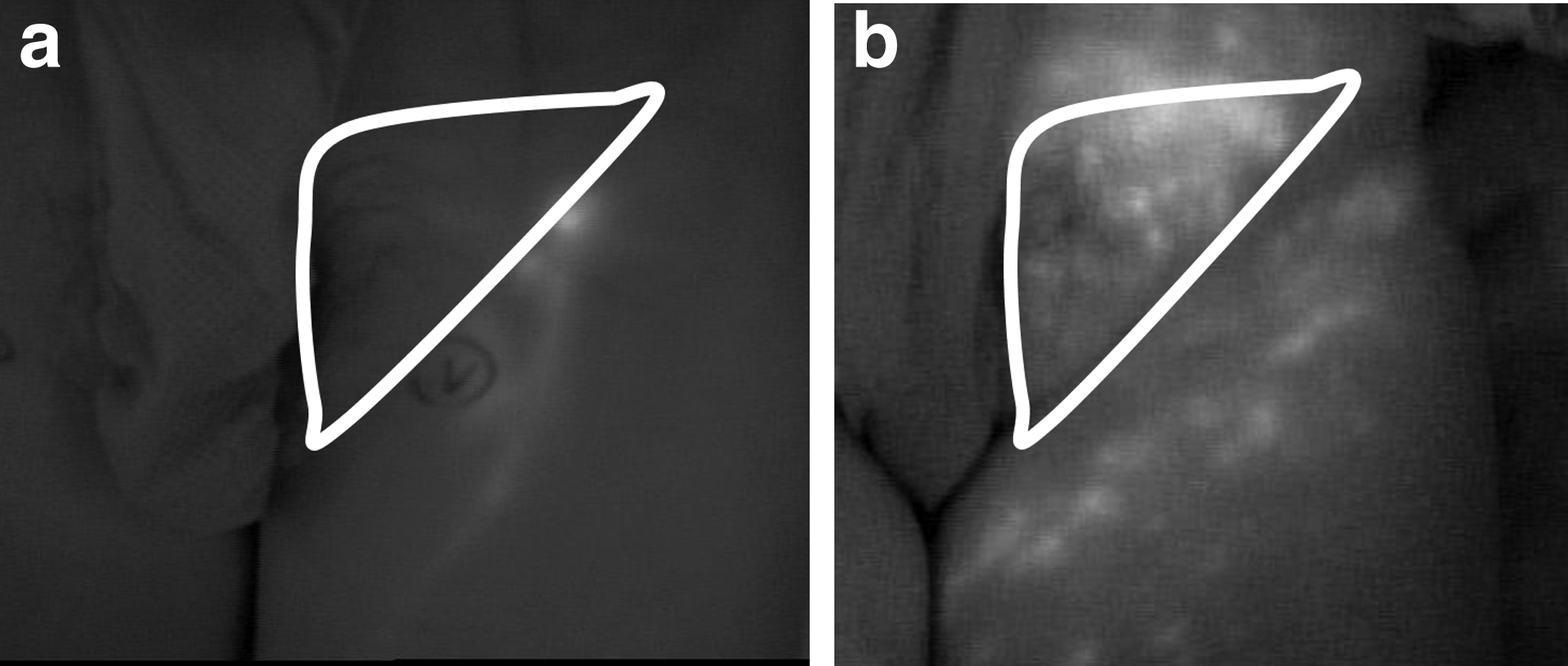
Images of ICG lymphography. White triangle indicates the genital region.
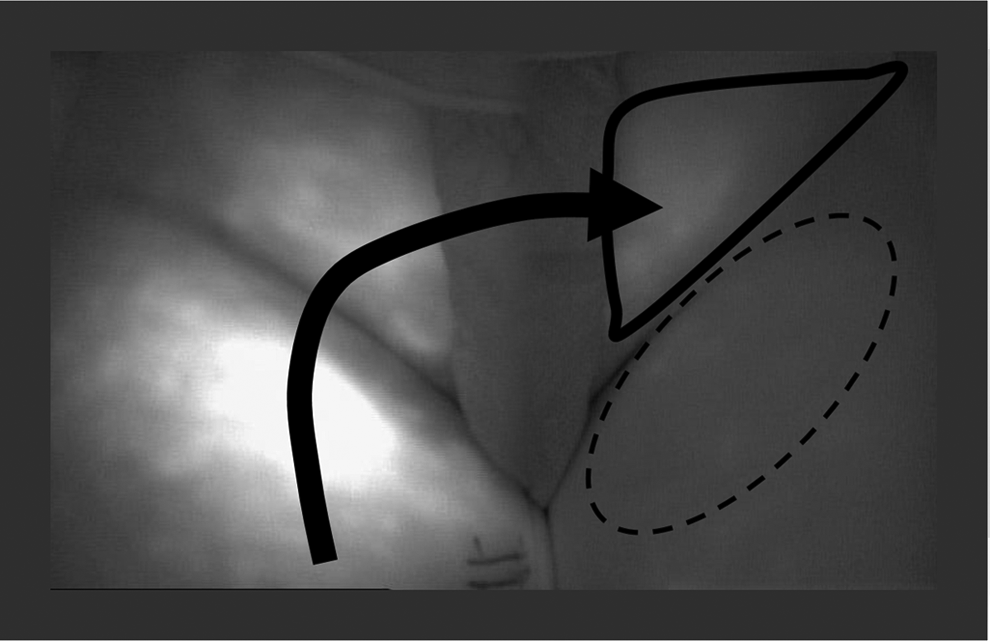
Illustration of lymphatic flow in GPS 1. Dermal backflow is observed in the left genital region (triangle), although there is no dermal backflow in the left inguinal region (circle). The lymphatic stasis in the left genital region flows from the contralateral side (arrow).
Tables 1–3 indicate the relationship between the presence of genital lymphedema and previous treatment for cancer. Chi-square tests showed a significant relationship between prior radiotherapy and the presence of genital lymphedema (p = 0.046).
There was not a statistically significant difference (p = 0.17).
LND, lymph node dissection.
There was a statistically significant difference (p = 0.046).
There was not a statistically significant difference (p = 0.34).
Discussion
In the present study, we performed ICG lymphography and lymphoscintigraphy in patients with lower limb lymphedema to evaluate genital lymphedema. We detected lymphatic flow in the genital region and the lymphatic stasis with both examinations.
Lymphatic flow around the genital region is difficult to understand, especially in lower limb lymphedema patients. In the normal condition, lymph from the genital region flows into the superomedial superficial inguinal lymph nodes. 13 However, in the patients with lower limb lymphedema, lymph flows back from the lower limbs to the genital region via the inguinal lymph nodes due to the closed traffic at the pelvic region, as presented in the current study. Although the lymphatic fluid flowed from the lower limb on the ipsilateral side to the genital region in most patients, there were a few who had lymphatic flow from the contralateral side. Based on these findings, we established GPS using ICG lymphography. We believe that this score is useful in determining the choice of treatment, because the direction of lymphatic flow is essential in the selection of treatment. For GPS 2 or 3, it may be adequate to perform lymphaticovenous anastomosis or lymph node transfer on the ipsilateral side, to reduce the amount of lymphatic fluid flowing into the genital region. For GPS 1, performing these procedures on the contralateral side seems reasonable.
In the current study, sensitivity was higher with ICG lymphography than lymphoscintigraphy. In lymphoscintigraphy, we usually inject isotope in the first web space. In patients with poor lymphatic function in the lower limbs, isotope cannot reach the inguinal or genital region. Due to the radiation exposure, injection of radioisotope in the multiple sites is to be avoided. Therefore, it is impossible to evaluate genital lymphatic stasis in those severe cases. For the same reason, conventional ICG testing is not adequate to evaluate genital lymphedema. 3 We injected additional ICG at the thigh or lower leg in those cases and obtained greater sensitivity. Although ICG lymphography can present only a superficial layer, it is free from radiation exposure and serves clear real-time images. 14
The main limitation of this study was the difficulty in verifying the lack of genital lymphedema. The absence of isotope accumulation or dermal backflow does not mean the lack of genital lymphedema. In this study, six sides had lymphedema in the genital region, without positive findings on physical examination. In those cases, the lymphatic fluid in the genital region seemed to be prevented from draining through the inguinal lymph nodes, although there was no reflux from the inguinal to the genital region. To verify lymphatic stasis in those patients, injection of isotope or ICG in the genital region is necessary.
In conclusion, a pathway from the inguinal lymph nodes to the genital region was observed on lymphoscintigraphy in genital lymphedema. The sensitivity was greater with ICG lymphography than lymphoscintigraphy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.