
Abstract
Abstract
Background:
Obesity is one of the well-known initiating and aggravating factors of lymphedema. Body mass index (BMI) is typically used to define obesity, but in Asian populations, health risks are elevated at lower BMI levels, and abdominal fat may be a better obesity metric. Thus, we assessed the potential association between abdominal obesity and lymphedema severity in postoperative breast cancer patients.
Methods and Results:
Thirty-three women with breast cancer-related lymphedema participated in this study. Arm circumference was measured at four locations per arm to identify the maximal circumference difference (MCD) between the affected and unaffected sides. All patients underwent lymphoscintigraphy, and we calculated the quantitative asymmetry index (QAI) of both arms. A computed tomography was also performed to assess abdominal obesity after lymphedema. Abdominal obesity was classified as a visceral fat cross-sectional area larger than 70 cm2. Fourteen women (42%) were obese (BMI ≥25 kg/m2), and 18 women (54%) had increased abdominal fat. BMI obesity and abdominal obesity were significantly correlated, but five patients were classified with abdominal obesity, despite a BMI below 25 kg/m2. The mean arm circumference difference was 2.8 ± 2.4 cm. Decreased axillary QAI was significantly correlated with obesity, and increased arm edema (MCD ≥2 cm) was significantly correlated with abdominal obesity.
Conclusion:
Abdominal obesity was significantly correlated with increased MCD and should be considered along with obesity as an aggravating factor for lymphedema severity.
Introduction
L
Obesity is a well-known initiating and aggravating factor of lymphedema; previous studies found that two groups undergoing dietary restriction (a low-calorie diet group and a low-fat diet group) had reduced lymphedema volume compared with a control group. Furthermore, there was a higher rate of lymphedema occurrence in a group with a body mass index (BMI) ≥30 kg/m2 compared to that of a group with a BMI <30 kg/m2,16 In addition, a case–control study demonstrated that the severity of lymphedema was significantly associated with BMI, in addition to infection and level of hand use. 17 Together, these results indicate that obesity is a significant prognostic factor for lymphedema occurrence and aggravation. Most studies recommended weight monitoring in breast cancer patients, using BMI as an indicator of obesity.18–20
Along with BMI, abdominal fat is another predictive factor to consider. In addition, there is an association between BMI and abdominal fat, as BMI can independently predict abdominal visceral fat content. 21 In 1998, World Health Organization (WHO) indicated abdominal obesity as a necessary requirement as diagnostic criterion for metabolic syndrome, highlighting different diagnostic criteria for different ethnic groups. Especially in Asians, including Korean population, there is higher health risk even with lower obesity level compared with western people, and abdominal fat is often considered more important risk factor than BMI.22,23
According to Buzato and Brigidio, 40% of normal-weight lymphedema patients had increased visceral abdominal fat measured using bioimpedance, highlighting the need to consider the importance of intra-abdominal fat in addition to BMI in this patient population. 21 No other previous studies have analyzed abdominal obesity as an aggravating factor of lymphedema.
This study aims to assess the relationship between abdominal obesity and lymphedema severity based on clinical testing and imaging in postoperative breast cancer patients diagnosed with lymphedema.
Materials and Methods
Study subjects
Thirty-three women with breast cancer-related lymphedema participated in this cross-sectional study. The inclusion criteria were: (1) unilateral arm lymphedema after surgical breast cancer treatment, with or without axillary LN dissection, and (2) voluntary participation in the study. The exclusion criteria were: (1) lymphedema with other etiologies (primary, traumatic, etc.); (2) other associated major illnesses; and (3) active infection (e.g., cellulitis at the edema site).
Procedures
All eligible rehabilitation center outpatients were recruited from March 2015 to February 2016. Patients were enrolled in the study after providing written informed consent.
Demographic and clinical characteristics
Baseline demographic and clinical characteristics of all enrolled patients were evaluated. A complete enumeration survey of all patients was performed by medical record review. The disease course during admission was documented, including information on cancer stage, surgical procedure (including presence of axillary LN dissection), and having received chemotherapy or radiotherapy. BMI (kg/m2) was measured during outpatient visits to the rehabilitation clinic; patients with a BMI ≥25 kg/m2 were classified as obese based on the WHO-defined obesity standard for adult Asians. 24 We also measured arm circumference at four locations on each arm, including the metacarpal joint, wrist, and 10 cm above and below the elbow. 25 Arm circumference was measured using a nonelastic measuring tape on the same day as the lymphoscintigraphy and CT scan. To maximize reliability, one rehabilitation medicine clinician measured the circumference twice, and the mean value was recorded. The maximal circumference difference (MCD) was calculated as the difference between the affected arm and unaffected arm at the uppermost symptomatic arm location (Fig. 1). 26
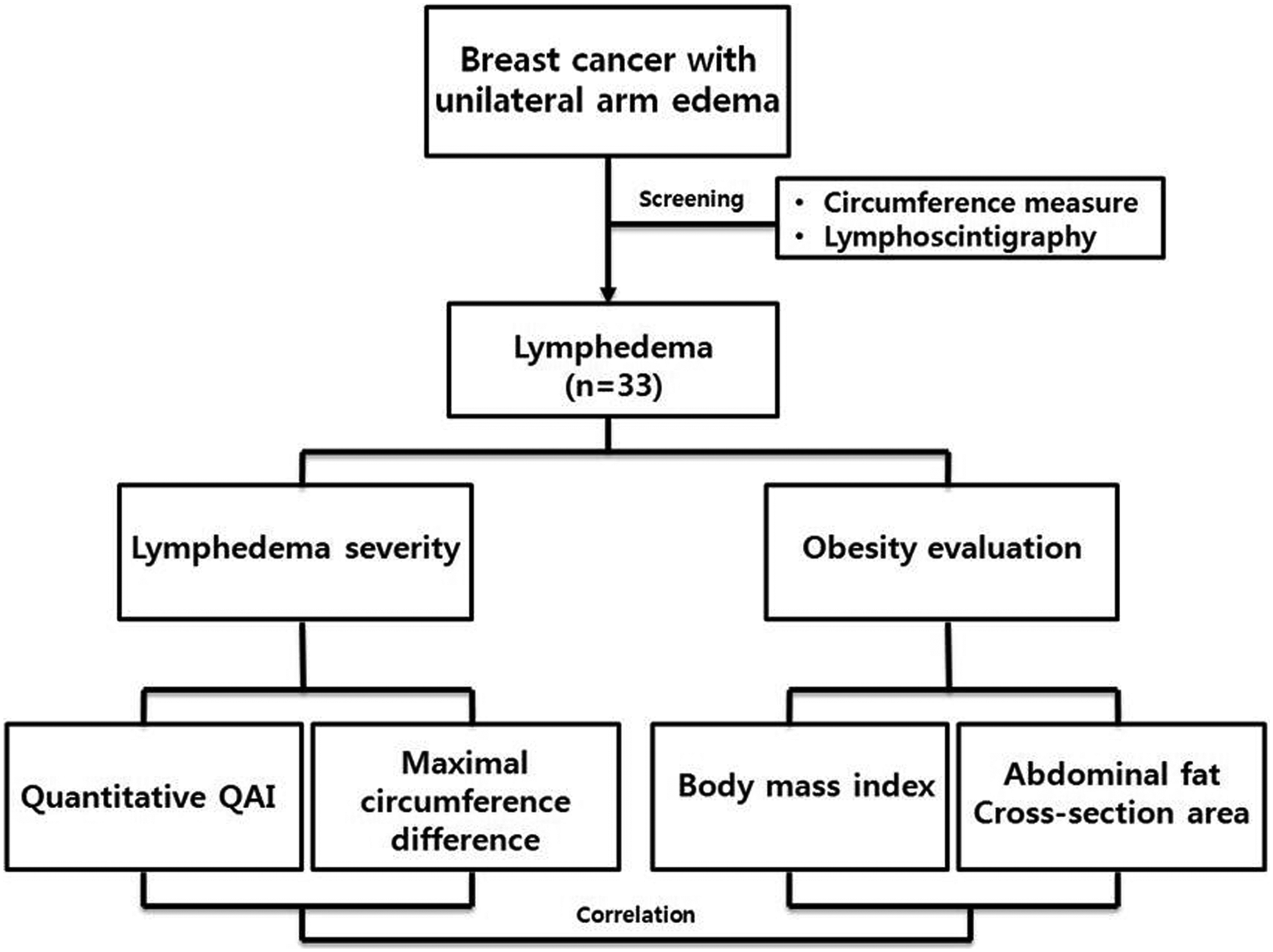
Study diagram of 33 patients with lymphedema.
Quantitative lymphoscintigraphic analysis
We performed lymphoscintigraphy on all patients to differentiate lymphedema from other types of edema (e.g., due to deep vein thrombosis).
27
The quantitative asymmetry index (QAI) was calculated for the axillary LN and the arm, as previously referenced.28,29 The regions of interest (ROIs) of both axillary LNs and arms were drawn, and the asymmetry indices were calculated based on radioactivity in the ROI using the following formula, where the gamma count was the total radiopharmaceutical uptake in the ROI.
CT scan analysis
On the same day of arm circumference measurement, we measured the cross-sectional area of visceral fat at the second lumbar vertebra level(slightly above the umbilicus) to assess abdominal obesity after lymphedema. 30 For the classification of abdominal fat, vales up to 70 cm2 were considered “normal,” and values greater than 70 cm2 were considered “above normal” and as abdominal obesity 31 (Fig. 2).
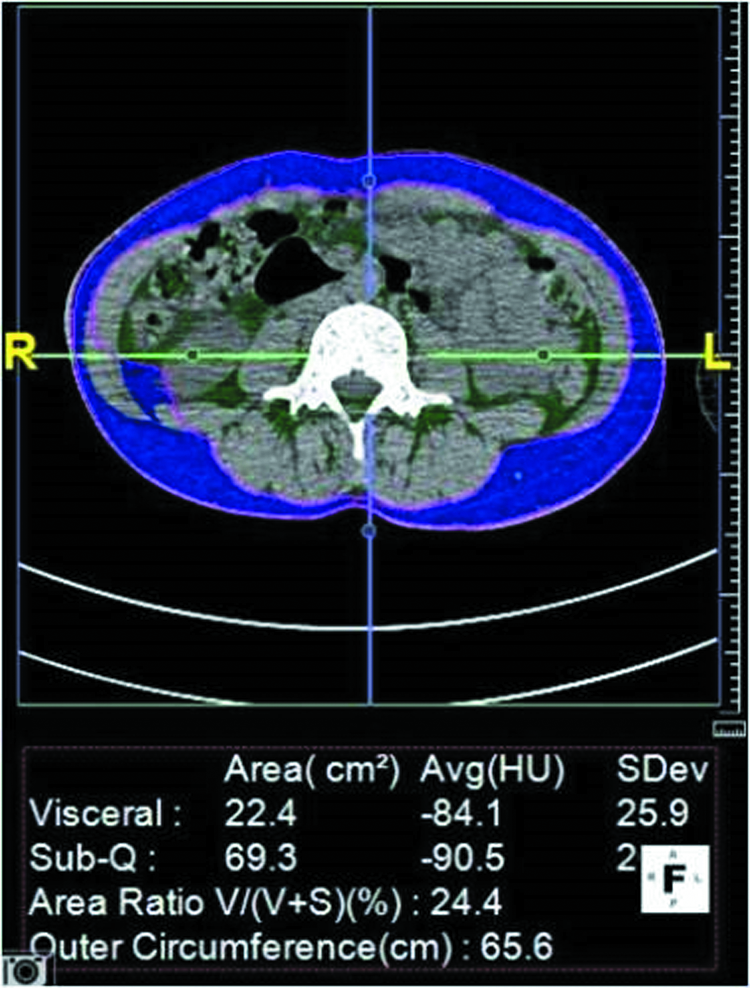
Cross-section area of visceral fat at second lumbar vertebra level. Visceral fat is indicated with green. A color version of this figure is available in the online article at www.liebert.pub.com/lrb.
Statistical analysis
Fisher's exact test was analyzed for correlation of obesity and abdominal obesity. To identify the risk factors that affect the obesity and abdominal obesity, Spearman correlation analysis was used for numeral factor and Wilcoxon test or ANOVA for categorical factors. Correlation analysis was used for the relationship of MCD and lymphoscintigraphy data. Factors with p-value being less than 0.05 were considered statistically significant. Area under receiver operating characteristic (ROC) curve of abdominal obesity was analyzed.
Results
Among the patients, 14 women (42%) were obese (BMI ≥25 kg/m2) and 19 (54%) had increased abdominal fat (Table 1). BMI obesity and abdominal obesity were significantly correlated, but five of the patients classified with abdominal obesity had a BMI of less than 25 kg/m2. There were no significant differences in age, time after surgery, cancer stage, history of axillary LN dissection, chemotherapy, or radiotherapy between patients with or without BMI or abdominal obesity. The mean circumference difference was 2.8 ± 2.4 cm (Table 2).
Significant difference (p < 0.05).
BMI, body mass index; CA, cross-section area.
LN, lymph node.
Positive, moderately strong correlations were observed between the MCD and upper limb QAI (r = 0.523, p = 0.002), indicating that both indices could be used to assess factors affecting disease severity (Table 3). In the assessment of whether BMI obesity or abdominal obesity was an aggravating factor of lymphedema, decreased axillary QAI was significantly correlated with BMI and increased arm edema (MCD ≥2 cm) was significantly correlated with abdominal obesity (Table 4). Axillary QAI had no significance with either obesity or abdominal obesity. Area under ROC curve was 0.572 for discrimination of abdominal cross-section area with increased arm edema. Cutoff value was 75.15 cm2 with 60% sensitivity and 72% specificity.
Significant difference (p < 0.05).
QAI, quantitative asymmetry index.
Significant difference (p < 0.05).
Discussion
Our study found that both indicators of obesity—BMI and abdominal fat cross-sectional area—were associated with lymphedema severity as assessed by lymphoscintigraphy (diagnostic scale) or MCD (clinical severity). Moreover, some patients had abdominal obesity despite a normal BMI, suggesting that measuring both indicators would provide increased reliability.
Obesity is a well-known risk factor for lymphedema after LN removal, and increased BMI is associated with increased frequency and severity of lymphedema. Werner et al. described that patients in the bottom 38th percentile of the BMI, the risk of severe arm edema was 0%, whereas for obese women in the top 23rd percentile, it was significantly higher. 20
Nevertheless, it is not clear whether obesity is a direct risk factor for developing lymphedema; however, it is certainly a risk factor for infection and poor wound healing after breast cancer surgery. 32 This supports the theory that delayed wound healing in obese patients is secondary to a cycle of fat necrosis, secondary infection, regional lymphangitis, and aggravating lymphatic obstruction. 33
Asians typically have smaller body size compared with western individuals, and there is a higher frequency of localized obesity, especially abdominal obesity with high visceral fat, rather than whole-body obesity in Asian populations. 34 In addition, previous studies have suggested that abdominal obesity is a better discriminator of comorbidity factors than is BMI.22,23 In our study, abdominal obesity was correlated with increased arm circumference.
In addition to arm circumference measurement, quantitative lymphoscintigraphic analysis was done in the assessment of the severity of lymphatic insufficiency. Weissleder et al. compared quantitative and qualitative lymphoscintigraphy in different grades of lymphedema and found that qualitative interpretation confirmed the diagnosis of lymphedema in only 70% of extremities, whereas quantitative analysis detected abnormal lymphatic function in all the examined limbs. 35 Our study also used QAI as the standard for our imaging-based severity assessment, and we found positive, moderately strong correlations between the MCD and upper limb QAI (exhibiting dermal back flow by LN obstruction), indicating that both indices could be used to assess factors affecting disease severity. In addition, Szuba et al. evaluated the utility of quantitative lymphoscintigraphic analysis in the assessment of the severity of lymphatic insufficiency. Consequently, there was no correlation between the axillary LN QAI and the initial measured edema volume, but significant correlation was found between the quantification of dermal back flow. 36 In our study, BMI was only correlated with axillary LN, but not arm QAI, which could reflect dermal backflow from a severe lymphatic obstruction. Otherwise, history of axillary LN dissection in 78.6% of obese patients could have effect on axillary LN QAI. In addition, as there were no correlations between the MCD and axillary LN QAI, axillary LN QAI can be less considered as a strong predictive factor compared to MCD and upper limb QAI.
In our study, we measured cross-sectional area of visceral fat of second lumbar vertebra (slightly above the umbilicus level) under CT, as it is more objective diagnostic tool than bioimpedance to assess abdominal obesity. When assessing abdominal visceral fat with CT, a single CT image is known to contain the same information on adiposity as a series of scans. 37 Radiation exposure due to CT studies of body composition can be limited by using single scans at different anatomical sites. If only a single scan at one site can be obtained, the level of the umbilicus is the most useful, because it contains the largest percentage of fat in the body. 37
In addition, obesity and abdominal obesity were significantly correlated, but five of the patients classified with abdominal obesity had a BMI of less than 25 kg/m2. The mean circumference difference of these patients was 4.2 ± 3.4 cm, which is larger than that of total patient. If BMI alone had been used as an obesity indicator in this study, five patients (27.7%) with normal BMI and abdominal obesity would have likely gone unidentified for potential aggravation of lymphedema.
Otherwise, there were some limitations to this study. First, the number of the participating patients was relatively small, and we had no control group data to compare. Second, as there was no data from before the onset of lymphedema, we could not analyze the effect of abdominal obesity as a risk factor of the development of lymphedema. However, analyzing clinical, radiologic data with abdominal obesity as an aggravating factor is a meaningful data for the ongoing therapeutic approach and alleviation of lymphedema after breast cancer.
Conclusions
We found that abdominal obesity was significantly correlated with increased MCD, suggesting that it should be considered as another aggravating factor in addition to BMI for evaluation of lymphedema severity.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of Pusan National University Hospital and informed written consent was obtained from all the study subjects.
Availability of Data and Material
The datasets generated during the current study are available from the corresponding authors on reasonable request.
Footnotes
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author's Contributions
Y.T.B., S.W.L., Y.L.J., and S.H.L. were responsible for data collection and provided comments on the article drafts. K.Y.K. and Y.S.S. contributed to the interpretation of data and provided comments on the final draft of the article. Y.B.S. and T.Y.K. provided administrative support for the study. J.A.Y. and M.J.S. were responsible for study conception, design, data analysis, and drafting of the work. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.