
Abstract
Abstract
The purpose of this study was to compare two methods, the sponge method and SOFTMEASURE, to evaluate the stiffness in lymphedema extremities. We investigated 12 lower extremities of six patients with lymphedema using the methods and compared the results with International Society of Lymphedema classification and lymphoscintigraphic staging. The average age was 53.8 years (43–70 years). We prepared three sponges with different hardness, each of them was numbered as 2, 4, or 6, for the sponge method. We compared the stiffness of the lymphedema extremities and recorded the number of the sponge that was most comparable in stiffness. SOFTMEASURE is a portable device used to measure Young's modulus of an object. Measurement was performed thrice for each extremity. We excluded the most extreme value and the average of the other two values was used for evaluation. The correlation coefficient between SOFTMEASURE and the International Society of Lymphology (ISL) stage was 0.79, and between SOFTMEASURE and the lymphoscintigraphic stage was 0.85 (indentation force of 0.5 N). The correlation coefficient between the sponge method and the ISL stage was 0.57, and between the sponge method and the lymphoscintigraphic stage was 0.54, which indicated an intermediate correlation. In conclusion, evaluation of the stiffness of the skin or subcutaneous tissue in the lymphedema extremities using SOFTMEASURE or the sponge method to assess lymphedema severity was easy and minimally invasive. Sponge method seemed to be more useful than SOFTMEASURE because it had higher correlation with the ISL staging and lymphoscintigraphic staging. Recognizing the change in stiffness is important for determining the therapeutic strategy of lymphedema.
Introduction
L
Lymphedema is unique compared with other etiologies of edema in terms of the stiffness of the skin. 4 This stiffness is partially due to fibrosis of the dermis and subcutaneous tissues, and partially due to protein-rich fluid accumulated between the fibrotic tissues. 5 Successful conservative treatment or a surgical procedure can decrease the stiffness of the extremities, which relieves the patients from symptoms, including difficulty in movement, heaviness, or pain. This suggests the importance of recording and assessing the stiffness of the skin or subcutaneous tissues in the evaluation of lymphedema.
The stiffness of the lymphedema limbs is difficult to assess objectively as the hardness of the limb could be due to the fibrotic changes or the accumulation of lymph fluids. In most of the reports on this subject, stiffness is recorded based on the subjective views of the patients or medical staffs. 6 Some articles also report measuring stiffness in extremities of patients with lymphedema using various devices, including elastography and tonometry.5–9 However, these devices are not common, and none is widely used to measure the stiffness of lymphedema extremities. Therefore, a convenient and reliable measurement device is desired.
Young's modulus has been used to evaluate the stiffness of industrial products or foods. 10 Recently, it has been used to assess the stiffness of tissues in human bodies.11–13 SOFTMEASURE (Horiuchielectronics Co., Ltd., Tokyo, Japan) is a device used to measure Young's modulus by using handy-type indentation testing system and has been already used for the human body (Fig. 1). 14
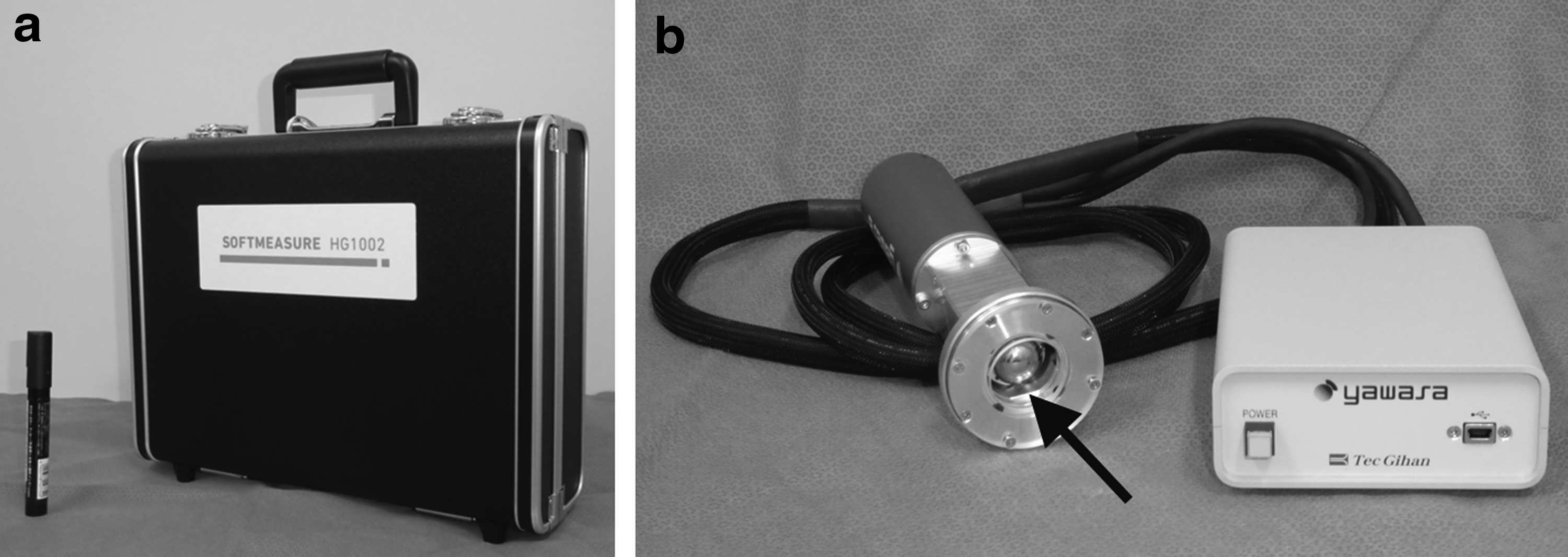
Photograph of SOFTMEASURE.
In this study, we used two methods to evaluate the stiffness of the lymphedema extremities: SOFTMEASURE and a sponge method. Establishing a tool for measuring stiffness will be helpful in determining a suitable therapeutic strategy for each patient. The purpose of this article is to report and compare these two methods to evaluate the stiffness in lymphedema extremities.
Patients and Methods
We investigated 12 lower extremities of six patients who were hospitalized in the Department of Lymphatic and Reconstructive Surgery, Saiseikai Kawaguchi General Hospital, between June and August 2016, and from whom written consent was obtained. Two methods, SOFTMEASURE and sponge method, are applied preoperatively for each patient to evaluate the stiffness of the lymphedema extremities.
The severity of lymphedema was evaluated and recorded by a well-experienced lymphatic surgeon (H.H. or M.M.) based on the International Society of Lymphology (ISL) classification. 15 The diagnosis of ISL stage was performed before using SOFTMEASURE or the sponge method. All six patients underwent lymphoscintigraphy, and staging was performed based on Maegawa classification. 16 Stiffness was evaluated at the medial side of the proximal thigh with the patient in the supine position, with the knee joint slightly flexed to release the skin tension.
The Sponge method was performed as outlined below. We prepared three types of sponges with different hardness (Yahata Neji Corp., Aichi, Japan), which were bought in a general shop (Fig. 2). The size of each sponge was 50 × 105 × 210 mm and the density was 20 ± 2.0 kg/m3, 35 ± 3.0 kg/m3, and 50 ± 5.0 kg/m3, respectively. Each sponge was numbered 2, 4, or 6, with no. 2 as the softest and no. 6 as the hardest. We compared the stiffness of the lymphedema extremities and the sponges and recorded the number of the sponge that was most comparable in stiffness. For example, if the stiffness of the extremity was most similar to that of sponge no. 2, we recorded “2.” If the stiffness of the extremity was harder than no. 2 and softer than no. 4, we recorded “3.” Accordingly, stiffness was expressed with numbers between 1 and 7. Assessing and recording were performed by a random general nurse or physiotherapist who took care of the patients in an outpatient clinic. These staff members were blinded to the patients' ISL stage or result of SOFTMEASURE.

Three types of urethane sponges used in the sponge method. The yellow one is numbered as 2, which is the softest (density of 20 ± 2.0 kg/m3). The orange one is numbered as 4, which is intermediately soft (density of 35 ± 3.0 kg/m3). The black one is numbered as 6, which is the hardest (density of 50 ± 5.0 kg/m3).
SOFTMEASURE (Horiuchielectronics Co., Ltd.) is a device used to measure Young's modulus of an object using a portable system of indentation testing, which costs about 1.7 million yen (Fig. 1). The ball indenter placed at the center of the probe is pushed out from the probe, and the stiffness of the material is calculated from the indentation distance and the indentation force. According to the elastic contact theory of Hertz, the relationship between the indentation force and the indentation quantity can be represented using the diameter of the ball indenter, Young's modulus E, and Poisson ratio v as below:
Then, the apparent changes of stiffness due to the thickness can be represented as below:
The diameter of the ball indenter was 10 mm. We set the maximum indentation forces as 0.5 and 2.0 N. Small indentation force seemed to measure the stiffness of the more superficial layer. We measured the stiffness of the lower limb thrice for both 0.5 and 2.0 N. Because the variability of the value was sometimes wide, we excluded the most extreme value and the average of the other two values was used for evaluation. The measurement was performed by the first author, who was blind to the results of the sponge method.
We calculated the coefficient of correlation between the results of SOFTMEASURE or the sponge method and the ISL stage or Maegawa classification, using Microsoft Excel.
Written informed consent was obtained from all patients following the approval of the ethics committee of the hospital (approval no. 26–6).
Results
All six patients had secondary lower limb lymphedema, and the average age was 53.8 years (43–70 years). The causative disease of the lymphedema was cancer of the uterine body in three patients, uterine cervical cancer in two patients, and ovarian cancer in one patient. The characteristics of the patients are shown in Table 1. All of them underwent pelvic lymph node dissection. The average lymphedema duration was 2.3 years (0.5–7 years). Five limbs were classified as stage 1 in ISL classification, two were stage 2a, four were stage 2b, and one was stage 3.
CT, chemotherapy; ISL, International Society of Lymphology; LC, lymphoscintigraphy; LND, lymph node dissection; RT, radiotherapy.
The result of the two evaluation methods is shown in Table 2. The relationship between the result of SOFTMEASURE and the ISL stage or lymphoscintigraphic stage is shown in Figure 3. The correlation coefficient between 0.5 N of SOFTMEASURE and the ISL stage was 0.79, and between 0.5 N and the lymphoscintigraphic stage was 0.85. The correlation coefficient between 2.0 N of SOFTMEASURE and the ISL stage was 0.77, and between 2.0 N and the lymphoscintigraphic stage was 0.75. All values indicated a strong correlation, and the correlation coefficient was generally higher in 0.5 N than in 2.0 N.
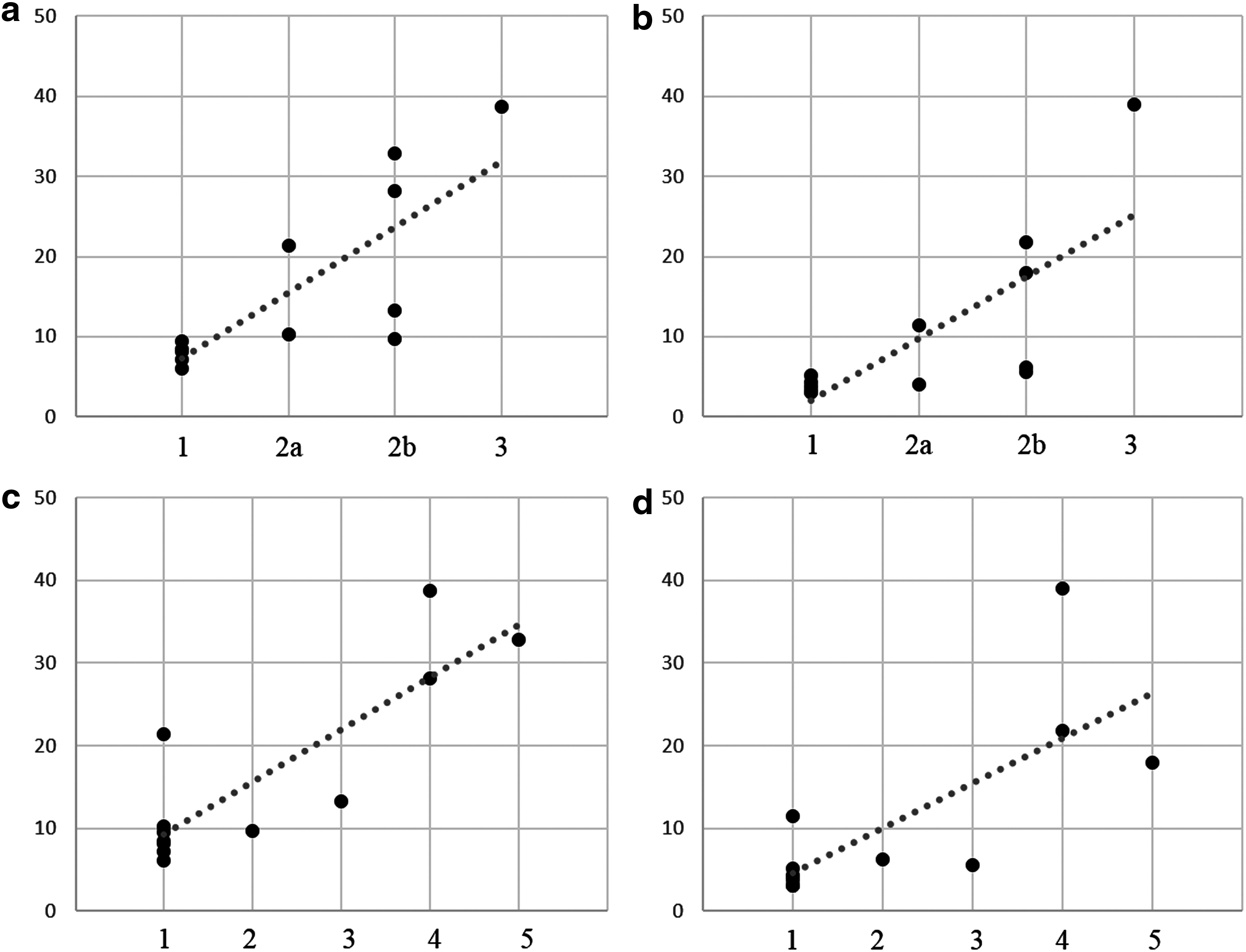
Relationship between the result of SOFTMEASURE and the ISL stage or Maegawa classification of lymphoscintigraphy. The vertical scale indicates the result of SOFTMEASURE, and the horizontal axis indicates the ISL or lymphoscintigraphic stage.
R, right; L, left; SM(0.5), 0.5 N in SOFTMEASURE; SM(2), 2 N in SOFTMEASURE.
The relationship between the result of the sponge method and the ISL or lymphoscintigraphic stage is shown in Figure 4. The correlation coefficient between the sponge method and the ISL stage was 0.57, and between the sponge method and the lymphoscintigraphic stage was 0.54, which indicated an intermediate correlation.
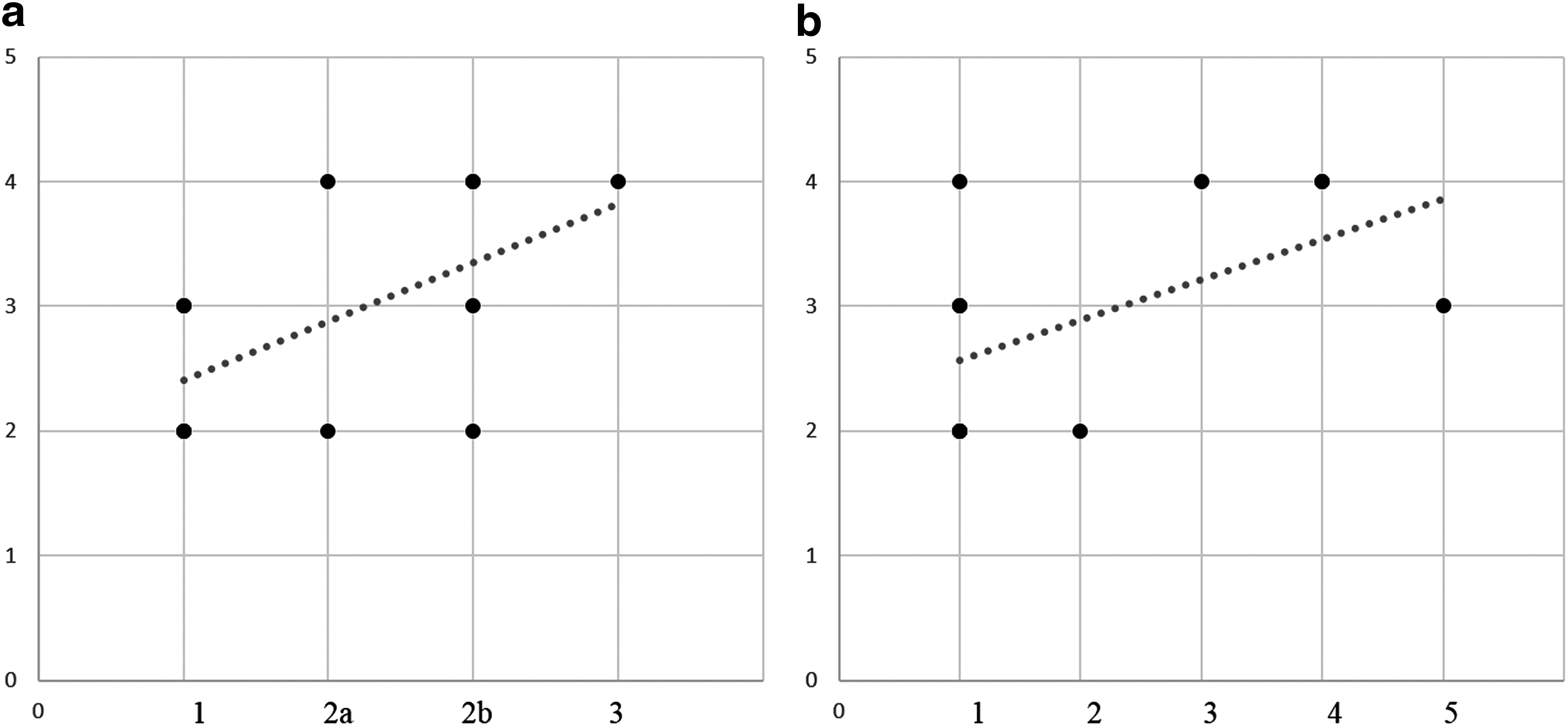
Relationship between the result of the sponge method and ISL stage or Maegawa classification of lymphoscintigraphy. The vertical scale indicates the result of the sponge method, and the horizontal axis indicates the ISL or lymphoscintigraphic stage.
The relationship between the result of SOFTMEASURE and the sponge method is shown in Figure 5. The correlation coefficient between 0.5 N of SOFTMEASURE and the sponge method was 0.65, and between 2.0 N and the sponge method was 0.62, which indicated an intermediate correlation.

Relationship between the result of SOFTMEASURE and the sponge method. The vertical scale indicates the result of SOFTMEASURE, and the horizontal axis indicates the result of the sponge method.
Discussion
In this article, we report the result of two methods used to evaluate the stiffness of the lymphedema extremities. SOFTMEASURE and the sponge method had strong and intermediate correlation with the ISL stage or lymphoscintigraphic stage. Both of these methods may be effective in evaluating the severity or the therapeutic course of lymphedema.
The stiffness is commonly used to evaluate treatment results objectively. Also, we sometimes use it for reference when we determine the indication of surgery. If the patient has a stiff extremity even though an appropriate compression therapy is applied, it seems to be a good indication of surgical treatment.
Currently, the most common way to evaluate the severity of lymphedema is volume or circumference measurement. However, clinically, some patients' affected limbs get softer after treatment, although the circumference remains the same. This softening indicates improvement of the lymphedema, and it is important to realize the improvement to select a correct therapeutic strategy. Furthermore, patients may be more motivated to continue treatment by noticing their improvement. On the contrary, hardening of the affected limb indicates aggravation of the lymphedema, and recognition of this is also important for accurate treatment. Recently, in addition to traditional conservative treatment, various surgical procedures are available for the treatment of lymphedema,17–21 and assessing and recording the stiffness of the affected limbs may help to determine which treatment is most appropriate.
The merit of the sponge method is its ease of use. The sponges used in the method can be cheaply purchased and are readily available. (They are about $3–5 each.) Moreover, as their degrees of hardness are expressed using an objective gauge of density, it is possible to share results among many hospitals or clinics in different countries. Furthermore, this method does not require a difficult procedure. Comedical staff members, including general nurses, physiotherapists, or lymphedema therapists, can easily perform the evaluation. Most importantly, patients themselves can understand this method, and this can lead to an early detection of aggravation. In fact, we had our patients touch the sponges in the outpatient clinic, explaining that the stiffness of their extremities is linked to lymphedema severity. Another merit of this method is minimal invasiveness with no pain, and short examination time of a few seconds.
The demerit of the sponge method is that it is not an objective examination, which may result in variability depending on the examiner. Staff members who are not used to lymphedema may accidentally evaluate the stiffness of muscle or bone instead of skin or subcutaneous tissue; therefore, staff education is necessary. Still, as the stiffness has been evaluated only by subjective tactile sensation for a long time, the sponge method must be a helpful tool to make the stiffness evaluation more objective.
The merits of SOFTMEASURE include objectivity and low invasiveness. Until now, stiffness of the extremities has been recorded as “soft” or “hard,” or using the visual analogue scale. 5 We could assess the stiffness of the extremities objectively using SOFTMEASURE, and this enabled us to evaluate the severity or therapeutic course of lymphedema. In addition, SOFTMEASURE is a light and portable device, which can easily be carried from an outpatient clinic to a patient ward, or even to other hospitals. Although multiple measurements are necessary for each extremity, due to data variability, it takes ∼10 seconds for one measurement, so total examination time is still relatively short.
Evaluation of the stiffness of an object using Young's modulus has been already performed in the area of orthopedics. The hardness of muscles or tendons is evaluated to diagnose the effectiveness of exercise or degree of fatigue.11–13 Stiffness evaluation based on Young's modulus may be widely used in evaluating lymphedema in the future.
The demerit of SOFTMEASURE is that it is a specific device that is not readily available. However, evaluating stiffness of tissues may be useful in other diseases, including backache or shoulder discomfort, because the stiffness of the muscles is related to the severity of the diseases. 22
We selected inner side of the thigh in this study for evaluation. We did not include the calf or ankle, because the subcutaneous tissue is sometimes very thin and there was a possibility that SOFTMEARURE evaluated the stiffness of muscle or bone that is located beneath the fat tissue.
We have one remaining question about which depth of the tissues does SOFTMEASURE evaluate. As it measures stiffness by compressing the indenter to the skin, it should evaluate the stiffness from the surface of the skin to some depth. An indentation force of 2.0 N indicates deeper indentation than 0.5 N, and it therefore must evaluate deeper tissue. In the affected limbs of lymphedema, non-pitting edema is observed with the accumulation of lymphatic fluid and proliferation of the fibrotic tissue. In this situation, when the subcutaneous tissue contains much fluid in lymphedematous limb, stiffness of the skin is considered to become large with the increased amount and inner pressure of the content. However, the change in the stiffness of the subcutaneous tissue alone in lymphedematous limb could not be evaluated in this study. Future research on this point is necessary, possibly combining elastography.8,9 Also, there is no comparison with tonometry or indurometry in this study, and it should be a future challenge. Also, the number of patients included in this study was small, and larger sample size would be necessary for further evaluation. The difference in the stiffness measured by these materials between nonpitting edema and pitting edema is still unknown.
Another limitation of this study was the variation of the stiffness of the limbs in lymphedema patients. Stiffness of the limbs is usually better in the morning than in the evening. Therefore, it seemed to be difficult to evaluate the severity of lymphedema only by stiffness. In this study, we measured the stiffness in the afternoon to reduce the bias.
In conclusion, evaluation of the stiffness of the skin or subcutaneous tissue in the lymphedema extremities using SOFTMEASURE or the sponge method to assess lymphedema severity was easy and minimally invasive. Sponge method seemed to be more useful than SOFTMEASURE because it had higher correlation with the ISL staging and lymphoscintigraphic staging. Also, it is cheap and accessible. Recognizing the change in stiffness is important for determining the therapeutic strategy of lymphedema. Future studies could help establish a competent method to evaluate the stiffness of lymphedema extremities.
Footnotes
Author Disclosure Statement
No competing financial interests exist.