
Abstract
Abstract
Background:
Recent studies, mainly on animal models, have suggested that negatively charged glycosaminoglycans, macrophages, and lymph vessels in the skin interstitium may serve as extrarenal control of sodium balance and blood pressure. The aim of the study was to prove the hypothesis that skin interstitium has a role in the pathogenesis of hypertension in humans.
Methods and Results:
We have examined skin biopsies in 91 patients from the department of surgery who had elective surgery with abdominal skin incision: 43 were hypertensive, 14 had resistant hypertension, and 34 with normal blood pressure as control group (median patients' age in these groups estimated accordingly 64 vs. 64 vs. 61.5; p > 0.05). We have studied (1) the content of Na+, water, accumulation of macrophages (CD68), and density of lymphatic vessels (D2-40) and blood vessels (CD31) in the specimens of abdominal skin taken at the time of surgery and (2) plasma NT-proANP, vascular endothelial growth factor (VEGF)-C, and VEGF-D concentrations. The study groups differed in skin expression of CD68 (control vs. hypertension vs. resistant hypertension groups were accordingly: 3.33 vs. 4.00 vs. 8.33; p = 0.005) and in serum concentration of VEGF-C (5792 vs. 4348 vs. 3974 pg/mL; p = 0.026). Differences among groups in plasma NT-proANP levels were close to statistical significance (p = 0.056).
Conclusions:
Our results confirm that skin interstitium may be involved in the pathogenesis of essential hypertension in humans. Lower levels of VEGF-C in hypertensive groups suggest that impairment of lymphangiogenesis and protective function of the skin lymphatic system may play a role in the pathogenesis of hypertension.
Introduction
P
Although numerous studies have shown an adverse effect of sodium (Na+) on arterial pressure, the precise understanding of how excessive sodium consumption triggers the rise in blood pressure remains elusive. Moreover, blood pressure response to a higher versus a lower dietary salt intake varies among individuals and forms a Gaussian distribution in the population.5,6 The degree of these responses to moderate increase of salt intake can be grouped into categories of salt sensitivity and salt resistance.1,6,7 Salt sensitivity becomes more prevalent with age5,6 and its occurrence was generally estimated for ∼50% of hypertensive individuals and for 20% of normotensives.8,9 The measurement of salt sensitivity remains problematic and difficult to apply in a clinical setting, due to the complexity, length of the dietary intervention, and required good compliance of studied patients.10,11 Recent data suggest that NT-proANP1–30 (the N-terminal fragment of the atrial natriuretic peptide prohormone, NT-proANP) may serve as a good marker of salt sensitivity.12,13
Traditionally, the development of salt-sensitive hypertension has been explained by the paradigm of “renal affair.” 14 This view is based on a still widely accepted two-compartment model of sodium balance in which kidneys are the most important organs that control total body sodium, body fluid content, and blood pressure. According to this concept, Na+ is thought to be restricted mainly to intravascular and interstitial space, to hold water in this extracellular space and by its osmotic activity to control the intravascular and interstitial fluid volume.15,16
However, long-term studies with constant sodium intake have shown large fluctuations in diurnal sodium excretion, arranged in weekly and longer rhythms with no correlation with sodium intake. There were rather correlations between sodium excretion and aldosterone and cortisol excretion, independent of blood pressure and body water content. 17
Recent studies conducted by Titze et al. demonstrated that the body sodium distribution should be considered a three-compartment model with skin interstitium as the third compartment. Experiments on rats have shown that Na+ in the skin interstitium can be stored in osmotically inactive form bonded to glycosaminoglycans (GAGs).18,19 GAGs seem to provide an actively regulated interstitial Na+ exchange mechanism that participates in volume and blood pressure homeostasis.20,2123Na magnetic resonance imaging ( 23 Na MRI) assessment of the human body's sodium distribution showed that sodium is accumulated mainly in the skin and muscles.22,23
Rats fed high-salt diet accumulated Na+ within skin GAGs with increasing skin interstitial tonicity. Macrophages infiltrating the skin in response to local hypertonicity expressed tonicity-responsive enhancer binding protein (TonEBP). TonEBP upregulates transcription of vascular endothelial growth factor-C (VEGF-C)19,24 and endothelial nitric oxide synthase (eNOS).24,25 VEGF-C and eNOS stimulate lymphangiogenesis.24,26 Macrophage-driven lymphangiogenesis and increased eNOS production may be seen as buffering mechanisms maintaining blood pressure in the states of high salt load. It has been presumed that new and hyperplastic lymph vessels enable increased lymph capillary transport capacity of sodium, and increased NO production results also in local vasodilatation that may compensate extracellular Na+ and volume retention.24,25 Inhibition of these buffering mechanisms in the skin of rats on high-salt diet (by macrophage depletion or inhibition of VEGF-C signaling) led to increase in extracellular water volume and blood pressure. 25
Moreover, recently it has been demonstrated that high-salt diet modulated the mechanical activity of afferent and efferent collecting lymphatics on animal models, suggesting adaptation of lymphatics to high-salt conditions.27,28 Although the mechanism of such functional adaptation seems to be complex, 29 VEGF-C might be also involved in mechanisms that stimulate lymphatic pump activity. 27
The presented model of extrarenal control of Na+, body volume, and blood pressure in the skin interstitium provided by macrophages—lymphangiogenesis regulatory pathway at present, has been fully established on animal model. The study was designed to prove the hypothesis that the regulatory processes in the skin interstitium are involved in the pathogenesis of essential hypertension in humans.
From several markers developed recently that allow lymphatic endothelial visualization, including D2-40/podoplanin, VEGFR-3, LYVE-1, and prox-1 antigens, we used D2-40 as the most specific and selective marker for lymphatic phenotype. D2-40 is a monoclonal antibody directed against podoplanin, which is a transmembrane mucoprotein expressed in lymphatic endothelial cells. 30
In our study, in addition to serum VEGF-C, we also evaluated serum VEGF-D. VEGF-C and VEGF-D are the most potent lymphangiogenic factors. They are necessary for the lymphatic vessels growing during development and in the adult they are essential in both physiological and pathological processes. 31
Materials and Methods
Patients and controls
The study group included 91 patients admitted for planned open abdominal surgery. All the subjects were patients of the Department of Surgery of the 4th Military Hospital in Wroclaw. Among them 57 were hypertensive and 34 normotensive (the control group). Fourteen patients of the essential hypertension group had resistant hypertension. Resistant hypertension was defined as blood pressure that remains uncontrolled despite the concurrent use of three antihypertensive agents of different classes. 32
The excluding criteria for all the study subjects were secondary hypertension, diabetes mellitus, and kidney failure.
Diagnosis of hypertension was established in every patient by clinical evaluation, including medical history of the patient. Clinical data collected for the study purposes were as follows: age, sex, height and weight, comorbidities, family history of hypertension, and routine laboratory test results. Physical examination included body mass index (BMI) evaluation and at least two blood pressure measurements by the Riva Rocci method. BMI was calculated as weight (kg) divided by the square of height (m2).
From all the study subjects, fasting blood samples and abdominal skin samples were obtained. Abdominal skin specimens were taken during the skin incision at the time of abdominal surgery. All the blood samples were taken before the surgery. The study was approved by the Bioethics Committee of Wroclaw Medical University (no 578/2012). All study subjects provided informed written consent before inclusion in the study. The procedures were in accordance with the 2008 Declaration of Helsinki.
Laboratory procedures
Blood samples
Venous peripheral blood samples were collected after an overnight fast using the Sarstedt S-Monovette System (Sarstedt AG & Co., Nümbrecht, Germany). Blood samples were centrifuged (1000 g for 15 minutes at 4°C). Plasma samples for NT-proANP and serum samples for VEGF-C and VEGF-D were initially frozen at −20°C (up to 2 weeks) and then were stored at −80°C until the analysis. Basic laboratory tests were performed immediately after venous blood collection with the use of standard commercial laboratory methods in the central laboratory of 4th Military Hospital in Wroclaw.
The biochemical workup in the study groups included the following: electrolytes (sodium and potassium), complete blood count, C-reactive protein, renal function (serum creatinine level, urea), hepatic function tests (aspartate transaminase and alanine transaminase activity, total serum bilirubin level, gamma-glutamyl transferase activity), and coagulation function (APTT, INR).
Plasma concentrations of NT-proANP and serum concentrations of VEGF-C and VEGF-D were performed using commercially available kits for ELISA (enzyme-linked immunosorbent assay): NT-proANP (1–98) ELISA (Biomedica Poland), Human VEGF-C Quantikine ELISA Kit (R&D Systems), and Human VEGF-D Quantikine ELISA Kit (R&D Systems).
Skin samples
Skin specimens for Na+ and water assessment were stored in containers made of polypropylene (Sarstedt) at −80°C until analysis. Skin specimens for histological assessment were initially fixed in 10% buffered formaldehyde solution and then embedded in paraffin.
Na+ concentrations in the skin specimens were measured after desiccating at 90°C for 72 hours. After dry ashing at 190°C for the next 24 hours and 600°C for an additional 48 hours, the skin ashes were dissolved in 20 mL 10% HNO3. Na+ concentrations in dissolved ashes were then measured with atomic absorption spectrometer.
33
Water content (W) in every skin sample was estimated as a percentage of the sample's dry weight, that is:
Skin specimens embedded in paraffin were cut into 5-μm-thick sections. For histopathological assessment, paraffin sections were stained with hematoxylin and eosin. For immunohistochemical staining, adjacent paraffin sections were freshly cut. Deparaffinization and antigen retrieval were performed in Target Retrieval Solution, pH Nine (97°C, 20 minutes) in PT Link Rinse Station. The sections were then washed in tris buffered saline (TBS) and incubated with primary antibodies (room temperature, 20 minutes), directed D2-40 (for lymphatic endothelium, monoclonal mouse anti-human D2-40), CD68 (for macrophages, monoclonal mouse anti-human CD68), and CD31 (for endothelium of all vessels, monoclonal mouse anti-human CD31) in Link48 Autostainer. EnVision FLEX set was used for the visualization of antigens in accordance with the manufacturer's instructions. All slides were then counterstained with Mayer's hematoxylin. All the abovementioned reagents were obtained in Dako (Glostrup, Denmark).
The immunostained slides were then assessed under BX-41 microscope (Olympus, Tokyo, Japan). The D2-40 and CD31 positively stained vessel count was estimated using the Chalkley method taking in account the number as well as lumina of identified vessels,34,35 making it the most suitable vessel assessment method for the current research. First, the sections were scanned at low power ( × 40, × 100 magnification) to identify the hot spots (areas of potentially the highest microvessel count) in the adventitia, which were then examined under × 200 magnification using a Chalkley Point Array graticule (Pyser Sgi., Edenbridge, United Kingdom). Three hot spots were evaluated and the average score was determined for each region of the section. For the evaluation of CD68-positve cells, the sections of three hot spots with potentially highest number of stained cells were counted under × 400 magnification.
Statistical analysis
Categorical variables were reported as number and percentage. Not normally distributed characteristics were presented as median with the interquartile range (Q1–Q3). Biochemical laboratory values were presented as mean and ± standard deviation.
Difference in sex among groups was calculated using the chi-square test. Kruskal–Wallis test was used for statistical analysis of the following variables: age, BMI, systolic and diastolic blood pressure, wet and dry weight of skin samples before ashing, skin Na+ and water content, number of macrophages (CD68), density of lymphatic vessels (D2-40), density of blood vessels (CD31), plasma concentration of NT-proANP and serum concentration of VEGF-C and VEGF-D, and basic laboratory findings. Post-hoc analysis was performed using Dunn's multiple comparison test. The correlations between the study parameters were calculated using Spearman's rank correlation test. In all the calculations, p ≤ 0.05 was considered statistically significant.
Statistical analysis was performed using Prism 6.0 (GraphPad, La Jolla, CA).
Results
Selected demographic and medical characteristics in the study groups are presented in Table 1. Baseline biochemical laboratory values and weight of wet and dry skin samples before ashing are presented, respectively, in Supplementary Tables S1 and S2 (Supplementary Data are available online at www.liebertpub.com/lrb).
Statistically relevant.
The groups with and without hypertension differed in skin expression of CD68 and in plasma concentration of VEGF-C. Differences in serum NT-proANP level among the study groups were insignificant, however, close to statistical relevance. Median and range quartile (Q1–Q3) of study parameters are presented in Table 2. Immunohistochemical expression of CD-68, D2-40, and CD-31 in the specimens of abdominal skin in the study groups is presented in Figure 1.
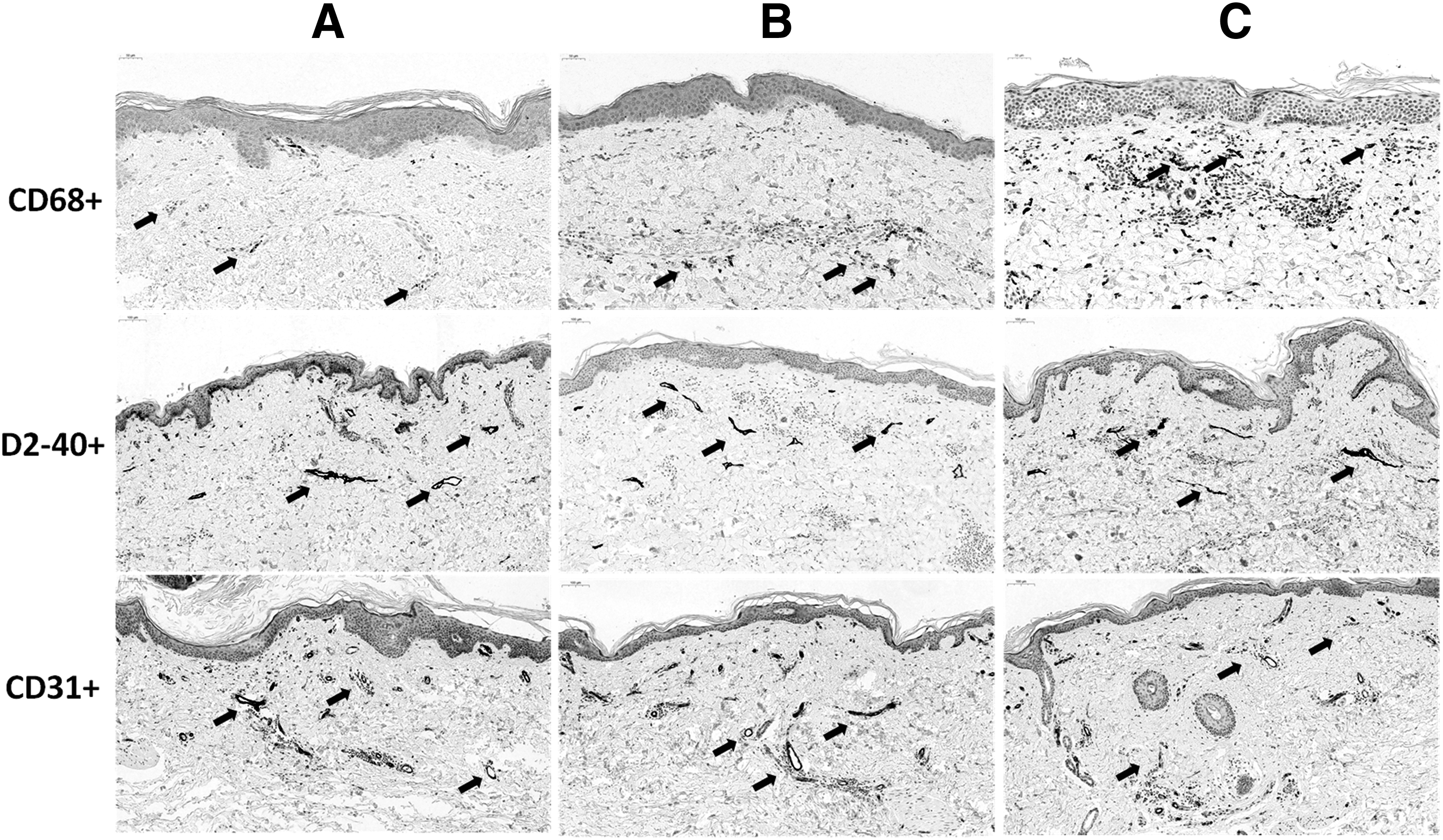
Immunohistochemical expression of CD68, D2-40, and CD31 in the specimens of abdominal skin in control
Statistically relevant.
VEGF, vascular endothelial growth factor.
Correlations in the control group were as follows: age correlated with plasma NT-proANP (r = 0.40; p = 0.019), BMI inversely with water content in the skin (r = −0,42; p = 0.014), Na+ content in the skin correlated with water content in the skin (r = 0.57; p < 0.001), CD68 correlated with D2-40 (r = 0.34; p = 0.051) and with CD31 (r = 0.37; p = 0.014), and D2-40 correlated with CD31 (r = 0.37; p = 0.032). Relationship between age and water content in the skin (r = 0.32; p = 0.067) was close to statistical relevance.
In the group with hypertension treated with less than three hypertensive drugs, the statistically significant correlations concerned only the relationship between Na+ content in the skin and water content in the skin (r = 0.58; p < 0.001).
In the group with resistant hypertension, the statistically significant correlations were the following: age correlated with CD31 (r = 0.60; p = 0.033) and inversely with serum VEGF-C (r = −0.74; p = 0.005), BMI correlated inversely with serum NTproANP (r = −0.63; p = 0.018), Na+ content in the skin correlated with duration of hypertension (r = 0.67; p = 0.009) and with plasma VEGF-D (r = 0.68; p = 0.009), and serum VEGF-D correlated with duration of hypertension (r = 0.67; p = 0.009). Relationships between water content in the skin and CD68 (r = 0.52; p = 0.058) and VEGF-D (r = 0.49; p = 0.075) were close to statistical relevance.
Discussion
The results of our study support the hypothesis that skin is involved in the pathogenesis of hypertension in humans.
We demonstrated directly that there is Na+ storage in the human skin. Na+ accumulation in human skin has been quantified only noninvasively, with using 23 Na-MRI.22,23 The direct measurement of the sodium content has been performed only on animal model.
Studies with 23 Na-MRI Titze et al. have demonstrated that skin Na+ deposition is greater in hypertensive subjects, in men, and increases with age.22,23 In contrast to muscles, skin sodium concentration corresponded to the skin water content. 22 Hemodialysis has resulted in lower muscle and skin Na+ content in patients with end-stage renal disease. 23 Spironolactone treatment has resulted in the decline of muscle Na+ concentration in patients with resistant hypertension. 22
Our study groups did not differ in the skin Na+ content, however, in the group with resistant hypertension, the medium Na+ concentration tended to be higher than in controls (Table 2). Our study confirms the finding of Titze et al. that greater Na+ content in the skin is associated with commensurate water retention, however, only in the control group and in the group with hypertension treated with less than three classes of antihypertensive drugs (this relationship was not present in the group with resistant hypertension). Instead, contrary to the studies of Titze et al., we did not observe the relationship between age or sex and Na+ content in the skin in any study group. Our results, on the contrary, revealed relationship between Na+ content in the skin, duration of hypertension, and serum VEGF-D concentration in the group with resistant hypertension.
Expected correlation between sodium concentration and plasma level of NT-proANP, as a marker of salt sensitivity, was not present in any of the study groups. This suggests that salt sensitivity is not just a consequence of a simple excessive accumulation of Na+ in the skin. There were also no relevant correlations between NT-proANP and other study parameters. Difference in serum NT-proANP concentration between the groups with hypertension and controls was close to statistical significance (p = 0.056).
The other important findings of our study include accumulation of macrophages in the skin and lower serum VEGF-C levels in hypertensive subjects.
The group with resistant hypertension had the greatest and control group had the lowest number of macrophages in the skin. Until now, the presence of macrophages in the skin in relation to hypertension had been assessed histopathologically only on animals. We had assumed that more macrophages in the skin would be associated with more lymphatic vessels in the skin. We observed such a relationship only in the control group. We suppose that the absence of such a relationship in the hypertensive groups results from a decrease in VEGF-C in these groups.
The control group had the greatest concentration of VEGF-C, and the group with resistant hypertension had the lowest concentration of VEGF-C. The results of the earlier studies on VEGF-C concentrations in hypertension are inconclusive. In one study, it has been shown that in patients with resistant hypertension, VEGF-C levels were greater than in normotensives. 24 In another study, it has been documented that in hemodialysis patients with hypertension, VEGF-C was lower in comparison to controls. 23 It has been also demonstrated that age-dependent increase in skin Na+ content paralleled reduced VEGF-C levels, 23 suggesting that decreasing VEGF-C levels in the elderly predisposes to Na+ accumulation in the skin, and possibly to hypertension. 23 Patients with higher VEGF-C levels showed lower Na+ content in muscle and skin after hemodialysis (measured with 23 Na-MRI), and thus tended to have improved Na+ removal from their skin during hemodialysis therapy. 23 We observed the inverse relationship between age and serum VEGF-C concentration only in the group with resistant hypertension.
The cascade of events from accumulation of sodium, through macrophage skin infiltration, VEGF-C expression, to lymphangiogenesis seems to be a protective mechanism against hypertension also in humans. Our study suggests that the higher number of macrophages in the skin and lower concentration of VEGF-C in groups with hypertension may reflect the blockade in synthesis/secretion of VEGF-C. Strong correlations between serum concentrations of VEGF-D and Na+ content in the skin and duration of hypertension in the group with resistant hypertension require further investigations. We hypothesize that VEGF-D may be secreted in greater amount in the place of lowered VEGF-C in this group of patients.
To conclude, our study supports the hypothesis that skin is involved in the pathogenesis of hypertension in humans. Decreased levels of serum VEGF-C in patients with hypertension suggest that impairment of lymphangiogenesis and protective function of the lymphatic system may play a role in the pathogenesis of hypertension.
Limitations
The group with resistant hypertension was relatively small. Our overall results will be based on a greater number of patients in this group.
We are also aware that Na+ deposition in various parts of human skin may differ. For our research, we used the abdominal skin excised during various surgical procedures with different abdominal incisions, thus from diverse parts of abdominal skin. Future studies to investigate such issues might be necessary. However, in our study, we focused rather on the relationships between skin Na+ content and the other skin elements that may be involved in pathogenesis of hypertension.
Moreover, it have been shown that spironolactone and hemodialysis influence Na+ body content.22,23 Other antihypertensive drugs, such as other diuretics, ACE inhibitors, sartans or β-blockers also may have an impact on the amount of Na+ in the body. The study patients have taken different antihypertensive drugs and probably their treatment chart had been changed in the past many times. That is why analysis of the influence of the drugs on skin Na+ content would be burned with too many errors. However, it may be hypothesized that if the study patients had not used antihypertensive drugs, the differences between the groups might be greater.
Footnotes
Acknowledgment
The study was supported by the Polish National Science Centre Grant No.: 2011/03/B/NZ4/05509. The funding body accepted the study protocol and had no later influence on data collection, analysis, interpretation, writing of the manuscript, or on the decision to submit the manuscript for publication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.