
Abstract
Abstract
Background:
To clarify the differences in the mode of fluid accumulation between arm and leg lymphedema using bioelectrical impedance analysis (BIA).
Methods and Results:
In 22 arms with lymphedema (ALE) and 65 legs with lymphedema (LLE), as well as 54 legs with venous edema (VE) for comparison, BIA was performed twice between April 2015 and March 2017. Then, the changes in BIA-derived parameters were correlated with the changes in extremity volumes. In ALE, the change in extracellular fluid resistance (Re) was negatively correlated with the change in arm volume (r = 0.51), while the change in intracellular fluid resistance (Ri) was constant, irrespective of the change in arm volume (r = 0.19). In LLE, the change in Re was negatively correlated with the change in leg volume (r = 0.67), but the change in Ri was also negatively correlated with the change in leg volume (r = 0.51). These correlations were similar to those in VE, in which the changes in Re and Ri were each negatively correlated with the change in leg volume (r = 0.66 and 0.53, respectively).
Conclusion:
The modes of change in BIA-derived parameters according to the change in extremity volume were different in ALE and LLE. The changes in LLE were similar to that in VE.
Introduction
W
Patients and Methods
This study was approved by the Institutional Review Board of Yamaguchi University Hospital (Ube, Yamaguchi, Japan). All participants provided written informed consent before enrollment. The study included 22 participants (22 arms) with ALE and 49 participants (65 legs) with LLE, who were in the maintenance phase of complex physical therapy in our clinic between April 2015 and March 2017. For comparison, 31 participants with venous edema (VE; 54 legs) treated in our clinic using compression therapy in the same period were included. In this study, leg edema caused by primary venous insufficiency, postthrombotic syndrome, and functional venous insufficiency (FVI) was regarded as VE. FVI was defined as follows: no reflux or occlusion in the deep, saphenous, and accessory saphenous veins, or in perforators on duplex venous ultrasound. The definition also included confirmed severe gait disturbance and/or prolonged sitting due to joint problems, general weakness, or obesity; and no other conditions causing edema (e.g., cardiac, hepatic, or renal failure). Dependent edema, which we considered FVI, may not be totally derived from venous insufficiency, but could also be due to reduced lymphatic pumping 7 and/or skin viscoelasticity. 8 However, because calf muscle pump failure can result in ambulatory venous hypertension,9,10 and because this group of participants often develops symptoms seen in advanced chronic venous insufficiency, 11 we included these participants in the study. The participants' characteristics are summarized in Table 1.
p < 0.05 vs. VE, ‡p < 0.05 vs. VE.
ALE, arm lymphedema; FVI, functional venous insufficiency; LLE, leg lymphedema; PTS, postthrombotic syndrome; PVI, primary venous insufficiency; VE, venous edema.
At the first visit for each participant, extremity volume measurements and bioelectrical impedance analysis (BIA) were performed. At subsequent visits, the same measurements were repeated. ALE volume was calculated based on tape measurements at 5-cm intervals from the axilla to the wrist, and LLE and VE volume were calculated at 10-cm intervals from the groin to the ankle, as described by Casley-Smith et al. 12 A bioimpedance spectrometer (U-400; Impedimed, Ltd., Brisbane, Australia) was used. Participants were placed in supine position in a room maintained at 25°C for 3 min before the measurements. Following degreasing with alcohol swabs, the specially designed electrodes were attached in a standard equipotential arrangement. All measurements were completed within 10 minutes. For ALE, the impedance in the affected arm was normalized to the contralateral normal arm, and used to obtain the extracellular fluid (ECF) resistance (Re) and intracellular fluid (ICF) resistance (Ri). Using these data, the L-Dex® (Impedimed, Ltd.) score (LDS) and impedance ratio (IR), both of which are indices used to represent fluid status in an extremity, were calculated. The basis of the L-Dex score is the comparison of the Re in the affected limb with that in the contralateral normal limb. The ratio is then compared with the ratio in a normal population, and LE is defined as a ratio more than three standard deviations greater than the mean: normalized.13,14 IR is the ratio of Ri to Re in the same limb, which is equal to the ratio of ECF to ICF volumes. 15 For LLE and VE, the impedance in an affected leg was normalized to the right arm instead of the contralateral normal leg, so that bilateral cases could be assessed. Although LDS in the leg is normally calculated using the contralateral normal leg as a reference, modified LDS obtained in this way (mLDS) has been validated and correlates very well with ordinary LDS. 16 IR in the leg was also calculated using these data.
Statistical analysis
The results are expressed as median (range) or count, unless otherwise indicated. To test the correlation between the parameters, simple linear regression analysis was used. To test the differences among the groups, the Kruskal–Wallis test was used; the Mann–Whitney U-test was used for multiple comparisons. Statistical analyses were performed using JMP 11.0 (SAS Institute, Cary, NC). A p-value <0.05 was considered significant.
Results
In ALE, Re decreased as arm volume increased (r = 0.51, Fig. 1A), while Re in the reference arm was relatively unchanged (Table 2). As a result, the change in LDS showed a good linear correlation with the change in arm volume (r = 0.72, Fig. 1B). The change in Ri was roughly constant, but was not zero (Fig. 1C). Accordingly, the change in IR (i.e., Ri/Re) was correlated linearly with the change in arm volume (r = 0.64, Fig. 1D).

Correlation between the change in extremity volume and the bioelectrical impedance parameters in arm lymphedema.
p < 0.05 between the first and second assessments, †p < 0.05 vs. LLE, ‡p < 0.05 vs. VE.
LDS, L-Dex score; mLDS, modified L-Dex score; Re, extracellular fluid resistance; Ri, intracellular fluid resistance.
In LLE, Re decreased as leg volume increased (r = 0.67, Fig. 2A), while Re in the reference arm was relatively unchanged (Table 2). As a result, the change in mLDS showed a good linear correlation with the change in leg volume (r = 0.74, Fig. 2B), as seen in ALE. However, the change in Ri showed a weak, but significant negative correlation with the change in leg volume (r = 0.51, Fig. 2C). As a result, there was no correlation between the change in IR and the change in leg volume (r = 0.31, Fig. 2D).

Correlation between the change in extremity volume and the bioelectrical impedance parameters in leg lymphedema.
In VE, Re decreased as leg volume increased (r = 0.66, Fig. 3A), while Re in the reference arm was relatively unchanged (Table 2). As a result, the change in mLDS showed a good linear correlation with the change in affected leg volume (r = 0.73, Fig. 3B), as seen in ALE and LLE. However, the change in Ri showed a weak, but significant negative correlation with the change in leg volume (r = 0.53, Fig. 3C). As a result, there was no correlation between the change in IR and the change in leg volume (r = 0.38, Fig. 3D), similar to the findings in LLE.
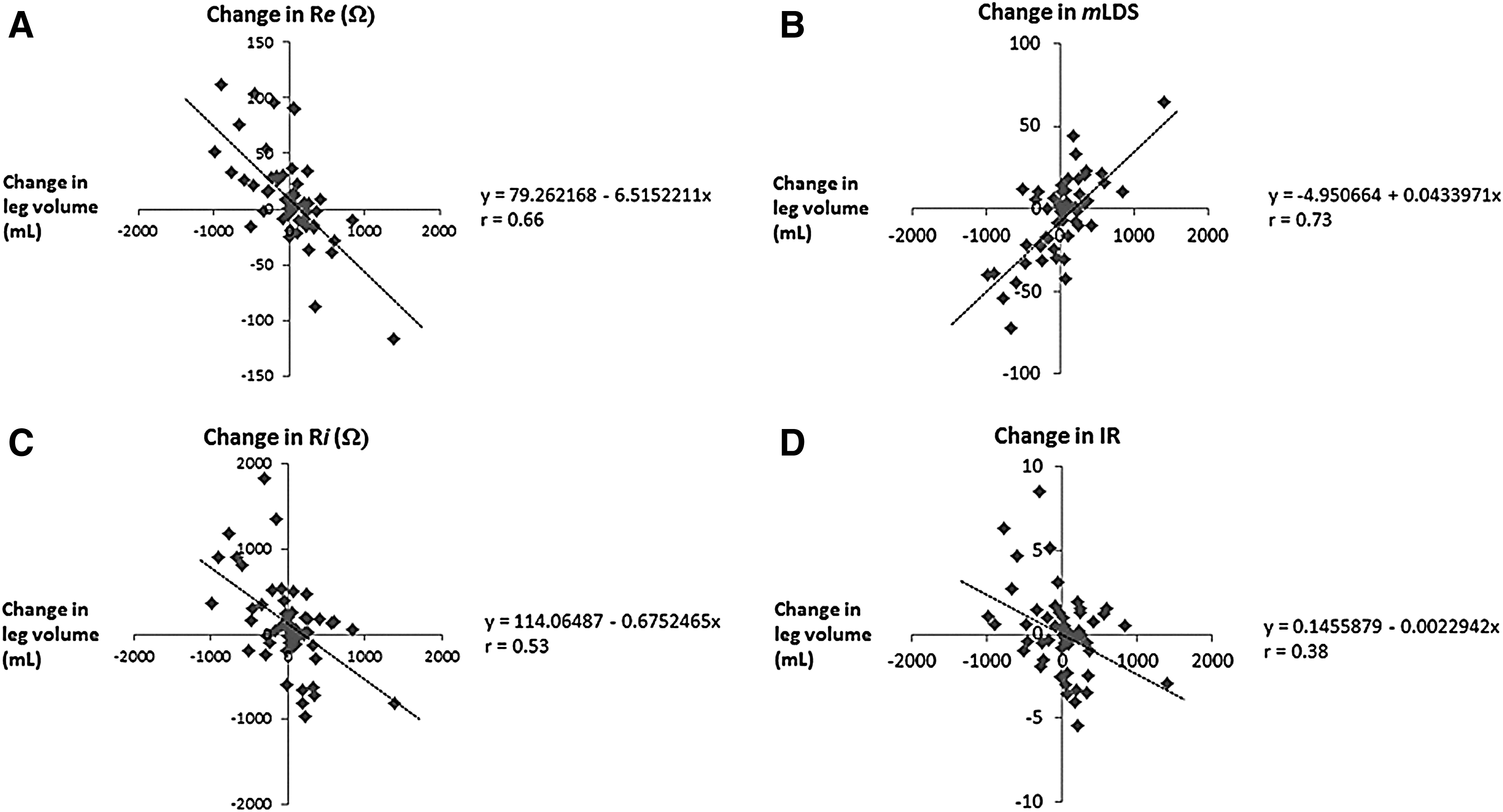
Correlation between the change in extremity volume and the bioelectrical impedance parameters in venous edema.
Discussion
In this study, we found that the change in Re was negatively correlated with the change in extremity volume in ALE, LLE, and VE. In contrast, the change in Ri was constant in ALE, while the change in Ri was negatively correlated with the change in extremity volume in LLE and VE.
In BIA, the main components of ECF are considered to be plasma and interstitial fluid (IF). Because the patients were placed in supine position before BIA to minimize venous blood pooling, current BIA results were likely to represent IF. It seemed natural that the changes in volume in VE legs were mainly due to changes in IF volume. However, it was surprising that the change in Re in both ALE and LLE was similarly correlated with the change in extremity volume because it is generally thought that the increase in volume of an extremity with lymphedema is caused by IF accumulation as well as (mainly adipose) tissue proliferation.17,18 However, these results indicated that the changes in limb volumes in ALE and LLE seemed almost solely derived from the change in IF volume. Although the basis for this result was unclear, possible explanations are that adipose tissue proliferation in lymphedema is accompanied by fluid accumulation, as seen in obesity, 19 or significant fat proliferation did not occur during this time span.
In LLE and VE, Ri decreased, that is, ICF increased, as leg volume increased. Because this was not observed in ALE, the phenomenon seemed specific to the leg. It is known that the change in ICF is related to osmotic factors 20 and the increase in venous pressure results in a decrease in the osmotic pressure in IF. 21 Therefore, the decrease in Ri in response to the increase in leg volume in VE is considered to be related to the increase in IF with low osmotic pressure. In LLE, the mode of change in Ri was very similar to that in VE, but it was clearly different from that in ALE. This means that the increase in IF in LLE is largely affected by increase in venous pressure, but not by impaired lymph drainage. On the contrary, the impact of venous pressure seemed very limited in ALE. In ALE, the change in Ri according to the change in arm volume was distributed consistently around 1000 Ω. If Ri was not affected by fluid accumulation, the change should have been zero. The reason for this discrepancy was unclear.
Another finding in this study was the difference between LDS/mLDS and IR. For ALE, both parameters seemed useful to represent fluid status, but this was not true for LLE and VE because IR changed due to the change in Ri in response to IF accumulation.
Limitations
With regard to extremity volume, the calculations based on tape measurement might be less accurate than those using methods such as perometry, although these expensive instruments were not available in our laboratory. However, the proximal limit of impedance measurement, for example, the level of the groin or axilla, using the BIA device is unclear. Therefore, the correlation between the extremity volume and BIA results would be different when such devices are used. The consistency of the Ri is based on the assumption that the electrolyte concentration is constant. 22 However, such an assumption might not be applicable in legs with edema and/or inflammation. 23 The impact of these factors could not be determined in this study.
Conclusion
We demonstrated that the modes of fluid accumulation in ALE and LLE were different. Modes of fluid accumulation in LLE and VE were similar, but distinct from ALE.
Footnotes
Acknowledgments
None.
Author Disclosure Statement
No competing financial interests exist.