
Abstract
Abstract
Background:
Lymphedema may affect patients' health-related quality of life (HRQoL) and thus a disease-specific questionnaire is needed. The Lymphedema Quality of life Inventory (LyQLI) has been tested for reliability and validity. The purpose of this study was to test the LyQLI for responsiveness and sensitivity.
Methods and Results:
The study participants were patients with lymphedema in the upper or lower limb, attending a Swedish rehabilitation program (RP) and undergoing conservative treatment without surgery (RP-sample), or undergoing liposuction (LS) in Australia, Scotland, and Sweden (LS-sample). Mean values for the three LyQLI domains (physical, psychosocial, and practical) were calculated before and 1 month after intervention, and the paired t-test was used to detect group differences. Responsiveness was calculated using standardized response mean (SRM), and sensitivity was analyzed with box plots and an independent t-test to detect group differences. Eighteen patients in the RP-sample and 50 in the LS-sample were studied, and both samples demonstrated increased HRQoL after intervention. The changes were significant in all domains, except for the practical domain in the RP-sample. The SRM for the three LyQLI domains (physical, psychosocial, and practical) were 0.8, 0.8, and 0.4, respectively, in the RP-sample and 0.7, 1.2, and 0.9 in the LS-sample. Statistical testing indicated that the LyQLI was sensitive enough to reveal differences between patient groups.
Conclusions:
LyQLI responsiveness and sensitivity indicated that the tool can be used to evaluate patients undergoing conservative or surgical lymphedema treatments.
Introduction
L
Lymphedema is commonly treated with complex decongestive therapy (CDT) that usually compromises manual lymphatic drainage, multilayer limb bandaging, compression garments, skin care, and exercises to enhance lymphatic pumping, but may also include other components.2,3 Lymphedema leads to early deposition of adipose tissue. While CDT can remove accumulated lymph fluid, it has no effect on the fatty component of the swelling. Once the lymphedema has reached the nonpitting stage and no further reduction can be achieved with CDT, liposuction (LS) can be performed if the excess volume remains a problem. LS is a surgical method that, together with use of compression garments, reduces edema volumes rapidly and effectively.4–6
Several researchers have investigated the influence on health-related quality of life (HRQoL) in upper limb lymphedema (ULL) after breast cancer treatment using patient-reported outcome (PRO) instruments. Hoffner et al. used SF-36 for LS of ULL and concluded that generic questionnaires like SF-36 cause a potential bias, and that disease-specific questionnaires are more accurate than global HRQoL assessments. 7 Pusic et al. found that only two of 17 PRO instruments reviewed were lymphedema specific. 8 Findings were similar for HRQoL in patents with lower limb lymphedema (LLL) after endometrial or head and neck cancer treatment.9,10 Study-specific questionnaires examined HRQoL in gynecological cancers survivors11–13 with questions about the lymph system, and all showed a negative impact of lymphedema on HRQoL.
Using disease-specific PRO instruments may show intervention-related changes in HRQoL more precisely. 14 Important features of a PRO instrument are validity and reliability, as well as sensitivity and responsiveness. 15 Lymphedema-specific HRQoL instruments have recently been developed,16–19 but they target one specific part of the body and thus make it difficult to compare different patient groups. Thus, an HRQoL instrument that is lymphedema specific, rather than body part specific, is needed. The Lymphedema Quality of life Inventory (LyQLI) is a lymphedema-specific PRO instrument that measures HRQoL in patients with lymphedema in various parts of the body, available in English and Swedish. It has been developed and tested for reliability and validity. 20
Aims
The primary purpose of this study was to evaluate the responsiveness of LyQLI. A secondary purpose was to evaluate sensitivity by comparing different patient groups. To evaluate responsiveness, two treatment concepts were used:
(1) Rehabilitation program (RP) conducting conservative lymphedema treatment in patients with mild/moderate/severe ULL or LLL. (2) LS in patients with moderate/severe ULL or LLL.
We hypothesized that:
(a) The internal responsiveness would be larger in the LS-sample than the RP-sample. (b) The domain scores in LyQLI would show larger internal responsiveness than global items 44 and 45 not included in the domains. (c) The external responsiveness would show that a decrease in perceived tension/heaviness would correlate to an increase in HRQoL and a reduction of limb volume in the affected limb would correlate to an increase in HRQoL, at least to some degree in each case. (d) Patients eligible for LS would estimate their HRQoL lower than other lymphedema populations because of larger excess volumes.
Materials and Methods
The evaluation of LyQLI responsiveness was based on a multi-center intervention study of two different treatment concepts in three countries. To evaluate sensitivity, the two treatment samples were compared to each other and to a reference lymphedema population from a previous study. 20
The patients' characteristics are shown in Table 1.
Reference lymphedema population from prior cross-sectional study.
p < 0.001, differences in excess volume were calculated with independent t-test.
p < 0.05, differences in affected limb volume were calculated with independent t-test.
SD, standard deviations.
Ethical approvals
All procedures performed in studies involving human participants were in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Australian part was approved by the Macquarie University Human Research Ethics Committee (HREC [Medical Sciences]), Reference No: 5201400124. The Swedish part of the study was approved by the Research Ethics Committee, Lund University, Lund, Sweden, Dnr 2013/628 and 2014/208. No ethical approval was required for the Scottish part of the study. Informed consent was obtained from all individual participants in the study.
Rehabilitation program
Patients diagnosed with ULL or LLL at Bräcke diakoni Rehabcenter Sfären, Solna, Sweden, were invited to the study when they registered for a 2- or 3-week RP. The program included the most common components of CDT, 2 expanded with relaxation, weightlifting, and water-based exercise, education about the lymph system, and ergonomic and self-care. Inclusion criteria were adults, 18 years or older diagnosed with lymphedema, and with no previous RP. Patients with concurrent cancer disease or cognitive or communication difficulties were excluded.
Liposuction
Study participants were patients with ULL or LLL undergoing LS 21 for management of lymphedema through the Macquarie University Advanced Lymphedema Assessment Clinic in Sydney, Australia, the Plastic Surgery Clinic at Ninewells Hospital in Dundee, Scotland, and the Department of Plastic and reconstructive Surgery, Skåne University Hospital, Malmö, Sweden.
Reference lymphedema population
In a previous study by Klernäs et al. 20 200 outpatients were selected from the registers of two lymphedema units in Sweden: Skåne University Hospital, Lund (n = 100), and Bräcke diakoni, Rehabcenter Sfären, Solna (n = 100). Patients were allocated to three subgroups by strategic selection: secondary ULL/head and neck (n = 80), secondary LLL/genitalia (n = 60), and primary lymphedema (n = 60). The selection was consistent with the incidence of lymphedema at both clinics, based on the patient register. Inclusion criteria were adults, 18 years or older, diagnosed with lymphedema for at least 6 months. Patients with concurrent cancer disease or cognitive or communication difficulties were excluded. A sample of 129 patients (64%) completed the LyQLI. 20
Measurements
Lymphedema Quality of Life Inventory
The LyQLI (Supplementary Data; Supplementary Data are available online at www.liebertpub.com/lrb) is a self-managed questionnaire that assesses HRQoL in lymphedema patients. It comprises 45 items. Forty-one items are divided into three multi-item domains: physical (12), psychosocial (16), and practical (13). For each item, the impact of lymphedema over the last 4 weeks is assessed on a 4-point Likert scale (0: None, 1: A little bit, 2: Somewhat, 3: A lot). Scores are presented as the mean for each domain, ranging from 0.0 to 3.0. A higher score indicates lower HRQoL. The questionnaire also includes four global questions, of which item 44 assesses the overall experience of lymphedema and item 45 the overall quality of life, both on a 4-point Likert scale ranging from 0: Very bad to 3: Very good. A higher score indicates higher HRQoL. The LyQLI has previously been tested in lymphedema patients in Sweden. Face, content, and concurrent validity, test-retest reliability, intra-class correlation coefficient (ICC), and Cronbach's alpha were all sufficient. The ICC for the physical and psychosocial domains was 0.88 and 0.87, and 0.87 for the practical domain. Cronbach's alpha for the three domains was 0.88, 0.92, and 0.88, respectively. 20
Clinical-sociodemographic questionnaire
Participants provided their characteristics, and lymphedema and medical history through hard copy surveys or a website link.
Visual analogue scale
The subjective experience of lymphedema symptoms in the affected limb was scored by each patient on a 100 mm horizontal visual analogue scale (VAS). Patients were asked to evaluate their average and least and worst experience of tension and heaviness during the past week. The endpoints were “no discomfort” (0 mm) and “worst imaginable discomfort” (100 mm).22,23 Because VAS measurements were repeated, the initial scores were made available to the patient at the second test. 24
Cylinder form method
Extremity volumes were calculated on each occasion using the cylinder form method, with circumferential measurements taken at 4-cm intervals and the contralateral arm/leg as control. 25 This method has been assessed as valid. 26 Sander et al. 27 found strong inter-rater and intra-rater reliability for both water and geometric volumes.
Truncated cone method
Extremity volumes were calculated on each occasion using the truncated cone method, with circumferential measurements taken at 4-cm intervals and the contralateral arm/leg as control.28,29 This method has been assessed as reliable and valid. 28
Water displacement method
Extremity volumes were measured with the water displacement method (WDM). 30 Bednarczyk et al. carried out a validity test for this method with a computerized limb volume measurement system and found a high correlation coefficient (r = 0.992). 31 Each arm/leg was submerged in a container of water on each occasion and the volume displacement was expressed in milliliter, with the contralateral arm/leg as control. 29
Procedure
Rehabilitation program
Patients were invited to the study as part of their routine invitation to attend the planned RP about 3 weeks before their appointment. The first author (P.K.) contacted the patients by telephone, and if they agreed to participate, they were sent the LyQLI, a consent form, and a clinical-sociodemographic questionnaire, with a request to return it before RP. On day 1 at the clinic, limb volume was measured using the cylinder method. 25 The patient's reported experiences of heaviness were recorded and tension of the affected limb determined using the VAS.22,24 The same parameters were measured on the patient's last program day. One month later, the patients received and answered the LyQLI by mail. The data were collected by PK who was not involved in the treatments.
Liposuction
About 3 weeks before LS, the patients received information about the study and were invited to participate. In Australia, a research assistant sent information to eligible patients by post or email describing the research aims. To take part in the study, the patients completed the consent form, the clinical-sociodemographic questionnaire, and the LyQLI either online or through a card copy. In Scotland, patients received the LyQLI questionnaire in the morning, 4 hours before surgery. In Sweden, the patients received information about the study at their visit 2 weeks before surgery and were then contacted by telephone by P.K., and asked to participate. If they agreed, they were sent the LyQLI, a consent form, a clinical-sociodemographic questionnaire by mail with a request to return it before surgery.
Limb volumes were recorded as a regular part of care within the clinics. Volumes were measured using the truncated cone method28,32,33 in Australia and Scotland, and WDM in Sweden.29,30 One month after LS, the patients completed the LyQLI either in hard copy or online through a website link. The surgeons were not involved in data collection.
Statistical analysis
Two methods were used to evaluate responsiveness: internal responsiveness, which measures the ability to detect changes over a prespecified time frame, for example, before and after an intervention, and external responsiveness, which compares a measurement to a corresponding clinical measurement to detect important clinical changes. 34
Descriptive statistics were calculated for the sample groups. Mean values, range, and standard deviations (SD) were calculated for the total limb volume and excess volume (affected limb–unaffected limb) in milliliter. Baseline differences in total limb volume and excess volume between the RP-sample and the LS-sample were calculated with an independent t-test. Mean values and SD were calculated for the LyQLI responses in the three domains and for item 44 (overall experience of lymphedema) and item 45 (overall quality of life), when missing data did not extend beyond 50%. 15 The paired t-test was used to detect significant differences at baseline and 1 month after. For the VAS measurements, mean values at baseline and after intervention were calculated.
Floor and ceiling effects
Floor and ceiling analysis was conducted by calculating the number of patients with possible minimum ( = 0) and possible maximum ( = 3) scores in both interventions in each domain, and as a total for the 41 items.
Responsiveness
To determine internal responsiveness, effect size was calculated as the standardized response mean (SRM). The SRM uses the variation in changes 15 and is widely used to evaluate responsiveness. SRM = response mean/response SD.14,34 According to Cohen, 35 the categorization of SRM is <0.50, small; 0.50 to 0.79, moderate; and ≥0.80, large. The SRM for each domain and global items 44 (overall experience of lymphedema) and 45 (overall quality of life) was calculated in both interventions. To evaluate external responsiveness, Pearson's correlation coefficient was used. Changes in LyQLI responses before and 1 month after intervention were correlated to changes in experience of tension and heaviness in RP-samples, and the LS-sample, to the reduction of limb volume in the affected limb. The correlations (r) <0.30 were considered low; 0.30 to 0.49, moderate; and ≥0.50, strong. 35
Sensitivity
Sensitivity was analyzed by calculating the differences in baseline response between the RP- and LS-samples in each domain, using the independent t-test. Further investigation was conducted using box plots of the baseline response from the reference lymphedema population and the two current samples.
All statistical analyses were two tailed with a significance value of 0.05.
Results
Rehabilitation program
Twenty patients fulfilled the criteria and completed the first measurement and 18 patients completed the second measurements. Patient characteristics are presented in Table 1. Two patients did not complete the second measurement, one because of cancer recurrence and the other because of trauma. Eighty-three percent of the study sample were females. Seventy-eight percent had secondary lymphedema, 99% of whom had lymphedema secondary to cancer treatments. Most of the patients had ULL, with breast cancer treatment being the most common underlying cause. Mean excess volume before and after intervention was 934 (1398) mL (range 186–6240) and 708 (1339) mL (range 43–5863), respectively (p = 0.032). Mean affected limb volume before and after intervention was 6885 (5668) mL (range 2622–23533) and 6554 (5560) mL (range 2526–23318), respectively (p = 0.008).
Liposuction
Fifty-six patients fulfilled the criteria and completed the first measurement before LS, and 50 patients completed the second measurement. Patients' characteristics are presented in Table 1. Four patients did not respond to the second measurement, with no reason given, and one patient gave a general lack of vigor as a reason. The sixth patient did respond, but failed to complete the measurement. Ninety percent of the study sample were females. Seventy percent had secondary lymphedema, 98% of whom had lymphedema secondary to cancer treatment. Most patients had LLL, with melanoma, or ovarian or cervical cancer treatment being the most common underlying cause. Mean excess volume before and after intervention was 3137 (2679) mL (range 586–12567) and 972 (1141) mL (−210 to 4227), respectively (p < 0.001). Mean affected limb volume before and after intervention was 10450 (5452) mL (range 2997–24166) and 8464 (4148) mL (range 2064–16425), respectively (p < 0.001).
Floor and ceiling effects
The results from the total 41 items showed that in the RP-sample, the possible minimum ( = 0) and maximum ( = 3) scores were 34% and 15%, respectively, at baseline and 44% and 6% after intervention. In the LS-sample, the corresponding scores were 22% and 26% at baseline and 40% and 8% after intervention. The results from the domains showed similar results (data not shown).
Responsiveness
The mean scores for the three domains decreased significantly (indicating higher HRQoL) in both interventions, except for the practical domain in the RP-sample. The mean scores for item 44 and 45 increased (suggesting higher HRQoL), but significantly only in the LS-sample (Table 2). The results for internal responsiveness in the three domains and two overall items are shown in Table 2. For the RP-sample, the SRM was large (>0.80) in the psychosocial domain, moderate (<8.0) in the physical, and small (<0.5) in the practical. 35 In the LS-sample, the SRM values were mainly higher: large (>0.80) in the psychosocial and practical domains, but moderate (<0.80) in the physical domain. The SRM values for item 44 and item 45 were small (<0.50) in both samples. 35
Paired t-test was used to detect the p-values. Item 44 = “overall experience of lymphedema.” Item 45 = “overall quality of life.”
Negative sign implies decrease in score after intervention, meaning higher HRQoL.
Positive sign for items 44 and 45 implies increase of score after intervention, meaning higher HRQoL.
HRQoL, health-related quality of life; LyQLI, Lymphedema Quality of Life Inventory.
The results for external responsiveness are shown in Table 3. The correlation between decrease in LyQLI responses and decrease in average tension and least tension in the RP-sample varied from low (r < 0.30) to strong (r > 0.50), 35 with significant results in least tension in the physical and psychosocial domains. The correlation with experiences of heaviness was smaller (data not shown). The correlation between limb volume reduction and decrease in LyQLI responses in the LS-sample was low (r < 0.30). 35 Some patients with a large limb volume reduction rated their HRQoL lower after intervention, while some patients with a small reduction rated their HRQoL higher (data not shown).
Correlations were calculated with Pearson's correlation coefficient.
Sensitivity
The independent t-test showed differences between LyQLI baseline responses in the two samples (RP and LS) within the physical (p = 0.194), the psychosocial (p = 0.141), and the practical (p = 0.036) domains. The results from the box plot calculations are shown in Figures 1–3. The ends of the whiskers in the box plots represent the minimum and maximum values and outliers are plotted as individual points.
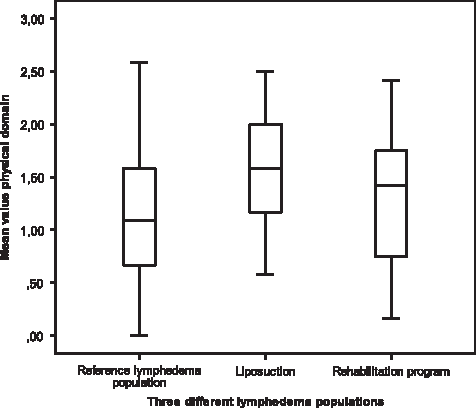
Differences in mean scores at baseline in the physical domain of LyQLI between the three lymphedema samples: Reference lymphedema population, liposuction-sample, and rehabilitation program sample. LyQLI, Lymphedema Quality of life Inventory.
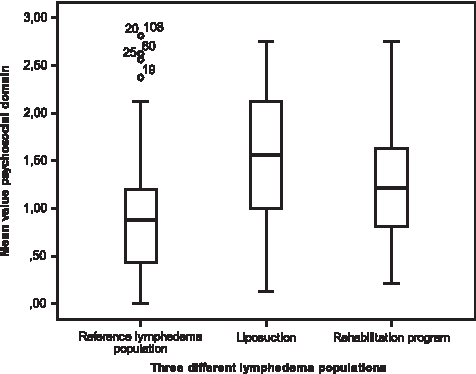
Differences in mean scores at baseline in the psychosocial domain of LyQLI between the three lymphedema samples: Reference lymphedema population, liposuction-sample, and rehabilitation program sample. LyQLI, Lymphedema Quality of life Inventory.

Differences in mean scores at baseline in the practical domain of LyQLI between the three lymphedema samples: Reference lymphedema population, liposuction-sample, and rehabilitation program sample. LyQLI, Lymphedema Quality of life Inventory.
Discussion
Responsiveness and sensitivity are essential for evaluating interventions and longitudinal studies.15,34 The results in this study confirm the responsiveness and sensitivity of LyQLI.
Samples
In total, 76 patients agreed to participate in this multicenter study. Only eight failed to complete the second measurement, giving a response rate of 89%. This is considered a high response that eliminates confounding. In this study, all kinds of lymphedema patients were represented.
Design
The measurements in the RP-sample were conducted at different occasions. The intention was to measure HRQoL similarly in both samples, that is, 1 month after intervention. However, we did not find it defensible to measure volume and VAS as late as 1 month after the rehabilitation, by practical reasons. However, we do not believe that these circumstances interfered with the results.
The LS-sample was collected from three different clinics in three different countries, which make it difficult to ensure the same time schedule for the presurgery measurement, even though the same study program was used. The circumstances that the Scottish patients got their questionnaire just 4 hours before surgery could have influenced the results. If so, probably in the direction that their HRQoL presurgery was higher than it should have been otherwise because the patients may have felt more confident that close to the surgery. However, the results did show a high responsiveness, anyway.
Floor and ceiling effects
The results in both samples showed that the maximum possible score was highest at baseline and decreased 1 month after intervention. As expected, the results were reversed for the minimum possible score. The fact that a relatively high percentage recorded a zero score may reveal a floor effect. However, the relatively high zero score at baseline indicates that the instrument included concerns and symptoms that not all patients experienced. After intervention, the zero score rose even higher, indicating that both patients' health and HRQoL improved. For a disease-specific PRO, it is important to include even relatively rare symptoms that not all patients will experience; so this will not be considered a floor effect. 15 However, since the LyQLI is quite extensive, including 41 items, probably some rare symptoms are redundant and can be deleted to shorten the questionnaire, which may reduce the burden for the patients to complete it. Considering that 26% of the LS-sample scored the maximum score at baseline may imply a ceiling effect. However, the results from the box plot calculations demonstrated that floor and ceiling effects were negligible.
Responsiveness
The primary aim of the study was to examine the responsiveness and we used two different treatments to achieve this. One was LS, which reduces excess volume quickly and in large amounts, 36 so the expected responsiveness is high. The other was an extended conservative treatment program, including the components of the CDT concept. In CDT, excess volume reduction is often more modest, but still significant 2 ; so a lower level of responsiveness is expected.
Our first hypothesis (a) that the SRM would be higher in the LS-sample and the LS-sample should show higher internal responsiveness than the RP-sample was supported by the results. We demonstrated that the SRM was “small” in the practical domain, “moderate” in the physical, and “large” in the psychosocial domain in the RP-sample. In the LS-sample, the SRM was “large” in the psychosocial and practical domains and “moderate” in the physical domain. 35 Since these sample sizes were relatively small, a moderate to large SRM implies an important clinical change. 15
Our second hypothesis (b) was that the domain scores in both samples should show a higher internal responsiveness than the global items 44 and 45. The SRM for these two items was “small” in both samples. The SRM in all domains was “moderate” to “large,” except for the practical domain in the RP-sample. 35 The hypothesis that a domain of several items would be more sensitive than a single item was supported by our results.
Our third hypothesis (c) was that external responsiveness would be at least moderate, that is, a decrease in perceived tension/heaviness would correlate moderately with an increase in HRQoL, and a reduction in limb volume would correlate moderately with an increase in HRQoL.
In the RP-sample, we found a “moderate” to “strong” correlation 35 between a decrease in perceived tension/heaviness and an increase in HRQoL. The correlations particularly in perceived tension were significant in two domains. These results indicate that hypothesis (c) was supported in the RP-sample for perceived tension. However, the relatively small sample size (n = 18) may be a limitation. Since both VAS and LyQLI are subjective measurements, it is plausible that they would correlate.
We chose to calculate the reduction of the volume of the affected limb instead of reduction of excess volume, as often applied. This procedure was used because, in particular, in the lower limb, a healthy side for comparison cannot be guaranteed. The reduction in limb volume and the increase in perceived HRQoL in the LS-sample were significant; however, the correlation between the two variables was considered low (r < 0.3). 35 Therefore, our hypothesis (c) that the two variables should have at least a moderate correlation was not supported. Similar results were found in other studies.37,38 Noh et al. 38 found that patients with LLL estimated HRQoL higher than patients with ULL after CDT treatments, even though there were no differences in the excess volume reduction. In the LS-sample, patients with LLL dominated (68%) and it is possible that the most important issue for these patients was to be taken seriously and cared for. 39 The fact that some patients with a small limb volume reduction nevertheless experienced higher HRQoL after intervention may illustrate this. However, in a longer follow-up, the correlations may be higher. 4
Sensitivity
The second aim of this study was to examine whether the LyQLI can discriminate between different groups of patients. We hypothesized (d) that patients eligible to undergo LS would score HRQoL lower than other lymphedema patients because they often have larger excess volumes resistant to CDT due to excessive fat deposition. Two calculations were made to investigate this. First, the baseline LyQLI responses in the RP- and LS-samples were compared. The results showed a difference, with higher scores in the LS-samples indicating lower HRQoL in the three LyQLI domains. However, the result was only significant in the practical domain (p = 0.036).
Therefore a second analysis was conducted, where we used the baseline data in LyQLI responses to discriminate between the LS-sample, the RP-sample, and the reference lymphedema population comprising outpatients from a cross-sectional study. 20 The box plots showed a difference between the three groups. In particular, the LS-sample seems to have higher scores, that is, they rated HRQoL lower than the two other samples. All samples ranged widely, indicating a large difference in experienced HRQoL between individual patients in all groups, as well as the fact that the LyQLI questionnaire can handle these differences. In conclusion, hypothesis (d) was supported by the results, demonstrating that the LyQLI questionnaire appears to be sensitive enough to detect differences between patient groups.
Strengths and limitations
One strength of our study was the use of different interventions and samples with different characteristics to evaluate responsiveness and sensitivity of the LyQLI. Patients with lymphedema in lower or upper limb and with secondary or primary lymphedema were represented, as well as patients with small, moderate, and severe excess volumes. The circumstances that no patients with lymphedema in head/neck, genitals, or other parts of the body were included can serve as a limitation. To evaluate LyQLI responsiveness and sensitivity in patients with lymphedema in other parts of the body, further studies have to be performed.
Another strength is that the three countries involved demonstrated the possibility of using LyQLI in further international studies. Despite the relatively small sample sizes, LyQLI was both responsive and sensitive.
Conclusions
LyQLI responsiveness and sensitivity indicated that the tool can be used to evaluate patients undergoing conservative or surgical lymphedema treatments.
Footnotes
Acknowledgments
This study was funded by the Swedish Cancer Foundation (Grant No. CAN 2013/629) and the patient organization, Swedish Edema Association. The authors are grateful to all the patients who took part in this study and our clinical colleagues for their assistance and support. We also thank Caleb Winch, research assistant at Macquarie University, for review of the English version of the instrument.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.