
Abstract
Abstract
Background:
Compression therapy is the only conservative treatment that has been shown to be effective for patients with lymphedema in randomized controlled trials. A commonly used classification system divides pressure into four categories ranging from mild to very strong. For lower limb edema, bandages with strong pressure were shown to be most effective. Recent studies indicate that many health care professionals use inadequate pressure. No study thus far has focused on therapists who are trained in lymphatic treatment.
Methods and Results:
Thirty-seven physiotherapists trained in lymphatic treatment were recruited. Each participant received a questionnaire concerning their competence in compression bandaging. The subjects were asked to apply bandages using strong and medium pressure in two practical trials. Using a PicoPress® device, pressure was measured both directly after bandaging and 2 hours later; 75.68% of participants successfully applied the bandaging with moderate pressure, correctly at least once, and 62.16% managed to do so with high pressure. A trend in the results shows that the higher the sub-bandage pressure at the beginning, the more it dropped after 2 hours. There was high consistency in pressure application for strong and moderate pressure. No correlation was found between the parameters of the questionnaire and correct bandaging pressure.
Conclusions:
Most of the physiotherapists were successful, at least once, in applying bandages with the proper amount of pressure. It is possible that the nature of the lymphatic treatment contributes to their success. Participants were most accurate in applying moderate pressure; however, it is unclear what impact this pressure has on a leg with lymphedema.
Condensed Abstract
Compression therapy is the only conservative treatment proven to be effective for patients with lymphedema in randomized controlled trials. Studies show that many health care professionals use inadequate pressure. For this study, 37 physiotherapists trained in lymphatic treatment were asked to apply bandages using strong and medium pressure in two practical trials. A PicoPress® device was used to measure sub-bandage pressure. The majority of physiotherapists were successful, at least once, in applying bandages with the correct amount of pressure. Participants were most accurate in applying moderate pressure; however, it is unclear what impact this pressure has on a leg with lymphedema.
Introduction
L
Compression therapy is delivered through a number of methods, including bandaging and hosiery.1–3,5–14 Inelastic compression bandages are shown to achieve higher working pressure and better venous output than elastic compression garments. 6 However, the use of an inelastic bandage on a lymphatic limb is associated with a rapid sub-bandage pressure drop of nearly 50% of the initial value within 2 hours and two thirds after 24 hours.1,6–8 The ISL official recommendation is that patients with exacerbation of lymphedema in the lower limb ought to bandage their leg with multilayer bandaging on a daily basis. 1
A classification system for compression bandages was recommended by Partsch et al.; pressure of <20 mmHg was categorized as mild, 20–40 mmHg as medium, 40–60 mmHg as strong, and ≥60 mmHg as very strong. 10 In patients with leg lymphedema, bandages with strong pressure were shown to be the most effective. 8 However, in the presence of a venous ulcer on a lymphatic leg, pressure between 35 and 45 mmHg is the widely accepted range for sufficient and safe compression. 11 In a group of patients with mixed arterial–venous ulcers, inelastic compression bandages applied with a pressure up to 40 mmHg did not reduce arterial flow, but increased the venous pumping function. 12 The only accurate way for a clinician to determine sub-bandage pressure is to use a measuring device, 1 however, it is neither economical nor feasible, nor is it realistic in terms of time.1,13
Recent studies show that health care professionals use inadequate sub-bandage pressure.11,13,14 Protz et al. surveyed the knowledge of compression bandages and their use among medical, nursing, and caregiving professionals in Germany. 13 Of 891 providers, fewer than 10% applied the bandages with the intended pressure. 13 Additional studies reveal that even after attending wound care educational programs or courses, less than 35% of experienced nurses applied bandages with the pressure they aimed for.11,14 Such findings suggest that a considerable proportion of compression bandages that are applied are not meeting their goal. 13 Different studies show that training and the use of a pressure monitor help optimize compression bandaging skills of nurses. 11 No study so far has focused on therapists who are trained in lymphatic treatment. In the face of the importance of accurate pressure bandaging, the question whether physiotherapists succeed in correctly applying it is left unanswered. The main purpose of this study is to evaluate the pressure-applying accuracy in multilayer bandaging among physiotherapists in Israel who treat lymphedema.
Materials and Methods
The study was approved by the Assuta Medical Center Institutional Review Board (Helsinki Committee approval number 2016032). Thirty-seven physiotherapists skilled and certified in lymphatic treatment, who work with Maccabi Health Maintenance Organization, were recruited for this research. All of the participants signed a consent form. The physiotherapists were asked to apply bandages on the researcher's legs, a healthy 31-year-old woman, using strong pressure on one leg and medium pressure on the other. The number of compression bandages, the width of the bandage, and the technique were chosen by the participant. Resting pressure was measured directly after bandaging and 2 hours later using a PicoPress® measurement device (Microlab Elettronica SAS, Padua, Italy). The sensor was placed on B1 point, the area at which the Achilles tendon changes into the medial calf muscle. When activating the measurement probe, the leg was in a relaxed position on an even surface. For each participant, for validation and reliability purposes, two practical trials were held; the second took place a week or more after the first. Pressure values were concealed from the participants during the first trial.
Questionnaire
All participants received a questionnaire concerning their self-perceived competence in the application of compression bandages. The original questionnaire was used by Keller et al. in their study regarding a training program for nurses in the application of compression bandages, using a pressure monitor. 11 For this research, it was translated back and forth from German to Hebrew and slightly modified to suit different study populations. The questionnaire was completed before the beginning of the first trial.
Bandage kit
Participants received a bandage kit consisting of a cotton tubular bandage, Rosidal® K short-stretch compression bandages (Lohmann & Rauscher International, Rengsdorf, Germany), and Cellona® (Vernon Carus) padding materials. Other padding materials were permitted in case physiotherapists do not use soft syntactic padding in their daily practice.
Results
Table 1 presents the characteristics of the 37 participating lymphatic physiotherapists. All but one completed the two trials. On three occasions, initial sub-bandage pressure exceeded 110 mmHg and the bandages were removed before 2 hours had passed due to pain and discomfort. The therapists were later informed on this matter.
The majority of physiotherapists were successful, at least once, in applying bandages with the correct amount of pressure (Fig. 1). The mean values of the pressure measurements were in the desired range, with an average of 33.89 mmHg for moderate pressure (20–40 mmHg) and 52.86 mmHg for strong pressure (40–60 mmHg) (Table 2); 64.38% of the bandages that were supposed to provide moderate pressure were successful, as opposed to 41.1% that were supposed to provide strong pressure. Box plots in Figure 2 and Table 3 show the median, quartile, and interquartile range values.

Participant percentages, applied pressure measurement.
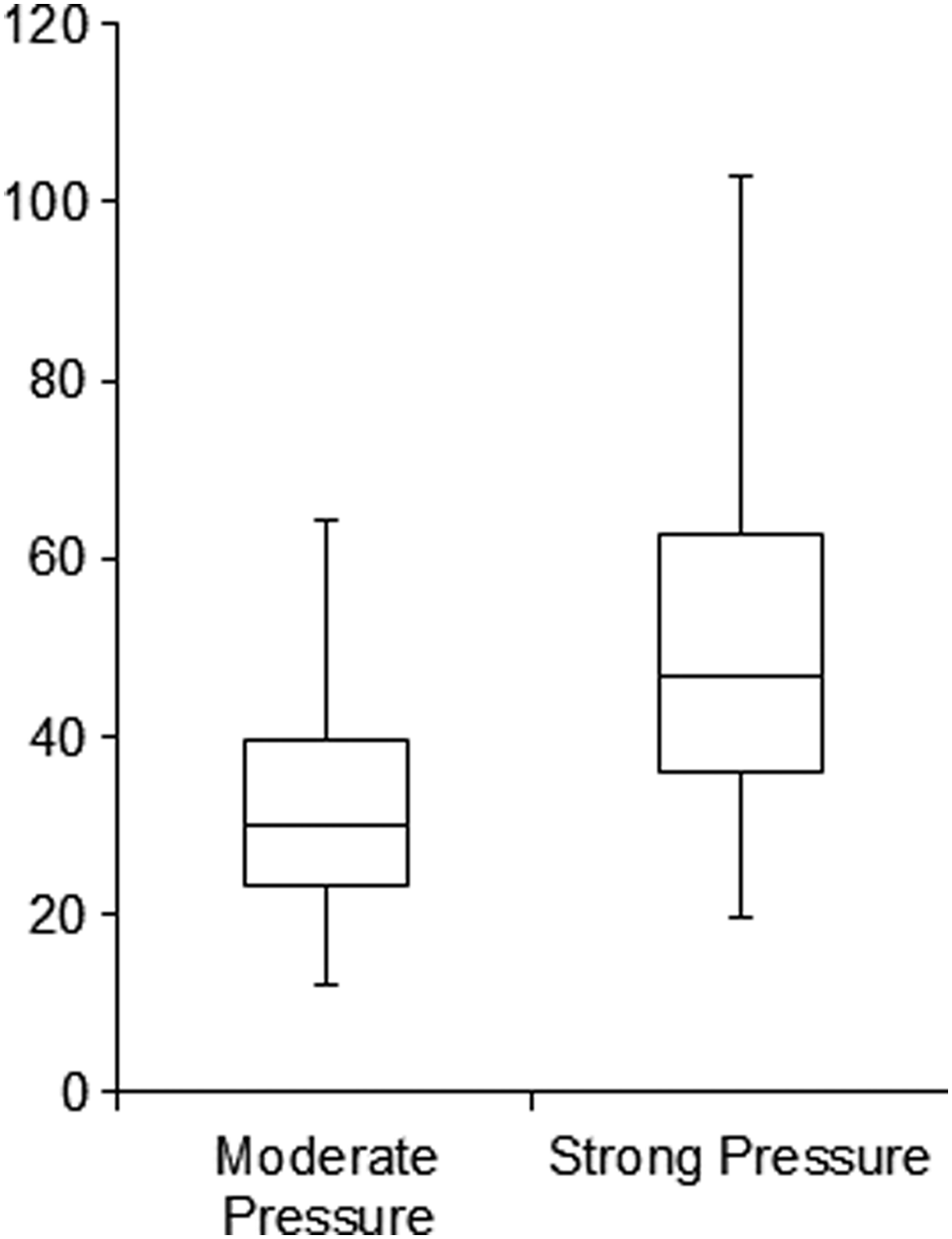
Pressure distribution (mmHg), moderate pressure versus strong pressure.
The intraclass correlation test was used to estimate inter-rater reliability. The results show high consistency in pressure application both for strong pressure, ICC(2,1) = 0.75 p < 0.0001, and moderate pressure, ICC(2,1) = 0.74 p < 0.0001. Box plots in Figure 3 show the percent of pressure drop after 2 hours for bandages that were applied with initial moderate or strong sub-bandage pressure. A two-sample t-test was used to assess the difference between the groups and it appears that the higher the sub-bandage pressure at the beginning, the more it dropped after 2 hours (t = −2.78, p < 0.01).
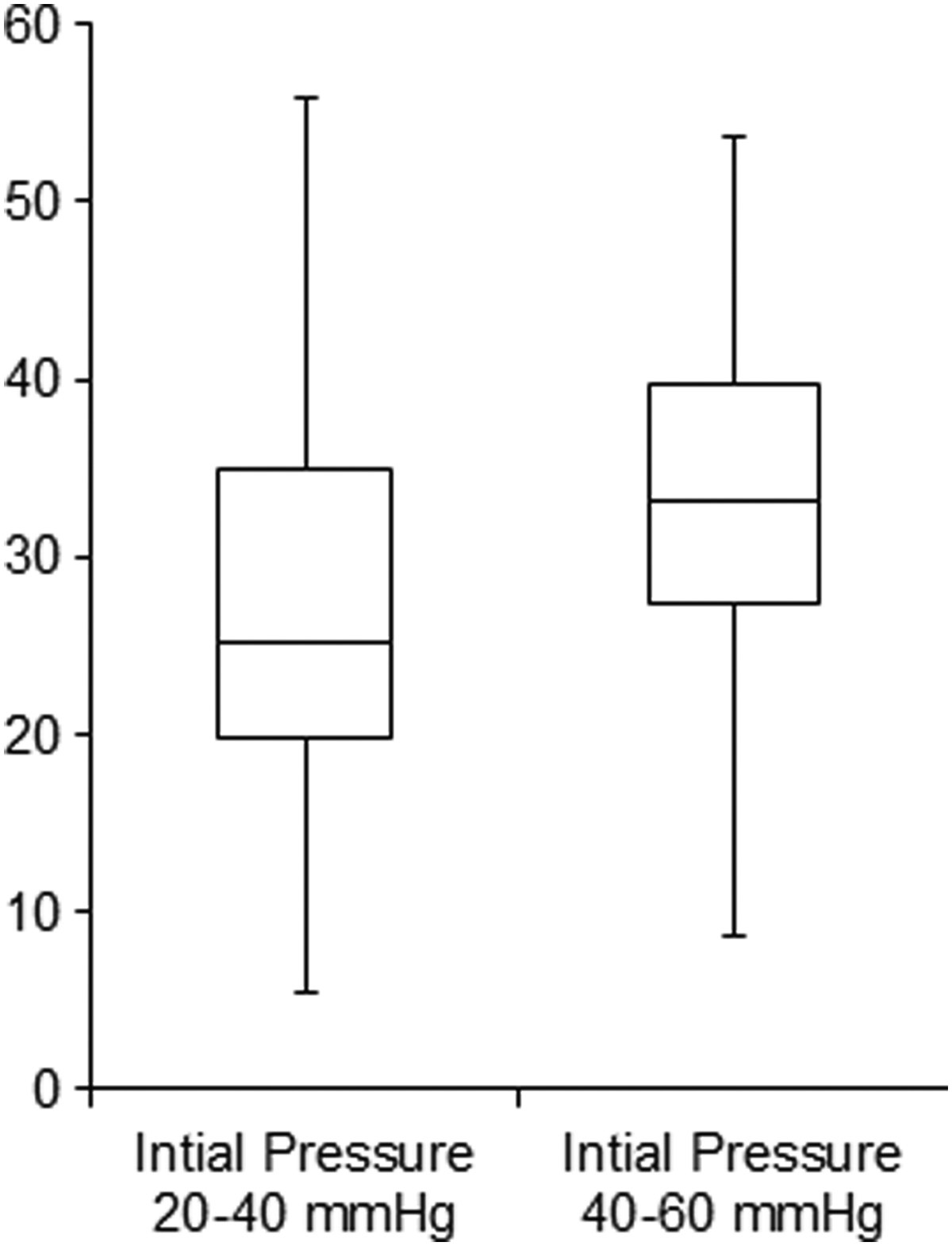
Percent of pressure drop after 2 hours.
Questionnaire parameters were tested alongside pressure measurements for any correlation. One-way analysis of variance was used when the data were distributed normally. The Kruskal–Wallis test was used in cases of non-normal distributions. Chi-square and Fisher exact were used for categorical variables. No correlation was found between the different parameters of the questionnaire and bandaging of legs with the correct amount of pressure.
Discussion
The purpose of this study was to evaluate the pressure-applying accuracy of physiotherapists who treat lymphedema. In recent years, small measurement devices such as PicoPress have allowed a more in-depth study into the world of compression therapy. In spite of the importance of precise pressure bandaging, studies that have used these devices have repeatedly shown that the majority of health care providers use inadequate pressure when applying multilayered compression bandages.11,13,14 In this study, 47.26% of the results were not in the desired range and ongoing education and training are necessary to improve the physiotherapists' skills; nonetheless, the current success rate is comparatively high.
No correlation was found between years of experience in lymphatic training and the ability to bandage legs with the correct amount of pressure. This is in correspondence with similar studies.11,14 Surprisingly, no correlation was found between previous practice with a pressure monitor and proper bandaging either. The PicoPress device is currently the only portable pressure monitor that was authorized by the Israeli Health Ministry. It has been in use since 2016 in several physiotherapy clinics and most of the participants used it once or twice. Those who have used the device three times and more did not show a higher success rate in bandaging with the proper amount of pressure; however, the total success rate of the physiotherapists is relatively high. It is possible that the nature of the lymphatic treatment contributes to their success. The purpose of the lymphatic treatment is to reduce edema and/or maintain the state of the affected limb. 3 It usually takes 1–2 weeks to achieve maximum reduction in edema, and during this time, it is necessary to measure the circumference of the limb multiple times. 3 Due to the quick impact of the treatment, it is easy for the therapist to assess whether the bandages provide sufficient amount of pressure. Previous studies that surveyed the manner in which health care professionals apply compression bandages focused mainly on nurses who treat venous ulcers.11,14 In contrast to the rapid reduction in swelling, ulcer wounds can persist for years, and the treatment is often prolonged.13,14 The length of the treatment can potentially affect the ability to apply bandages with the proper amount of pressure.
Participants were more successful in applying moderate pressure, with a 64.38% success rate in providing moderate pressure compared with 41.1% in applying strong pressure. The only studies so far that examined the use of bandages with moderate pressure tested their impact on blood flow in the lower leg6,12 and edema reduction in the arm.5,9 Researches that looked into the effect of different pressures on legs with lymphedema compared a compression bandage with strong and/or very strong pressure with a compression garment with moderate pressure.1,2,9 This comparison is problematic because it disregards the stiffness of different materials and its impact on lymph drainage. Therefore, it remains unclear what impact bandaging with moderate pressure has on a leg with lymphedema. It should be noted that in a study concerning upper limb lymphedema, patients who were treated with high-pressure bandages indicated more complaints of pain and discomfort compared with those who were treated with low pressure. 5 Further research in this matter is recommended since patient compliance is essential to the success of the treatment. 4
Sub-bandage pressure drops shortly after bandaging of legs.1,6–9 A study by Protz et al. showed ∼15% decrease in sub-bandage pressure after a four-time dorsiflexion of the foot. 13 A different study found a decrease of around 1/3 of the pressure after half an hour. 7 Most of the pressure reduction occurs within the initial 2 hours.1,7–9 In this study, there was on average 35.8% decrease in sub-bandage pressure when the initial pressure was more than 40 mmHg. This matches the 37% reduction observed 2 hours after bandaging healthy participants in Damstra et al.'s study. 7 However, pressure drop is not constant and may be influenced by different factors 8 ; the results of this study show a trend according to which the higher the sub-bandage pressure at the beginning, the more it will drop after 2 hours. At present, there are no studies that measured the decrease in different sub-bandage pressures after bandaging a leg with lymphedema; further research is needed to determine whether this tendency persists.
There are several factors that might have influenced the results of this study. First, some of the data were collected while the researcher was pregnant. Her leg volume was measured using a volumeter in the last weeks of the pregnancy and 4 months later, and she was found to have had mild grade 1 edema in both legs. However, this did not have a significant impact on pressure drop, meaning the results were similar during the pregnancy and afterward. Second, the bandages were reused often without being washed after each use. It is possible their natural wear influenced the sub-bandage pressure and the percent of pressure drop after 2 hours. Third, the applied compression bandages were not standardized. On the occasions when sub-bandage pressure was not in the given range, it was usually lower than what was asked, which is consistent with similar studies.11,13,14 Low sub-bandage pressure does not inflict any danger, but its value is unclear either. The ISL recommendations on pressure values for treating a leg with lymphedema are based on limited information regarding the effect of mild and moderate pressure. Future studies should investigate the efficacy of different sub-bandage pressure values on patients with lymphedema while taking into account its effect on patient compliance to the treatment.
Conclusions
The majority of physiotherapists who participated in this study were successful, at least once, in applying bandages with the correct amount of pressure. Additionally, they showed high consistency in pressure application. No correlation was found between years of experience in lymphatic training or previous practice with a pressure monitor and the ability to bandage legs with the correct amount of pressure. It is possible that the nature of lymphatic treatment contributes to their success. Participants were most accurate in applying moderate pressure; however, it is unclear what impact this pressure has on a leg with lymphedema.
Footnotes
Acknowledgment
The authors thank Ms. Dorit Tidhar for providing a PicoPress measurement device and for comments that greatly improved the manuscript.
Author Disclosure Statement
No competing financial interests exist.