
Abstract
Abstract
Background:
Lymphedema affects ∼15% of all patients after breast cancer treatment. The aim of this review was to assess the clinical effects (improvement in arm circumference and quality of life) of lymphaticovenous anastomosis (LVA) in treating breast cancer-related lymphedema (BCRL).
Methods and Results:
A systematic literature search was conducted in Medline, Embase and the Cochrane Library in July 2017, to identify all studies on LVA for the treatment of BCRL. The primary outcome was limb volume or circumference reduction and the secondary outcome was the improvement of quality of life. The search yielded 686 results, of which 15 articles were included in this review. All studies reported on BCRL in terms of volume or circumference reduction. Thirteen out of the included studies reported a positive surgical effect on reduction in volume or circumference. Twelve articles mentioned qualitative measures, being symptom improvement and improvement in quality of life. The number of patients who experienced symptoms relief ranged from 50% to 100% in the studies.
Conclusions:
The current review showed that the effects of LVA for the treatment of BCRL are variable among studies, although overall LVA seems effective in early stage BCRL. Higher quality studies are needed to confirm the effectiveness of LVA.
Introduction
L
A previous systematic review and meta-analysis by Basta et al. addressed the advantages and disadvantages of the various surgical techniques for the treatment of peripheral lymphedema. 12 In contrast, the current review of the literature specifically focused on the results of LVA for the treatment of BCRL patients only, thereby omitting other surgical options, lower extremity lymphedema, and primary lymphedema to create a more homogenous population.
The aim of this review was to evaluate the effectiveness of LVA for the treatment of BCRL in terms of volume and/or circumference reduction and improvement in quality of life. Additional analysis will be performed to assess which patients are most suitable for this intervention to be able to select the optimal patients with BCRL for treatment with LVA.
Materials and Methods
Eligibility criteria
All published studies on LVA for the treatment of BCRL were considered. A date restriction was applied. Only articles published after 1999 were included, since the quality of microscopes before that time are not deemed comparable to the current operating microscopes. Lymph vessels with a diameter varying between 0.2 and 0.9 mm are used in this technique to reduce the chance of venous backflow; hence, the quality of the microscope is an important factor. No language restrictions were applied.
Information sources and search
A comprehensive and reproducible electronic search was conducted by three independent researchers (A.C., J.B., and L.E.) in Embase, Medline and the Cochrane Library, to identify all published studies on LVA. In addition, clinicaltrials.gov was searched for ongoing trials and recently completed studies. Databases were searched from inception until July 1, 2017. Search terms are specified in Table 1.
Study selection
All references were stored in EndNote Reference Manager X7. Three reviewers (A.C., J.B., and L.E.) independently screened the titles and abstracts to determine which met the inclusion criteria. Any disagreements between the researchers were resolved by consensus. Studies performing LVA in patients with BCRL were included. Full-text articles were screened by the same three reviewers when articles seemed appropriate for inclusion. All potentially relevant publications excluded from the review are listed as such with the reason for exclusion. A flow diagram of the literature search is presented in Figure 1.
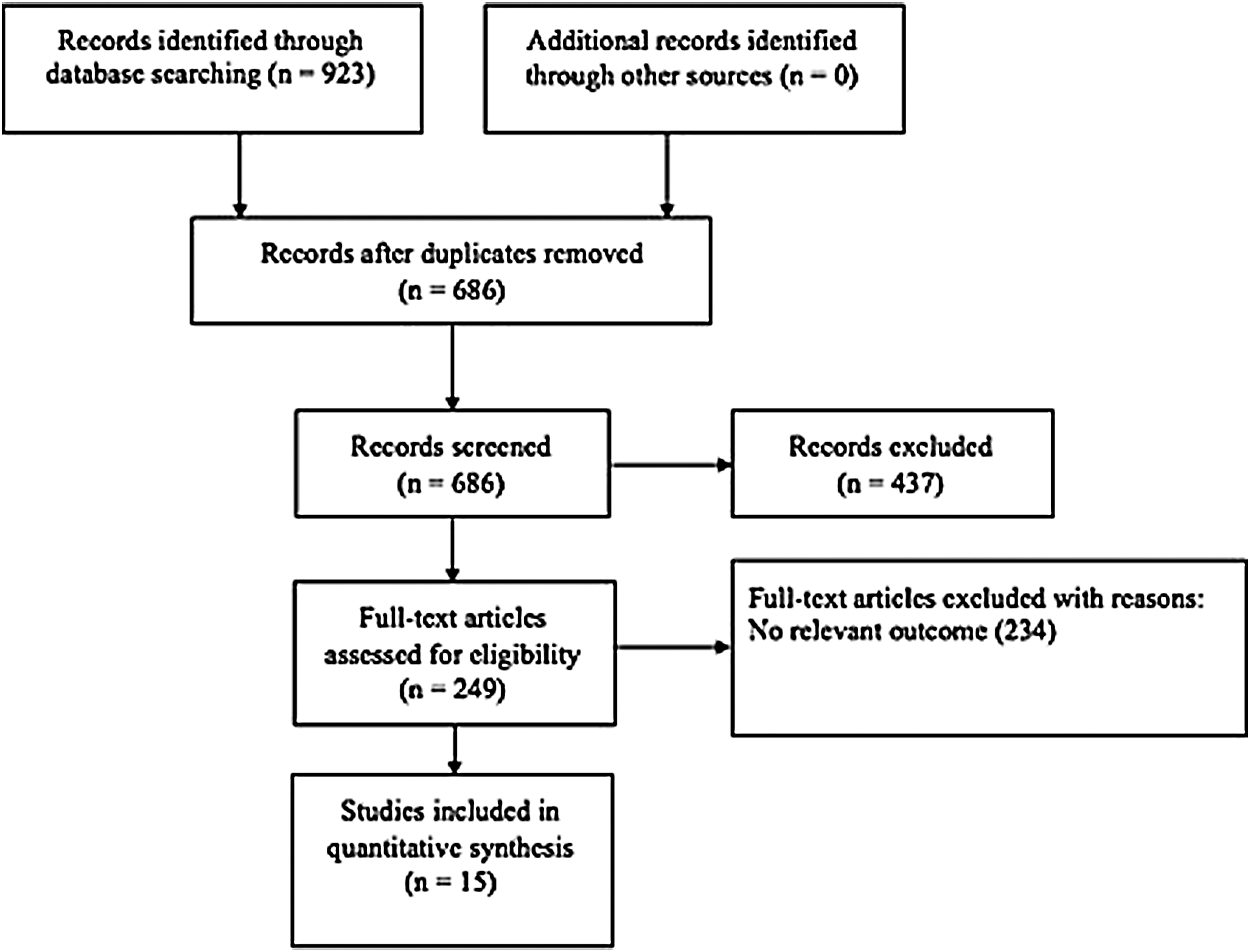
Flow diagram of the literature search according to PRISMA statement. Flowchart of the study selection.
Data collection process
A data extraction sheet was developed containing items on type of study, number of patients, oncological treatment, type of anastomosis, postoperative complications, follow-up, and outcome measures (volume, circumference, subjective complaints, and quality of life). The sheet was completed for all included studies.
Risk of bias in individual studies
The risk of bias in individual studies was assessed by the three aforementioned independent reviewers. Studies were screened for selection, intervention, and measurement bias.
Summary measures
The primary outcome measure was the mean limb volume or circumference reduction. The secondary outcome was the improvement of subjective symptoms or quality of life.
Synthesis of results
A systematic, narrative synthesis was provided with information presented in text and tables to summarize the effects of LVA in BCRL patients and to explain the characteristics and findings of the included studies. The narrative synthesis explored the connections and results both within and between the included studies, which were clarified in graphics that were created by using Microsoft Excel (2015). Furthermore, forest plots were created according to the random-effects model using Review Manager (RevMan) (Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Statistical significance was tested using a paired Students t-test in SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0; IBM Corp, Armonk, NY).
Additional analysis
Additional analysis of subgroups was provided to investigate whether LVA was more effective in early or moderate stages of lymphedema in comparison to severe lymphedema. The included studies used different types of classification systems. Therefore, the system to categorize the different classification systems into early, moderate, or severe lymphedema, used in the current study, can be found in Table 2. Another analysis was performed to assess the effect of the time from the onset of lymphedema till the surgical intervention.
ISL, International Society of Lymphedema staging; MDA, MD Anderson classification.
Results
Study selection
The literature search identified 686 studies after removal of duplicates. Full-text screening of 249 articles was performed. Case reports and studies on the results of LVA in lower extremity lymphedema were excluded. Studies where the etiology of upper limb lymphedema was omitted were excluded. Clinicaltrials.gov revealed two additional studies concerning LVA; however, these were not completed at the time of the literature search and writing. Finally, 15 of these articles explored the results of LVA in BCRL and were included in the review.13–27 The flow diagram is displayed in Figure 1.
Study characteristics
Fifteen articles concerning LVA in women with BCRL were analyzed. Eleven prospective studies and four retrospective studies were included. The average follow-up was 20 months, ranging from 2 months to 8 years.
Participants
The total study population consisted of 268 patients; 263 patients presented with BCRL, 1 patient with upper limb lymphedema after an elbow fracture, 13 and 4 patients with primary upper limb lymphedema.19,20 Twelve patients were included as a control group, they were not included in the study population as they did not undergo LVA. 19 The mean age was 55 years. The classification scales used for the staging of lymphedema greatly varied: the Campisi staging was most commonly used,13–15,17,18,25–27 followed by the International Society of Lymphedema (ISL) classification system20,22,23 and the MD Anderson classification.16,21 One study used Cheng's lymphedema scale. 24 One study did not report on the use of any classification system. 19 The study and patient characteristics are presented in Table 3.
The average excess circumference of the affected arm compared with the normal forearm.
One patient was lost to follow-up.
Two patients had primary lymphedema.
MDA based on ICG lymphangiographic findings.
Two patients experienced skin irritation on the contrast injection site, both were treated conservative.
ALND, axillary lymph node dissection; BCRL, breast cancer-related lymphedema; CT, chemotherapy; E-E, end-to-end anastomosis; E-S, end-to-side anastomosis; GA, general anesthesia; IB, isosulfan blue; ICG, indocyanine green; LA, local anesthesia; Mast, mastectomy; MB, methylene blue; NR, not reported; P, prospective; PB, patent blue; R, retrospective; RT, radiotherapy.
Intervention
The intervention in all the included studies was a LVA. However, the technical procedure differed largely between studies. In six studies, only end-to-end anastomoses were used,13,15,18,19,25,26 in four studies, both end-to-end and end-to-side were used,14,16,24,27 in one study, the “Octopus technique” was used, 17 and in four studies, the type of anastomosis was not reported.20–23
Control group
A control group was provided in two articles. One study included a control group where the patients who only received continuous bandaging were compared with those who underwent the intervention and continuous bandaging. 19 Another study included several groups to compare the effect of different interventions, including LVA and lymph node transfers in combination with or without microvascular breast reconstruction, to groups only receiving decongestive therapy. 24
Outcome measures
The volume or circumference reduction was mentioned as the primary outcome in 11 studies.13–19,22,25–27 Most studies also reported on subjective outcomes such as symptom reduction, improvement in quality of life, or a decrease in hardness of the limb.
Risk of bias within studies
To begin with, the level of evidence of the studies investigating the effect of LVA is low, with only two level III studies and the rest being level IV evidence. The low level of evidence is due to the lack of control groups in most trials and the small sample sizes.
Furthermore, most trials did not mention whether consecutive patients were included, so the chance of selection bias could not be dismissed. Most studies did not mention whether the procedure was performed by the same surgeon or failed to mention the experience/qualifications of the surgeon. The follow-up in some studies is not long enough to evaluate the long-term effect of the anastomoses in the limb reduction and decrease in subjective symptoms. Table 4 shows the methodological quality assessment.
+, yes; +/−, moderate; −, no.
Results of individual studies
Koshima et al. showed that the mean decrease in total excess circumference postoperative was 4.1 cm (47.3%) in the LVA group compared with 0.8 cm (11.8%) in the bandaging group, implying a higher circumference reduction for the LVA group. 19
Damstra et al. included 10 patients with Campisi stage III lymphedema in a prospective study. Although 50% of the patients presented subjective relief of their complaints, after 12 months, the volume reduction was 2%. 18
Chang conducted a prospective study with 20 patients with variable lymphedema stages. The mean volume reduction after 12 months was 35%. Furthermore 80% of the patients reported a long-term symptom improvement at 18 months of follow-up. 15
Auba et al. retrospectively performed a study concerning LVA in 7 patients with upper limb lymphedema who had a variable Campisi stage and only reported a circumference reduction of 0.85 cm after 18 months follow-up. One patient was lost to follow-up. Ninety percent of the patients had noticeable improvement of symptoms. 13
Mihara et al. reported a reduction rate of 6% after LVA with a follow-up of 2 months. Furthermore, patients experienced a decrease in hardness of the arm. 20
Ayestaray et al. reported a mean volume reduction of 22.8%. In addition, three out of four patients could discontinue lymph drainage therapy for 4 months, and 90% of the patients reported a better quality of life after 6 months. 14
Chang et al. published results on a prospective study concerning 30 patients with BCRL. After 1-year follow-up, a mean reduction of 61% in the early-stage group (MD Anderson stage I or II) was reported, whereas a mean reduction of 17% in the late-stage group (MD Anderson stage III or IV) was presented. Overall, 96% of the patients presented subjective improvement of their symptoms. 16
Chen et al. performed a prospective study, including six patients with the “Octopus” technique, to create the anastomosis. The mean upper extremity lymphedema index preoperatively was 135, and postoperatively this was reduced to 122. 28 The average reduction was 9.6%. Furthermore, all patients experienced prompt relief of symptoms. 17
Torrisi et al. presented a prospective study with six patients, in which half of the patients had a moderate decrease in limb volume. An opto-electronic limb volumeter was used. Five patients reported improvement of symptoms. 21
Gennaro et al. performed a retrospective study on 69 patients, of which 39 presented with upper limb lymphedema due to BCRL. An average volume reduction of 50% after LVA was observed. Many patients could also stop their decompression therapy and noticed improvement in subjective symptoms such as reduction in heaviness, hardness, functional impairment, and pain of the affected arm. 22
Cornelissen et al. prospectively performed a study on the improvement in quality of life after LVA in women with BCRL. They found a decrease in circumference, although not statistically significant. They also found a statistical significant improvement in quality of life after 1 year of follow-up using a validated questionnaire (lymph-International Classification of Functioning, Disability and Health). Moreover, 85% of the patients discontinued compressive stockings. 23
Engel et al. presented a study comparing the outcome of microsurgery, including LVA and vascularized lymph node flap transfer with or without microvascular breast reconstruction, for the treatment of BCRL. One group with 23 patients only received LVA, they were included in the review. A mean reduction rate of 17.3% was observed after a follow-up of 19 months. 24
Lee et al. performed a retrospective study on LVA with a follow-up of 2 years. Three patients with upper limb lymphedema due to breast cancer were included. Two patients with Campisi stage II lymphedema showed an increase in volume after 2 years and one patient with stage III lymphedema showed a decrease. The mean volume reduction rate was −4.7% after 2 years. 25
Poumellec et al. published results on a prospective study with 31 patients who had undergone stepped LVA for BCRL. No patients were lost to follow-up. Eighty-four percent of the patients experienced a moderate to substantial increase in quality of life. 93.5% of the patients showed a reduction in circumference. However, the mean overall decrease after 1-year follow-up for all patients was only 24.7%. They also report that patients with a lower Campisi lymphedema stage had better results. 26
Winter et al. performed a retrospective study on the efficacy of LVA in BCRL on 29 patients. After 1-year follow-up, the percentage volume reduction was 33%. Only one patient showed an increase in volume. The overall perceived quality of life also increased. Fifteen patients were able to discontinue the use of compression garment. 27
The number of patients with early- and late-stage lymphedema for each study is shown in Figure 2. The results concerning volume reduction are presented in Figure 3.

Division between early, moderate, and late-stage lymphedema within studies according to Table 2.
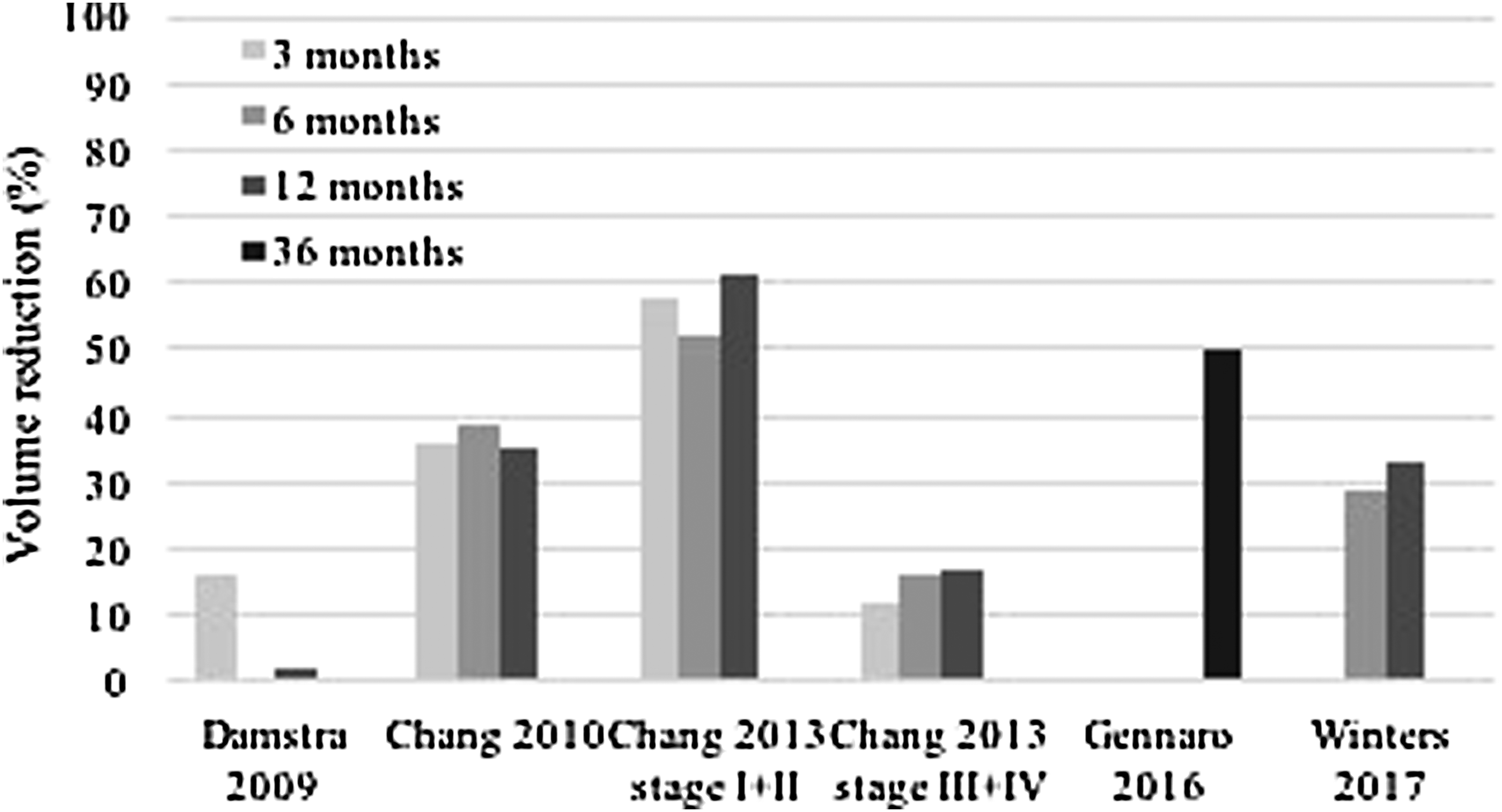
Volume/circumference reduction as measured over a period of time.
Additional analysis
The additional analysis performed studied the effect of LVA in different lymphedema stages and differences concerning the years from the onset of BCRL. Since the articles used different ways to present their outcome measurements, it was not possible to analyze all articles. Therefore, the forest plots are limited. Subanalysis concerning years of onset was performed (Figs. 4 and 5), and a subanalysis of the effect of LVA in patients with moderate versus delayed lymphedema was performed (Fig. 6).

Forest plot comparing years of onset of BCRL on the effect of LVA years of onset since 2–5 years versus >5 years. Effect of LVA was considered either volume or circumference reduction in the affected arm comparing preoperative measurements with postoperative measurements (longest available follow-up was used). BCRL, breast cancer-related lymphedema; LVA, lymphaticovenous anastomosis.

Forest plot comparing years of onset of BCRL on the effect of LVA years of onset since <2 years versus 2–5 years. Effect of LVA was considered either volume or circumference reduction in the affected arm comparing preoperative measurements with postoperative measurements (longest available follow-up was used).

Forest plot comparing stage of lymphedema on the effect of LVA moderate versus late-stage lymphedema. Effect of LVA was considered either volume or circumference reduction in the affected arm comparing preoperative measurements with postoperative measurements (longest available follow-up was used).
Discussion
Summary of evidence
A reduction in either circumference or volume was shown in 13 out of 15 studies. Two studies report an increase in upper limb volume.18,25 This lack of volume reduction could have been caused by the more advanced stage of lymphedema of the entire study population. Furthermore, the postoperative scintigraphy in that study showed absence of lymph transport, dermal backflow, and few signs of organized transport at the level of the LVA. This might indicate that the quality of the lymph vessels that were used was not good enough to create a working anastomosis. Finally, the anastomoses were made in the upper arm where the lymph flow is already damaged, and therefore, creating the LVA more distally could have provided better results. 18 The other study reports that during the treatment of some patients, the indocyanine green (ICG) lymphography was not available in their nation during the study period. Therefore, some surgeries may have been performed with inappropriate lymph vessels with a suboptimal function. 25
Twelve out of 15 included studies reported an improvement of symptoms in patients after LVA. In some cases, this improvement was already noticed during the first postoperative week.15,17 The number of patients who experienced improvement varied between 50% and 100%.
One of the largest included studies is by Chang et al., clearly proposed that LVA is substantially more effective in early stages of lymphedema in the upper extremity than late stage or lower limb. 16 Due to the fact that in early stages the lymphatic wall is not completely damaged, the contractility is still present. 29 Contributing to the idea that LVA is more effective during early stages of lymphedema, some studies, not included in this review, suggest the use of LVA as preventive measure in women with breast cancer undergoing mastectomy and further treatment. Boccardo et al. were the first to describe this approach as the “Lymphatic Microsurgical Preventing Healing Approach” (LYMPHA) and reported that the incidence of secondary arm lymphedema after preventive LVA was 4.1% in comparison with a 13%–65% incidence rate after axillary dissection without LVA. 30 They reported that it is a safe procedure to prevent lymphedema and allows surgeons to preserve blue nodes, but it was not possible to make sure that the preserved nodes are not metastatic. 31 This also suggests that applying LVA as preventive measure or in an early stage provides beneficial outcomes for women with BCRL.
Additional analysis
The additional subgroup analysis showed that the effect of LVA was statistically significantly better in patients with moderate lymphedema when compared with severe lymphedema (Fig. 6) and that less years since onset also had a positive effect on the outcome of LVA (Figs. 4 and 5). Preferably, we would have also performed subgroup analysis regarding distal versus proximal anastomosis, number of anastomosis, and follow-up period. Unfortunately, we were not able to retrieve enough information from the included studies. Lymphedema is known to worsen over time as it is a progressive chronic disease. The physiology of the lymphatic vessels changes over time to fibrotic tissue which no longer functions as lymphatic transporters. This process in BCRL starts proximally and progresses distally. Therefore, chances to find a functioning lymphatic vessel are higher in early onset, nonsevere lymphedema patients in the distal arm. This hypothesis is confirmed by our results.
Limitations
The volume and level of evidence of the studies on the effects of LVA in this specific patient population were low. Thirteen out of 15 studies provided level IV evidence, and only 2 studies provided level III evidence, but these were retrospective studies. No randomized controlled trial could be included, which displays the lack of solid evidence on this topic.
Furthermore, the follow-up time in some studies was too short, with follow-up ranging from 2 months to 6 years. This raises doubts, since studies with a short follow-up time reported good outcomes, but it remains unknown whether this reduction was maintained over a period of time.
Another contributing factor to the low level of evidence was the low number of patients included in the studies and the lack of control groups in almost every study.
The broad variety in the years from onset till the LVA contributed to the heterogeneity of our study population. Some patients only suffered from lymphedema for 1 year till the operation, while others were operated after 10 years, this also affects the condition of the lymph vessels.
The success of LVA depends upon surgical skills. Unfortunately, a lot of details on the surgery itself were unknown or poorly described. It is unknown how experienced/qualified the surgeons were. This means that the quality of the LVAs cannot be guaranteed.
Finally, the way the outcomes were described varied enormously between studies. Some reported in terms of absolute or relative volume reduction while others mentioned circumference reduction. Contributing to the differences in reporting, sometimes the reduction was calculated using the preoperative volume, but other times the reduction was calculated by comparing it to the contralateral healthy arm.
Conclusions
Heterogeneous results of LVA in the volume/circumference reduction for the treatment of BCRL were reported among studies. Improvement of the subjective symptoms was presented in most of the studies. The current review showed that LVA may be particularly useful to improve quality of life in breast cancer-related lymphedema, in particular, in early-stage lymphedema in the distal arm. This hypothesis is confirmed by our results. Further prospective, randomized controlled studies are required to confirm the effectiveness of LVA and to determine the appropriate candidates for this procedure.
Ethical Considerations
This study is not reporting on experiments with human subjects, but is a literature review. Therefore, ethical approval is not applicable.
Footnotes
Author Disclosure Statement
No competing financial interests exist.