
Abstract
Abstract
Background:
In the past, measurement of upper limb lymphedema was done by water displacement (WD), which is frequently cited as the gold standard. For various reasons, however, the use of WD is restricted in clinical settings. A more precise and easy-to-use method would be favorable. The high precision of three-dimensional (3D) imaging in comparison to WD has already been reported for healthy subjects. The aim of this study is to determine the validity and reliability of 3D imaging by comparing it to the WD method in women with unilateral upper limb lymphedema.
Methods and Results:
Thirty-nine women with unilateral breast cancer-related lymphedema (BCRL) were included, of which 37 completed two volume measurement techniques (3D and WD) on the BCRL and contralateral healthy arm. Slightly larger volumes were measured by the WD method in healthy arms (+9.8 mL; p = 0.058) and also in BCRL arms (+18.5 mL; p < 0.001). All measurements were performed twice by the same researcher to evaluate reliability. There was no significant difference between the two measurements for healthy arms (p = 0.323) or BCRL arms (p = 0.807) in 3D imaging. Bland–Altman plots showed a high limit of agreement between the single measurements. 3D imaging had a high intrarater reliability (Intraclass Correlation Coefficient = 0.999).
Conclusion:
Results show that 3D imaging is an innovative method for measuring upper limb volume in BCRL patients. Even though image processing is time consuming, 3D imaging combines high reproducibility with high precision. By software automation, this technique could easily be integrated into clinical routine. It is for this reason that we would recommend implementing the Vectra 3D imaging technique for measurement of BCRL.
Introduction
I
In healthy subjects, interstitial fluid is transported into the initial lymphatics and pumped through larger more proximal collecting ducts to various lymph nodes. 9 In BCRL, microvascular filtration rates from capillaries and venules exceed lymphatic drainage capacity. This results in the stasis of lymphatic fluid which accumulates in the interstitial spaces, causing the respective arm to increase in volume. 9 As a result, range of motion is impaired, and patients report arms that feel heavy, painful, and weak.10,11 This can lead to a reduction in quality of life.10,12
Even though a high number of patients are diagnosed with BCRL and definitions exist, a precise and efficient measurement method for all patients is still missing.13,14 Knowledge about the exact arm volume is important to detect the first signs of lymphedema and to follow the progressive and regressive effects of the treatment.14,15 Most commonly used thresholds for the definition of lymphedema of the upper limb range from physical measurements (>200 mL absolute interlimb volume difference, >8%–10% relative interlimb percentage difference, and >2 cm circumference difference between the two arms) to subjective reports of limb heaviness.16,17
Nevertheless, there is no commonly accepted and standardized method for volumetric measurement of the upper limb. Over the years, many techniques have been developed to measure the volume of the arm. These include water displacement (WD), limb girth through tape measurements, and infrared laser perometry. 18 In most studies, WD volumetry is used as the gold standard. 19 It is an inexpensive, safe, and painless method of measurement. However, use of WD is restricted for various reasons; it is time consuming, the maximum arm volume is limited, and patients may experience difficulties bending over to fully place their arm into the water.20,21 Furthermore, results depend on the patients' capability to cooperate, as movements have to be done slowly and smoothly to reduce undulation. In addition, there is a small risk of cross-infection among patients and subjects with open wounds (e.g., skin infections, ulceration, or psoriatic plaques). 21
Therefore, an accurate, convenient, and objective method for measurement of arm volumes is necessary. Three-dimensional (3D) measurement is a relatively new technique which has been proven to be reliable. 22 A variety of 3D systems have been developed, including the Vectra 3D imaging system, which has been used in the past for volume measurements of the face, keloid scars, and breasts.23–26 In 2014, the Vectra XT 3D imaging system (Canfield Imaging Systems, Fairfield, N.J.) was proven to be valid and reliable for the measurement of healthy arms. 22 However, 3D imaging by Vectra XT is not yet verified for patients with lymphedema in the upper limb. Therefore, this study aims to investigate the reliability of Vectra XT for the measurement of arm volumes in BCRL patients and to compare these results to volumes obtained by WD (gold standard).
Materials and Methods
Ethical approval
Approval for this study was obtained from the Medical Ethics Committee of Maastricht University Medical Centre (MUMC+). Written informed consent was obtained from each subject before participation in this study. All patients participated voluntarily. This study was performed in accordance with the principles described in the Declaration of Helsinki.
Participants
To be eligible for this study, women were required to be a minimum of 18 years old and report one-sided BCRL. Women were defined as having one-sided BCRL when they had an interlimb volume difference of >200 mL measured by WD, complained of one-sided arm swelling, or were currently undergoing unilateral treatment for lymphedema. Patients with BCRL also present with small volume differences between the arms in clinical practice. Therefore, women with an interlimb volume difference of <200 mL were included in this study when they reported at least one other condition. Exclusion criteria were open wounds on hands and arms, metastases, recurrence of breast cancer, bilateral lymphedema, disorders affecting the participants' ability to cooperate, or an arm volume higher than 4000 mL (as higher volumes could not be measured in the water basin).
In total, 39 women with one-sided BCRL volunteered to participate in the study at MUMC+ between September 2016 and June 2017. The study was performed at the outpatient clinic in conjunction with the patients' regular appointments. Two participants were excluded; one due to an arm volume exceeding 4000 mL and one due to inability to complete measurements because of overlapping appointments. Therefore, the results of 37 women were used for analysis.
Study design
For the study, patients were measured by two methods. First, WD was performed and then 3D photographs with Vectra were taken. Participants were asked to wear no compression garments or undergo therapy 24 hours before the visit. Clothing covering the arms and jewelry were removed.
Before WD and 3D measurements, the sections of interest were measured with measuring tape (1 mm accuracy) and marked with a surgical pen. Lines were marked by cutoff points based on a previously published study by Erends et al., proximal at 80% and distal at 30% of total arm length (Fig. 1). 22 The total arm length was measured from the tip of the third digit to the acromion. The hand was excluded from the calculation, as Vectra is not validated for hands due to larger measurement inaccuracies. 27 Five reference points were drawn on the dorsal and ventral sides of both arms to facilitate the analysis of images. Volumes of both arms—the affected and the nonaffected—were measured twice by each method. Preparation of both arms took on average 20 minutes, and a further 25 minutes was required to carry out WD and Vectra 3D measurements. All measurements and calculations were conducted by one researcher.
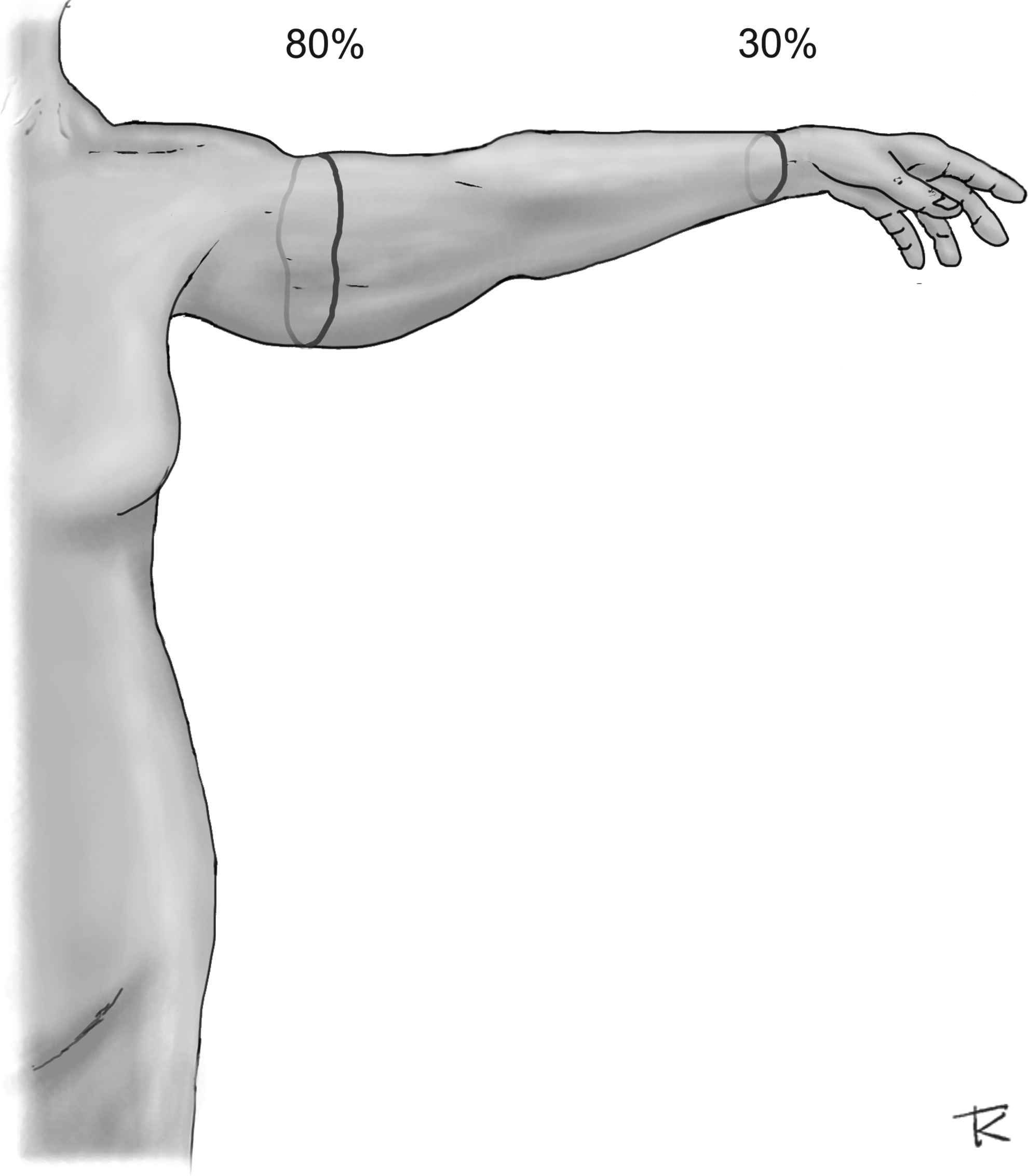
Predefined cutoff points at 30% and 80% of total arm length and positioning of the arm during marking, as well as 3D photography. 3D, three dimensional.
WD method
A bravometer (Varitex, Haarlem, The Netherlands) based on the Archimedes' principle was used for volume measurements (Fig. 2). 28 The bravometer is a water filled container which is adjustable according to patient height and utilizes an integrated calibrated scale that is accurate to 1 mL. This apparatus was filled with tap water, the temperature of which ranged from 25°C to 32°C. Water temperature in the range of 20°C to 32°C was found to not affect volumes measured. 29 Healthy and BCRL arms were measured alternately to reduce the impact of surrounding air temperature and to ensure equal familiarization for both arms with the technique. 30 Before every measurement, the weighing scale was calibrated to zero.

Bravometer (Varitex, Haarlem, The Netherlands).
Participants stood next to the water basin. They were asked to slowly immerse their hand until the 30% line reached the surface of the water. Displaced water moved from the basin into a separate overflow container. This primary overflow was measured and the container emptied. The scale was calibrated back to zero. Afterward, the arm was lowered into the water until the 80% line was reached. Participants were asked to momentarily avoid moving, as this reduced false flow of water between basin and overflow. Contact of the arm with the water basin was avoided when possible to prevent excess skin or adipose tissue sitting above the water surface. The arm was removed and dried. Secondary overflow was measured. Measurement results were converted from kilograms (kg) to milliliters (mL) using the standard conversion for water of 1 kg being equal to 1000 mL.
3D volume measurement
3D measurements were carried out using the Canfield Vectra XT surface photo imaging system (Canfield Imaging Systems, Fairfield, NJ), which was calibrated daily before usage (Fig. 3). The Vectra camera system consists of six color cameras with a capture time of 3.5 milliseconds that are positioned in a triangulated configuration. Due to the variety of angles, the system is able to capture 3D images in 180°. 31

Vectra XT 3D imaging system (Canfield Imaging Systems, Fairfield, NJ).
Participants were asked to stand ∼70 cm in front of the camera. All subjects were instructed to hold arms horizontally, with their palms facing down (Fig. 1). Exact positioning was reached with the aid of the researcher. To evaluate the volume of the upper extremity, two images were taken from the anterior and posterior side of both arms. Data were automatically merged into a high resolution 3D 180° image and saved in the Vectra system. The 180° images with the best visibility of landmarks were chosen by the researcher for constructing a 360° digital model (Fig. 4). In total, two models were constructed for each arm. For processing, Mirror PhotoFile and Mirror PhotoTools (Canfield Imaging Systems software) were used. Previously marked 30% and 80% lines were used as cropping points and, therefore, marked the edges of the model. Volume inside the model was calculated using closed surface measurement. Capturing one suitable photo from each side of the arm took ∼2 minutes. Processing the images took on average, a further 5 minutes per arm.

Thee-dimensional images of the arm. Top: Landmarks are set on each of the 10 reference points; Middle: The two 180° images are merged together into one 360-degree model; Bottom: Edges are removed using the cutoff lines, and volume inside the model is calculated.
Statistical analysis
For power analysis, p < 0.05 was considered as the level of significance, and a power of 1−β = 0.80 was handled. Using Cohen's d, a medium effect size of d = 0.50 was chosen. Calculation determined a required study population size of 33 participants. Patient characteristics and results were described using descriptive statistics. The mean and standard deviation are given for continuous variables. Absolute numbers and relative frequencies are used when applicable.
Pearson correlation coefficient was used to assess the association between WD and 3D imaging for both arms. Paired-samples t-test was applied to determine the mean volume difference between WD and 3D imaging, but also to assess the mean volume difference between the single (first and second) measurements of WD and 3D imaging. Bland–Altman plots were used to analyze the agreement between WD and 3D. They were also used to analyze agreement of single measurements for both techniques separately. Intrarater reliability of WD and 3D measurements was determined through using Intraclass Correlation Coefficient (ICC). Inter-rater reliability was not assessed, as a high inter-rater reliability for Vectra has already been proven in a previous study. 22 A significance level of ≤0.05 was considered as statistically significant. For statistical analysis, IBM SPSS Statistics for Windows (Version 23.0, Armonk, NY: IBM Corp.) was used.
Results
Patient characteristics
Before the measurements, baseline characteristics and treatment history were collected from each woman (Table 1). The whole set of measurements was taken within a maximum of 1 hour. The mean age at time of measurement was 55.0 years (standard deviation [SD] 10.2), the mean BMI was 25.2 (SD 4.2), and mean arm length was 70.6 cm (SD 3.1) for both arms. The median duration of lymphedema was 55.0 months (range 3–252 months) before presentation. Twenty-one participants (56.8%) had lymphedema on their dominant arm.
3D, three dimensional; SD, standard deviation; WD, water displacement.
Validity
Figure 5 depicts a plot of the average volumes measured by WD and 3D for healthy arms and Figure 6 for arms with lymphedema. Comparison between WD and 3D showed a high correlation for healthy arms (0.996) and even higher for arms with lymphedema (0.998). WD technique measured slightly larger volumes (+9.8 mL; SD 30.5) compared to 3D imaging in healthy arms. Also, larger volumes were obtained by WD (+18.5 mL; SD 26.0). Paired-samples t-test showed that this mean volume difference was not significant for healthy arms (p = 0.058), but significant for arms with lymphedema (p < 0.001). Bland–Altman plots (Figs. 7 and 8) demonstrated a high agreement between the average values of WD and 3D imaging. More specifically, in healthy and in BCRL arms, 86.5% and 89.2% of the mean volume differences were less than 50 mL. Volume differences between WD and 3D ranged from −37.0 mL to +89.5 mL in healthy arms (Fig. 7) and from −35.5 mL to +64.0 mL in arms with lymphedema (Fig. 8).
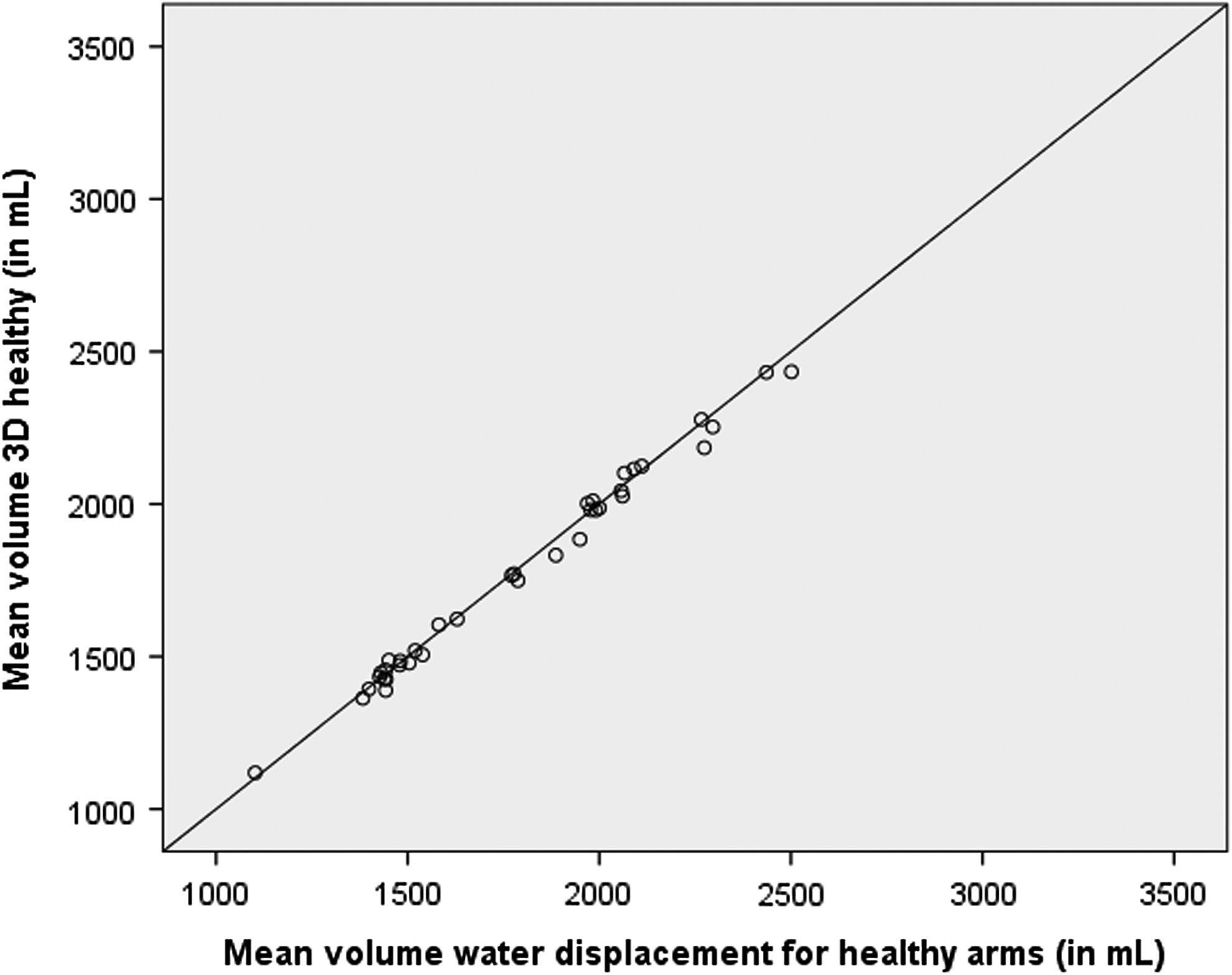
Plot of average values of water displacement versus 3D imaging for healthy arms (in mL).
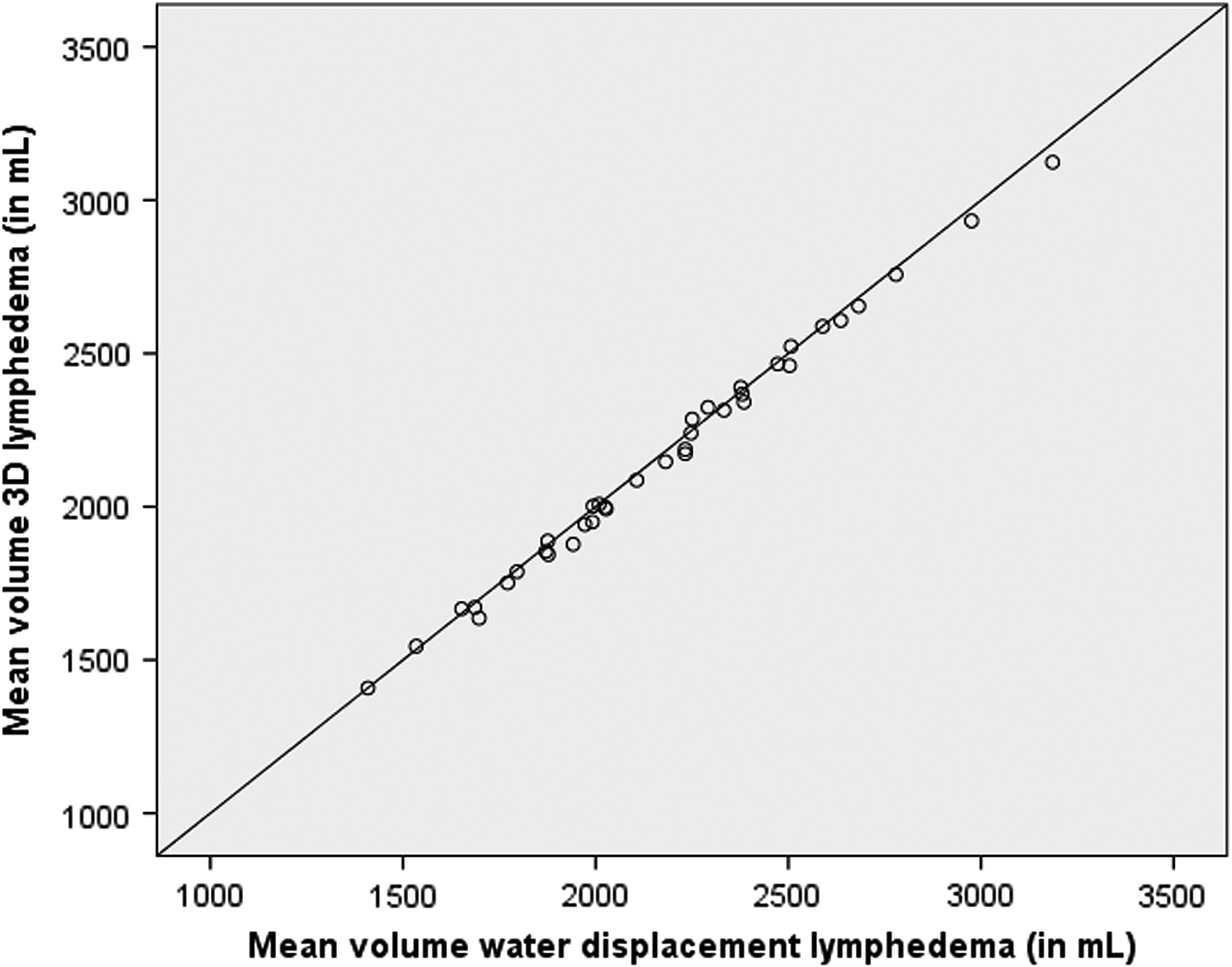
Plot of average values of water displacement versus 3D imaging for arms with lymphedema (in mL).

Bland–Altman plot of water displacement and 3D imaging for healthy arms (in mL).
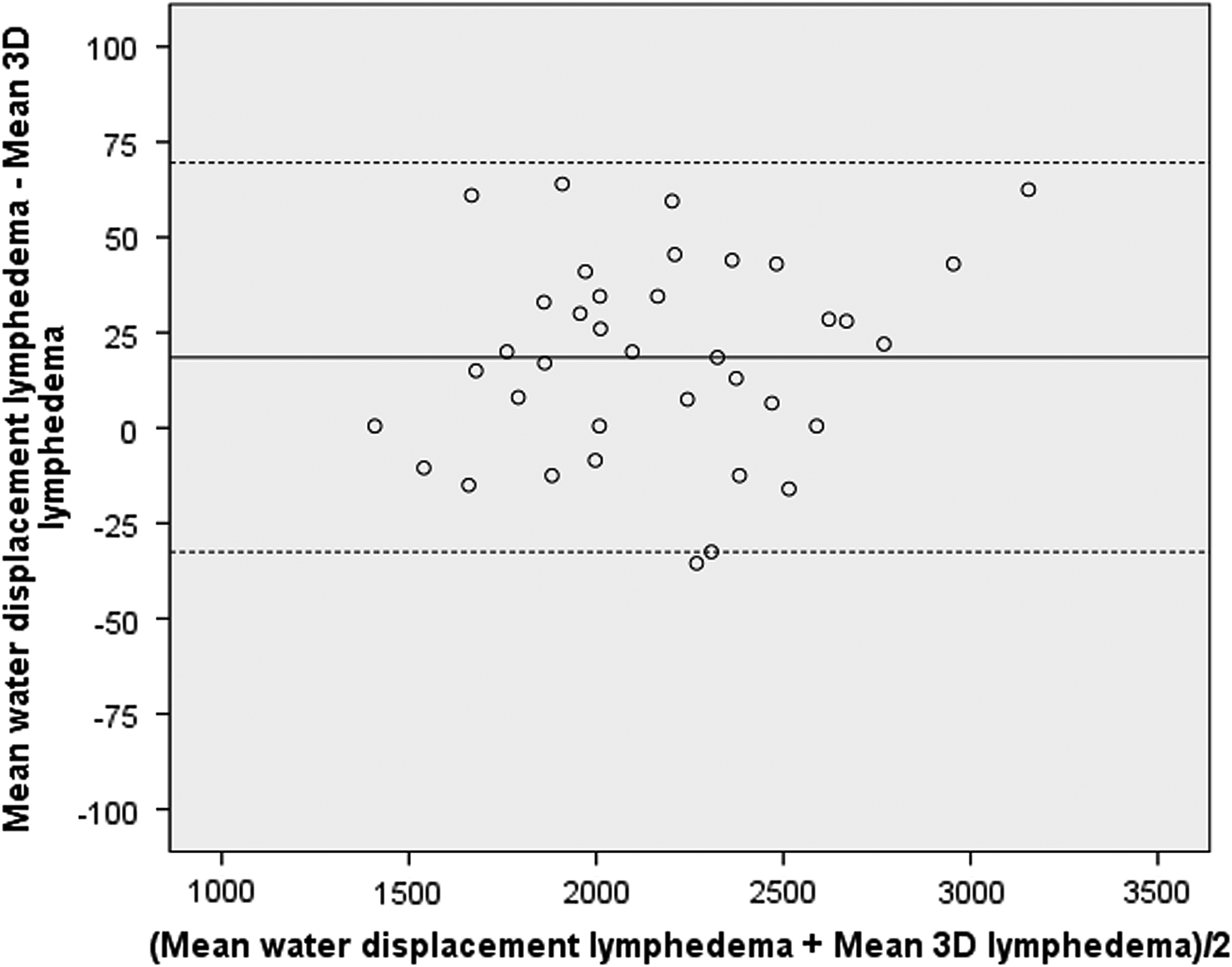
Bland–Altman plot of water displacement and 3D imaging for arms with lymphedema (in mL).
Reliability
The intrarater reliability for WD measurements was high for healthy arms and arms with lymphedema (both ICC = 0.998). Paired-samples t-test revealed neither a significant difference between the first and second WD measurement for healthy arms (p = 0.152) nor for arms with lymphedema (p = 0.395). The mean volume difference between the two WD measurements was +5.14 mL (SD 21.4) for healthy arms and +3.24 mL (SD 22.9) for BCRL arms. Bland–Altman plots (Figs. 9 and 10) indicated a high agreement between the first and second WD measurements with differences ranging from −35.0 mL to +50.5 mL for healthy arms (Fig. 9) and from −38.0 mL to +62.0 mL for arms with lymphedema (Fig. 10).

Bland–Altman plot of single water displacement measurements for healthy arms (in mL).
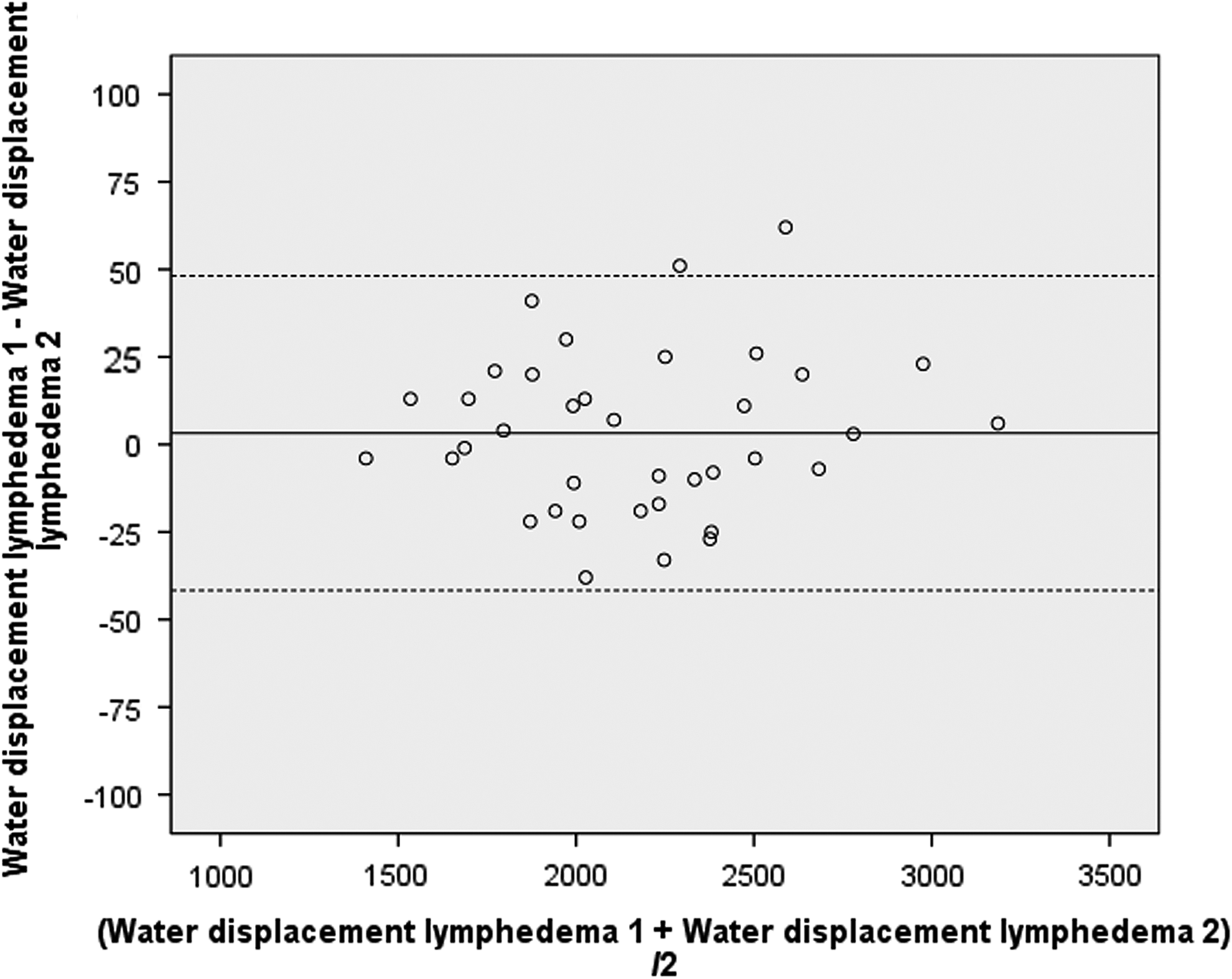
Bland–Altman plot of single water displacement measurements for arms with lymphedema (in mL).
Volume measurements performed by 3D imaging also showed a high intrarater reliability for both arms (both ICC = 0.999). Paired-samples t-test showed no significant mean volume difference between the first and second measurement for healthy arms, +2.51 mL (SD 15.3; p = 0.323), nor for arms with lymphedema, −0.60 mL (SD 14.7; p = 0.807). Bland–Altman plots reveal that 3D has a higher agreement than WD (Figs. 11 and 12). Differences between the first and second 3D measurement ranged for healthy arms from −28.0 mL to +38.0 mL (Fig. 11) and for arms with lymphedema from −36.0 mL to +35.0 mL (Fig. 12).
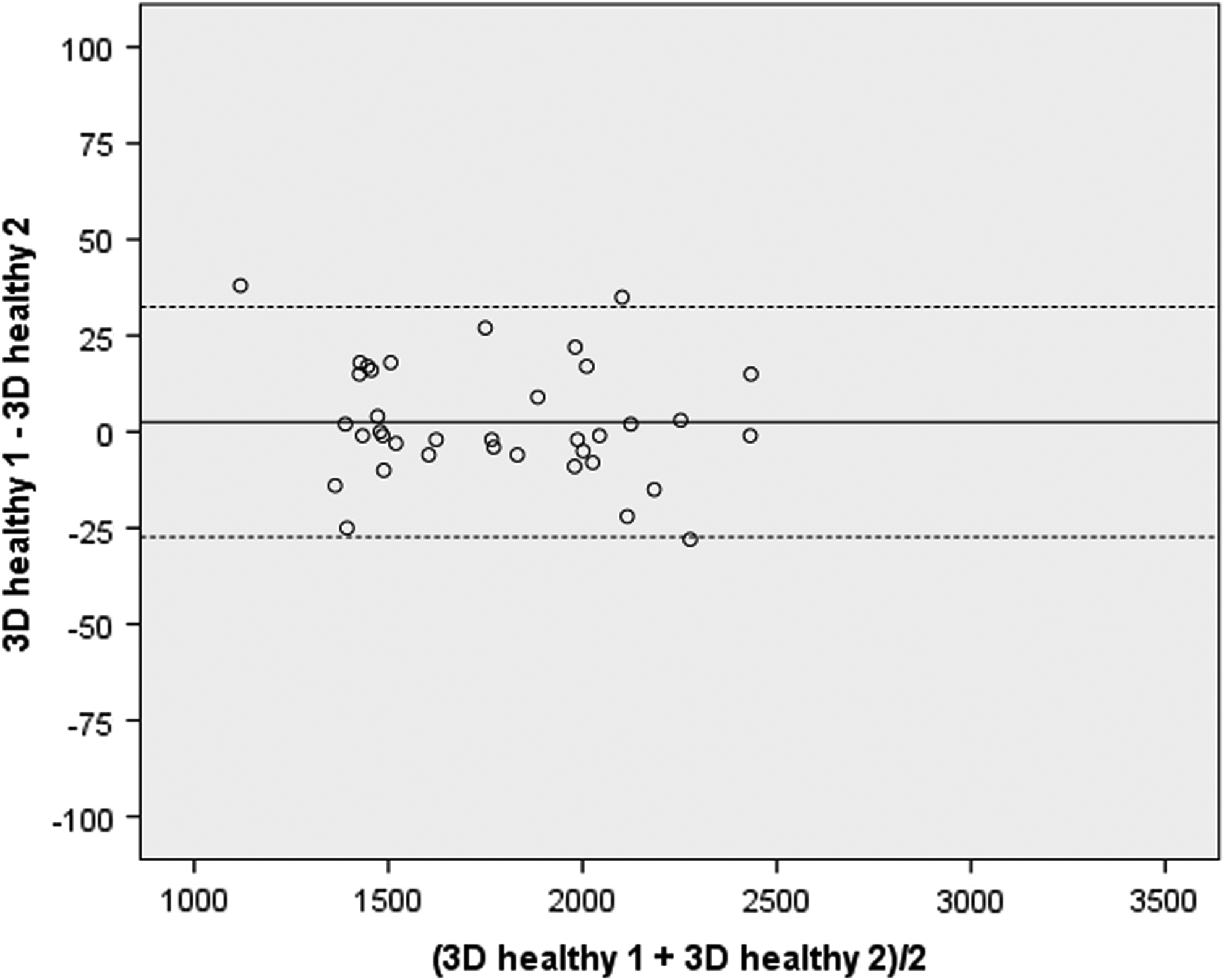
Bland–Altman plot of single 3D measurements for healthy arms (in mL).

Bland–Altman plot of single 3D measurements for arms with lymphedema (in mL).
Discussion
This study demonstrated that there was a small but significant difference between the WD and Vectra 3D when measuring arms with lymphedema. However, the level of agreement between these two methods was still high. Furthermore, this study showed that 3D imaging has an excellent reliability for measuring volumes of BCRL arms. A high level of agreement between the two 3D measurements was also seen by Hameeteman et al., who compared 3D stereophotogrammetry to WD in patients with lymphedema. 32 In contrast to the results published by Erends et al., this study revealed higher arm volumes for the WD method than for 3D imaging. 22 This may be due to heaviness, stiffness, altered sensation, and high arm volume in BCRL patients, which led to difficulties in holding the arm in a steady position. At times, instability of the arm might have led to subtle sloshing and therefore may have caused undulated overflow. This may have resulted in an overestimation of arm volume.1,33 Gjorup et al. described similar difficulties leading to possible measurement errors in WD. 33 Another reason that could have led to overestimation of arm volumes by WD is that the marking of arms is performed in the horizontal axis. Measurement of the arm in the water basin however is performed in the vertical axis, causing excess skin folds and adipose tissue on the dorsal side of the arm to push down, resulting in different angles of the 80% line when reaching the water surface (Fig. 13).

Positioning of the arm during the water displacement measurement; excess skin folds push down, leading to an uneven line.
As the 3D imaging technique takes only milliseconds to conduct, it is not vulnerable to the same measurement errors as the WD method. Captured images provide the opportunity for a variety of processing without burdening the patient. However, taking 3D photos with visible reference points, especially image processing on the computer and calculation of the volume, is time consuming. Indeed, researcher experience results in a faster capturing and processing technique, but the procedure is still lengthy. Using 30% and 80% lines for calculations is advantageous as it allows for individual standardization according to arm lengths. However, in a clinical setting, lines might be marked by different examiners, producing larger errors. Furthermore, palpating the acromion may be difficult in patients with a high BMI. It may also be hard for the examiner to draw an accurate line around the upper arm, especially when individuals have large, loose skin folds. On the contrary, except for the impossibility to measure hand volumes, 3D imaging can be performed without restrictions caused by arm volume, skin infection, immobility, or fragility due to age. 27 It must, however, be considered that a Vectra 3D scanner is costly and might not be available at every clinical center.
Both measurement techniques were well tolerated by all participants. Participants of this study were representative of women with BCRL. Baseline characteristics such as age, BMI, and history of axillary lymph node dissection were highly consistent with those of other studies.26,32,33 Inclusion and exclusion criteria were well chosen. Although the inclusion criteria concerning the diagnosis of lymphedema were broad, results show that mean volume differences between healthy and BCRL arms were evident. The study population was therefore a good reflection of the wider lymphedema population.
Conclusion
This study shows that three-dimensional volume measurement by Vectra XT is a safe, reliable, and valid method to measure arm volumes in patients with BCRL. It is a suitable option to replace the WD technique, although it is time consuming for the investigator. Looking toward the future, a fully automated volume measurement method that offers the possibility to calculate segmental volumes by computer would be most desirable.
Footnotes
Acknowledgment
The authors express their gratitude to Todor Krastev for his support in creating the images.
Author Disclosure Statement
No competing financial interests exist.