
Abstract
Abstract
Background:
Lymphedema of the arm and/or hand is a well-established complication of breast cancer therapy. The objective of the study was to determine the interest of auto-adjustable MOBIDERM® Autofit night arm sleeve in controlling edema rebound effect in breast cancer-related lymphedema patients just after a successful intensive phase of decongestive lymphedema therapy (DLT).
Materials and Methods:
This is a subgroup analysis of MARILYN Study, conducted on 40 patients after completion of intensive DLT. Patients were randomized in Night-user group (fitted with MOBIDERM Autofit device) or No night-user group (no night compression). For subgroups analysis, patients were defined as high responders (HR) if their lymphedema volume reduction during DLT was ≥35% or as low responders (LR) if it was below 35%.
Results:
In HR subgroups (n = 16), the mean lymphedema volume variation between Day 0 and 30 was 28.4 mL in the night-user group versus 181.4 mL in the no night-user group. When adjusted to the loss of volume during DLT, 89% of the DLT benefit is maintained in HR night-user versus 54% in no night-user group. Between LR (24 patients), this mean volume variation was by 65.1 mL versus 54.9 mL in night-user and no night-user groups respectively between Day 0 and 30.
Conclusion:
Wearing MOBIDERM Autofit, on top of the day time hosiery, appears a promising way to control the early rebound effect during the maintenance phase especially in DLT-HR.
Introduction
L
Management of lymphedema is based on decongestive lymphedema therapy (DLT), which consists in two consecutive phases: an intensive phase that combines manual lymphatic drainage, multilayer bandages, compression garments, skin care, and physical exercises, to reduce as much as possible lymphedema volume in a short period of time, and a maintenance phase that consists in helping the patient to preserve lymphedema volume reduction, achieved during the intensive phase, as long as possible.3–6
In clinical practice, noticeable differences are seen in patient response to the treatment of breast cancer-related lymphedema (BCRL), but, it is common to observe an increase of lymphedema volume after DLT, known as “rebound effect.” The short-term kinetic of lymphedema volume was not well studied, and no consensus or clinical definition of this “rebound effect” exists. Some authors pointed out the fact that the benefit of DLT was partially reverse few months later. In a long-term trial, Vignes et al. 7 estimated that the risk of treatment failure (i.e., a lymphedema volume increase of ≥50% of the total reduction obtained with the first intensive decongestive physiotherapy) was 38.1%, 53.1%, and 64.8% at 1, 2, and 4 years respectively after DLT. In the observational POLIT study, 5 Quéré et al. showed that the reduction of lymphedema volume by 30% obtained during the intensive phase was partly lost 6 months later. Therefore, optimizing maintenance phase treatment appears to be crucial for long-term management of lymphedema.
Even if the modalities of the maintenance phase are less precise and defined than those of intensive treatment, it's recognized that good compressive strategy is important to maintain and optimize the volume reduction achieved during the DLT phase. Therefore, long term and consistent use of garments or bandages during the night are encouraged and recommended by International Lymphoedema Framework (ILF) and Haute Autorite de Santé (HAS)8,9 in France. It was demonstrated that especially when compression therapy is neglected, the achieved improvement soon goes to waste. 10 Garments are alternatives to bandages that require skills and trained person to be used correctly and to apply the level of pressure needed. No previous study investigates the role of night garment in maintenance phase.
So, we conducted a randomized controlled pilot study (MARILYN) to evaluate the effects of the nighttime auto-adjustable MOBIDERM® Autofit arm sleeve in women with BCRL who had just completed intensive DLT. 11 Results showed that during the first month after DLT (primary endpoint), lymphedema volume increased by 46.7 mL (i.e., median increase 1.8%) in the night-use group while it was two times higher (92.9 mL, i.e., median increase 3.2%) in the no night-use group.
Here, we report subgroups analysis of the MARILYN study based on clinical response to the DLT (high or low responders, as defined in Materials and Methods section). The purpose was to assess the interest of MOBIDERM Autofit in stabilizing lymphedema volume especially in patients who presented an important lymphedema volume reduction during DLT; patients for whom rebound effect risk was high.
Materials and Methods
Ethical approval
The study complied with the protocol and Declaration of Helsinki, and was done in accordance with Good Clinical Practice and regulatory guidelines and relevant local legislation. The protocol received approval from health authorities and ethics committee. Before study start, all patients provided written informed consent (clinical trial number 2014-01008-39).
Study design and study population
The study population consisted of 40 female patients aged ≥18 years old, screened in a single institution at the vascular medicine department of the Saint-Eloi Hospital, Montpellier, France from September 2014 to February 2015. Eligible patient had to have a unilateral BCRL with evident pitting sign (assessed as ++ or +++). All patients had to undergo an intensive phase of DLT, as indicated by the good clinical practice, with a clinically significant decrease of lymphedema volume assessed by clinicians before study entry. Patients were excluded from the study in case of active cellulitis, lymphedema associated with active cancer requiring chemotherapy, motor and/or sensitive neurological deficiency, postoperative edema (i.e., acute edema occurring in the days following breast cancer-related surgery), presence of skin lesions on the arm sleeve placement, and pregnancy or breastfeeding. Patients were analyzed according to their response to DLT phase before randomization.
After the intensive phase of the DLT (Day 0), patients fulfilling the study entry criteria were randomized in a 1:1 ratio to:
• The Night-user group, fitted during the first 30 days WITH MOBIDERM Autofit device additionally to their made to measure day-time THUASNE lymphology® hosiery, a circular knitted garment with a level of pressure from 15–20 mmHg (French class 2) or 20–36 mmHg (French class 3) on investigator's demand. • The No night-user group will be fitted only by their made to measure day-time THUASNE lymphology hosiery during 30 days.
After Day 30 ± 2, all patients in both groups used both their daytime and nighttime MOBIDERM Autofit devices until the end of the follow-up period (Day 90 ± 3).
In each group, patients were also classified according to clinical response to the intensive DLT phase for post hoc subgroups analyses. Patients were considered as high responders (HR) if the lymphedema volume reduction between the initiation of the intensive phase (DLT) and the beginning of maintenance phase (Day 0) was ≥35% and as low responders (LR), if it was lesser than 35% (Fig. 1).
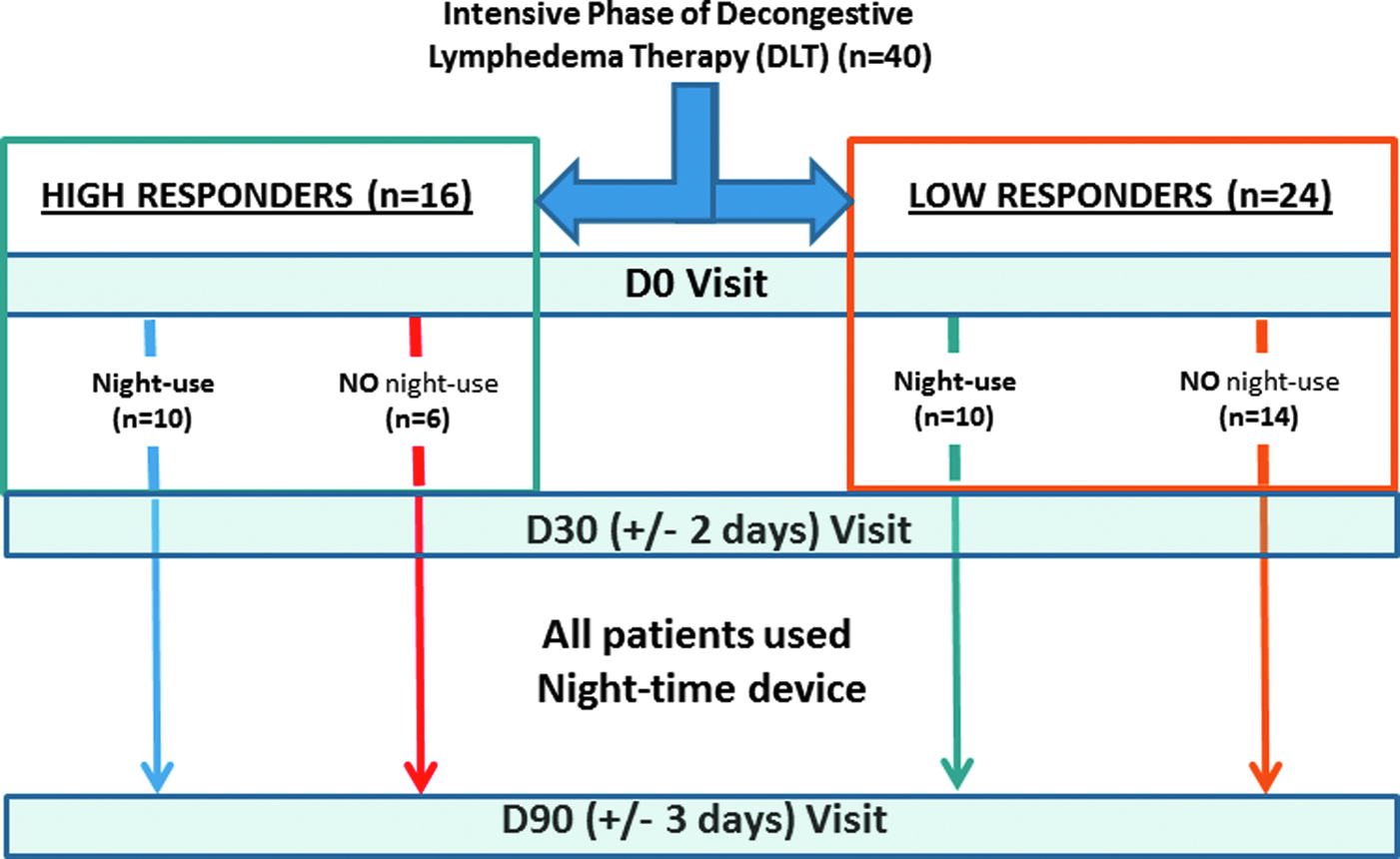
Subgroups analysis.
Description of the medical device tested
The nighttime MOBIDERM Autofit (Thuasne, Saint-Etienne, FRANCE) is a low-stretch, auto-adjustable semi-open sleeve, designed to apply a pressure of 15 mmHg irrespective of patient's morphology. Thanks to several semi-rigid straps, the device can be adjusted to each patient's morphology or volume change. It was supplied to the patients in the corresponding standard references among the 6 sizes, 2 lengths, left/right arm available.
The garment uses the patented MOBIDERM technology composed of foam blocks surrounded by soft adherent webbing. It creates on the skin (and under the skin) zones of differentiated pressures between the foam blocks and their perimeter allowing a local drainage to facilitate edema fluid circulation (Fig. 2).
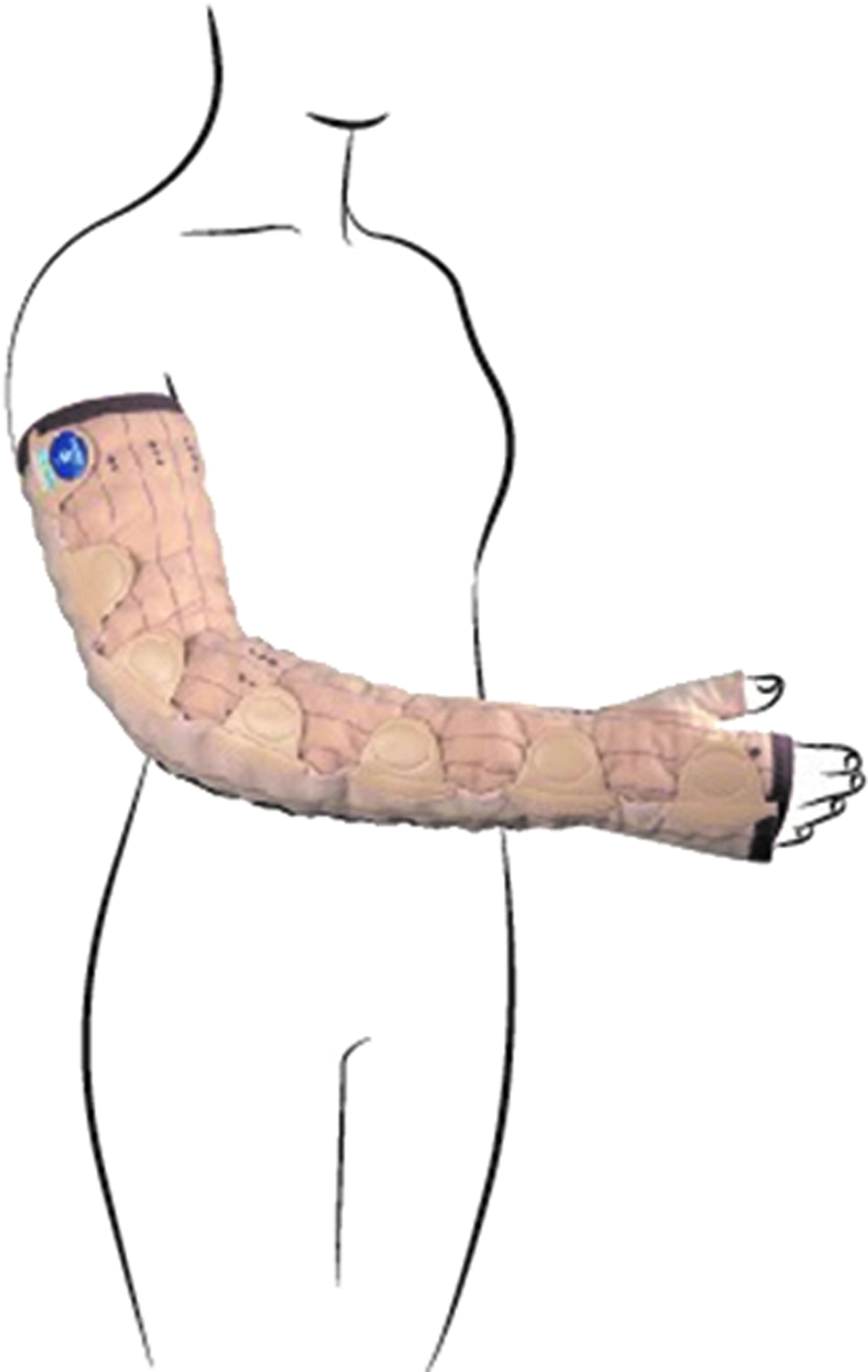
Nighttime auto-adjustable MOBIDERM® Autofit device.
Statistical analysis
Descriptive statistics were used to analyze the lymphedema volume variations (mL) between the different study timepoints (DLT, Day, 0, 30, and 90) defined as the volumetric difference of the affected limb compared to the contralateral upper limb, calculated with truncated cone formula.
Primary results were already presented in the article of Mestre et al. 11
Results
Main baseline demographics and characteristics of lymphedema
A total of 40 patients were included and analyzed (20 patients in each randomized group).
At the end of the DLT, among the randomized Night-user group (n = 20), 10 patients were categorized as HR and 10 as LR while in the randomized No night-user group (n = 20), only 6 patients were defined as HR and 14 as LR.
Patient's demographics and lymphedema baseline characteristics are provided by subgroups of analysis in Table 1. All patients had radiotherapy after their breast cancer surgery. As shown in this table, HR of No night-user group were older (median age of 77 years) as compared to the other subgroups and they also had an older diagnosis of lymphedema before study entry (median time from diagnosis to inclusion was 8 years). In terms of lymphedema characteristics, no significant difference was observed between the LR subgroups at study entry. For HR subgroups, two patients of no night-user group present stage III lymphedema while all HR patients from night-use group had stage II lymphedema. Other baseline demographics were well balanced between the four subgroups.
Lymphedema volume variation according to DLT response
HR lymphedema volume evolution
As illustrated in Figure 3, in both HR subgroups, DLT was effective: mean lymphedema volume decreases by 261.27 mL ±109.01 (i.e., median decrease 39.10%) and 405.07 mL ±287.83 (i.e., median decrease 47.03%) respectively in the randomized night-use and no night-use groups (Table 2). The expected rebound effect during the first month after intensive DLT phase (Day 0–30) was observed only in the no night-use group with an increased lymphedema volume by 181.39 mL ±198.84. In the night-user group, this effect was erased (mean lymphedema volume variation between Day 0 and 30 was 28.36 mL ±90.01) corresponding respectively to maintenance of 55% and 89% of the benefit of the DLT phase (Table 2).
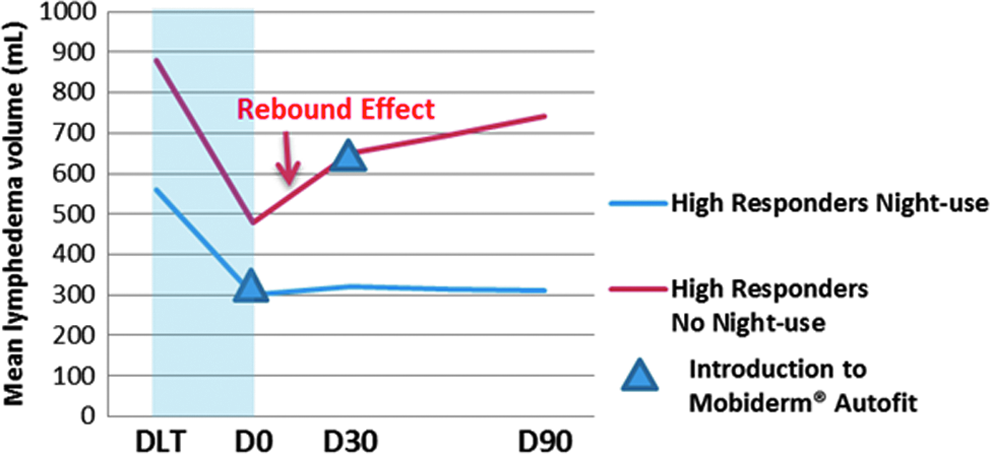
Lymphedema volume variation between high responders to DLT. DLT, decongestive lymphedema therapy.
DLT, decongestive lymphedema therapy.
From Day 30 and 90, after Mobiderm Autofit is introduced and applied to all patients the mean lymphedema volume variation remained stable in the initially randomized night-user group (1.29 mL) and tended to increased more slowly in the randomized no night-user group (92.87 mL).
Considering the volume lost during the DLT, maintenance of this benefit at Day 90 was of 88% and 32% in HR night-user and no night-user subgroups (Table 2).
LR lymphedema volume evolution
Between LR of the two groups, during the Day 0–30 period, the rebound effect was of lesser magnitude, irrespective of groups (Fig. 4 and Table 2). Lymphedema volume increased by 65.12 mL ±108.80 in LR night-user versus 54.91 mL ±190.30 in LR no night-user corresponding to maintenance of 69% and 54% of the benefit of the DLT phase respectively.
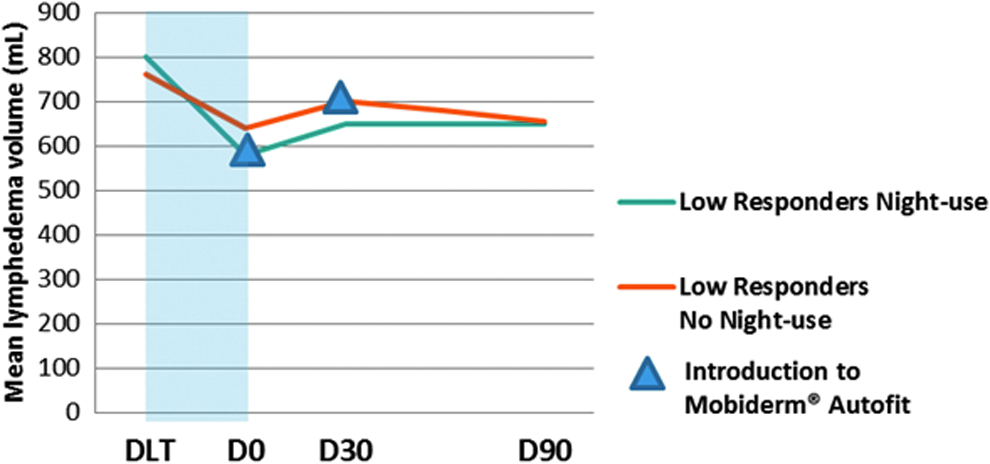
Lymphedema volume variation between low responders to DLT.
From Day 30 and 90, when using the night armsleeve, the mean lymphedema volume was stabilized irrespective of the subgroups analysis: it was of −3.81 and −40.27 mL in the initially randomized night-use group and no night-use group respectively.
Discussion
This study assessed the efficiency of the nighttime MOBIDERM Autofit arm sleeve to control the lymphedema volume in patients suffering from BCRL.
The intensive phase of DLT is a relevant acute treatment only if its effectiveness is maintained over time. Some work suggests that during maintenance phase, there is a risk to observe a rebound effect and/or a rapid loss of DLT benefits.5,7,12 Night bandages are effective but are not unconstrained. So, the interest is to see inpatients with high risk of losing their benefit achieved during the intensive phase, if a night treatment, of easy application, could limit lymphedema volume recovery.
The patients were classified into two subgroups according to the volume of edema reduction at the completion of the initial intensive DLT phase. The evolution of the lymphedema volume during the maintenance phase was analyzed according to the DLT response.
Our results showed that lymphedema volume evolution mainly reflected the introduction of a night compression modality in the treatment, with an effect of DLT maintained to a greater extent. Generally, there is a trend to an increase of lymphedema volume since the first month after the DLT, with an early rebound effect mainly observed in the no night-user group and high DLT responder subgroup.
To date, no consensus for the definition of successful DLT is reached due to the large interpatient variability. Reduction of lymphedema volume after intensive DLT may vary according to the published series between 20% and 80%, depending on the studied populations and the different methods of measurement of lymphedema.12–19
In our study, we defined “High responders” when lymphedema volume reduction between the initiation of the DLT and Day 0 was more than 35%. The threshold of 35% was chosen a priori based on the results of a previous observational study (The POLIT study), which showed a relative median excess volume decrease during intensive DLT phase of 31.0% for patients suffering from either upper limb or lower limb lymphedema. 5 Based on this definition, at the completion of the intensive DLT patients, 50% of patients in night-use group and 30% of patients in no night-use group achieved a high response (16 patients).
We showed in a first time that between DLT-HR, patients fitted with a night sleeve presented a lymphedema volume variation six times lower as compared to those of no night-user patients (28.4 mL vs. 181.4 mL respectively) at 1 month after DLT. Thus, HRs' patients who used night device retained 89% of the initial reduction, whereas in the no night-user group, HRs' patients maintained 54% of the benefit of DLT. The absence of rebound effect in night-use patients during the first month of maintenance phase, suggest an important beneficial effect of the studied night device in controlling the lymphedema volume, right after the completion of intensive DLT phase.
In both LR subgroups we observed a similar and weak lymphedema volume evolution (65.1 and 54.9 mL in LR night-use and no night-use subgroups respectively). This observation confirms that the risk to the failed maintenance phase mainly depends on the DLT response level. Indeed, it was demonstrated that the higher the volume reduction achieved during DLT period is, the higher the risk is to have a rapid increase of the lymphedema volume just after the completion of DLT.7,20 In study conducted by Ramos et al., 21 the authors showed that patients with less edema showed a better response to decongestive treatment (a mean reduction of 78%), and those with more edema showed a worse response (58.9%). In a randomized study enrolling 60 severe postmastectomy upper limb lymphedema, Gradalski et al. 12 observed also a rebound effect within the first month of maintenance therapy. In our study, the rebound effect was restricted in HR of night-use group as compared to those observed in the no night-use group, while between LRs' patients no rebound effect was observed whatever the group. These results first confirmed that the HR DLT patients were particularly sensitive to an important and rapid lymphedema volume recovery, and secondarily suggested that the MOBIDERM Autofit arm sleeve presented beneficial properties to control the rebound effect particularly when the volume mobilized during the intensive phase is high.
Some noticeable demographics and characteristics of lymphedema differences between the subgroups before initiation exist. HR in no night-use group were indeed older and had a longer duration of lymphedema before the initiation of DLT. Older age and chronicity of lymphedema were reported as negative predictive factors of response to DLT, although still controversial. 22 In a study conducted by Vignes et al., 7 the authors found that clinical parameters that were associated with negative outcome were patient's weight and a BMI >30, parameters well balanced in our groups; whereas older age was associated with a decreased risk of treatment failure.
Results discussed in this article confirmed that the main lymphedema volume changes after an intensive phase occur within the first month. Lymphedema volume variation measured between DLT and Day 90 were sensibly similar to those measured between DLT and Day 30, showing a stability of lymphedema volume between Day 30 and 90 in both high and LR.
The main strengths of our study are that it was conducted in a specialized lymphedema center and it was prospective and randomized study including only women with BCRL. Lymphedema volume measurements and follow-up visits were ensured by specific trained physiotherapists. Importantly, the study is the first to show an effect of the use of nighttime garment in the control of the rebound effect after completion of the initial intensive DLT phase. The threshold to defined HR or LR was defined a priori according to POLIT results and before results of MARILYN study.
The study design (Pilot Study) with the sample size (40 patients) is the main limitations of this study. Randomization was not stratified by DLT efficiency to categorized patients in High or LR subgroups. Accordingly to these points, the study was only powered for subgroups descriptive analysis.
It is well known that the study period is crucial in the evolution of the lymphedema, so we believe that our findings could be helpful for the clinicians and patients. Nevertheless, these results should be confirmed in a well-designed phase III study.
In conclusion, based on our observations, wearing a nighttime garment on top of the day time hosiery appears to be a promising treatment modality to control lymphedema volume in patients suffering from BCRL. The night compression device allowed to reduce the risk of rebound effect and stabilized the lymphedema volume during the maintenance phase, especially in HR patients who had the highest volume mobilized during the intensive DLT phase.
Footnotes
Acknowledgments
We thank all the patients who took their time to participate in the study and the team of the Unit of Lymphology, Montpellier University Hospital who allowed this study to take place in the best conditions. We specially thank our caregivers: Fabienne Mourgues, Florence Delseny, and Hélène Pourquier et Véronique Bouys.
Author Disclosure Statement
S.M.: Reports personal fees from Thuasne laboratory, during the conduct of the study (support for travel to meetings for the study or otherwise). G.G., M.B., V.S.-S.: No competing financial interests exist. M.P., C.B.A.: Working at Thuasne, sponsor of the study. I.Q.: Reports grants, nonfinancial support, personal fees, and other from Thuasne laboratory, for the University Hospital of Montpellier and herself, during the conduct of the study.