
Abstract
Abstract
Background:
Primary idiopathic lymphedema is an uncommon condition that typically affects the lower extremities. Patients have a malformed lymphatic system that causes subcutaneous fluid and adipose deposition. Rarely, the disease also has been described in the upper extremities. The purpose of this study was to investigate a cohort of patients with primary arm lymphedema to better understand the disease.
Methods:
Patients evaluated in our Lymphedema Program between 2008 and 2018 were reviewed for individuals with upper extremity primary lymphedema. Gender, age of onset, morbidity, associated features, and management were identified. Transit of radiolabeled tracer and dermal backflow on lymphoscintigraphy were recorded.
Results:
Twenty-three patients of 234 individuals with primary lymphedema had upper extremity disease (9.8%). Eleven subjects were male. Age of onset was infancy (n = 15), adolescence (n = 5), or adulthood (n = 3). The disease affected the left arm (n = 11), right arm (n = 9), or both upper extremities (n = 3). Lymphoscintigraphy in 15 patients exhibited delayed transit of tracer and 2 illustrated dermal backflow. One-half of individuals also had primary lower extremity lymphedema (six unilateral and six bilateral). None of the patients in the cohort exhibited a family history of lymphedema. Two individuals had Turner syndrome. Morbidity included infection (n = 5), other lymphatic anomalies (n = 6), and lymphangiosarcoma (n = 1).
Conclusions:
The upper extremities are a rare location for primary lymphedema and patients often also have lymphedema of the legs. Compared with that of the lower extremities, primary disease of the arm is more likely to be associated with systemic lymphatic dysfunction and has a lower risk of familial transmission.
Introduction
The most common etiology of lymphedema is secondary disease from injury to axillary or inguinal lymph nodes. Primary idiopathic lymphedema is rare, affecting ∼1/100,000 children 1 and comprises <1% of lymphedema cases. The disease almost always involves the lower extremities, but the arms may be affected. Primary upper extremity lymphedema typically has been described in case reports,2–9 in association with Turner syndrome,10,11 or in larger series on lower extremity disease.1,12–14 The purpose of this investigation was to analyze patients with primary upper extremity lymphedema to better understand the condition.
Methods
Patients evaluated in our Lymphedema Program between 2008 and 2018 were reviewed for individuals with primary lymphedema. Subjects with primary upper extremity lymphedema then were further evaluated. Diagnosis was made by history, physical examination, and lymphoscintigraphy. Clinical severity was documented based on the International Society of Lymphology criteria of increased limb volume: mild <20%, moderate 20%–40%, severe >40%. Gender, age-of-onset, morbidity, associated features, and lymphoscintigraphy imaging results were recorded. Abnormal lymphoscintigraphy findings included delayed transit of radiolabeled tracer to the axillary or inguinal nodes and dermal backflow.15,16
Results
Twenty-three patients out of 234 (9.8%) individuals with primary lymphedema in our database had upper extremity disease (Table 1). Eleven subjects were male. Age of onset was infancy (n = 15), adolescence (n = 5), or adulthood (n = 3) (Fig. 1). The disease affected the left arm (n = 11), right arm (n = 9), or both upper extremities (n = 3). Increased limb volume was mild (n = 10), moderate (n = 4), and severe (n = 9). We did not observe an association between location of lymphedema, lymphoscintigraphy findings, or disease severity.
Onset of isolated primary upper extremity lymphedema.
Phenotypes of Primary Upper Extremity Lymphedema
Axillary nodes of affected arm had significantly less radiolabeled tracer uptake at 45 minutes than nonaffected extremities. (—) Not performed.
BLE, bilateral lower extremity; BUE, bilateral upper extremity; F, female; LLE, left lower extremity; LUE, left upper extremity; M, male; RLE, right lower extremity; RUE, right upper extremity; GLA, generalized lymphatic anomaly; GI, gastrointestinal.
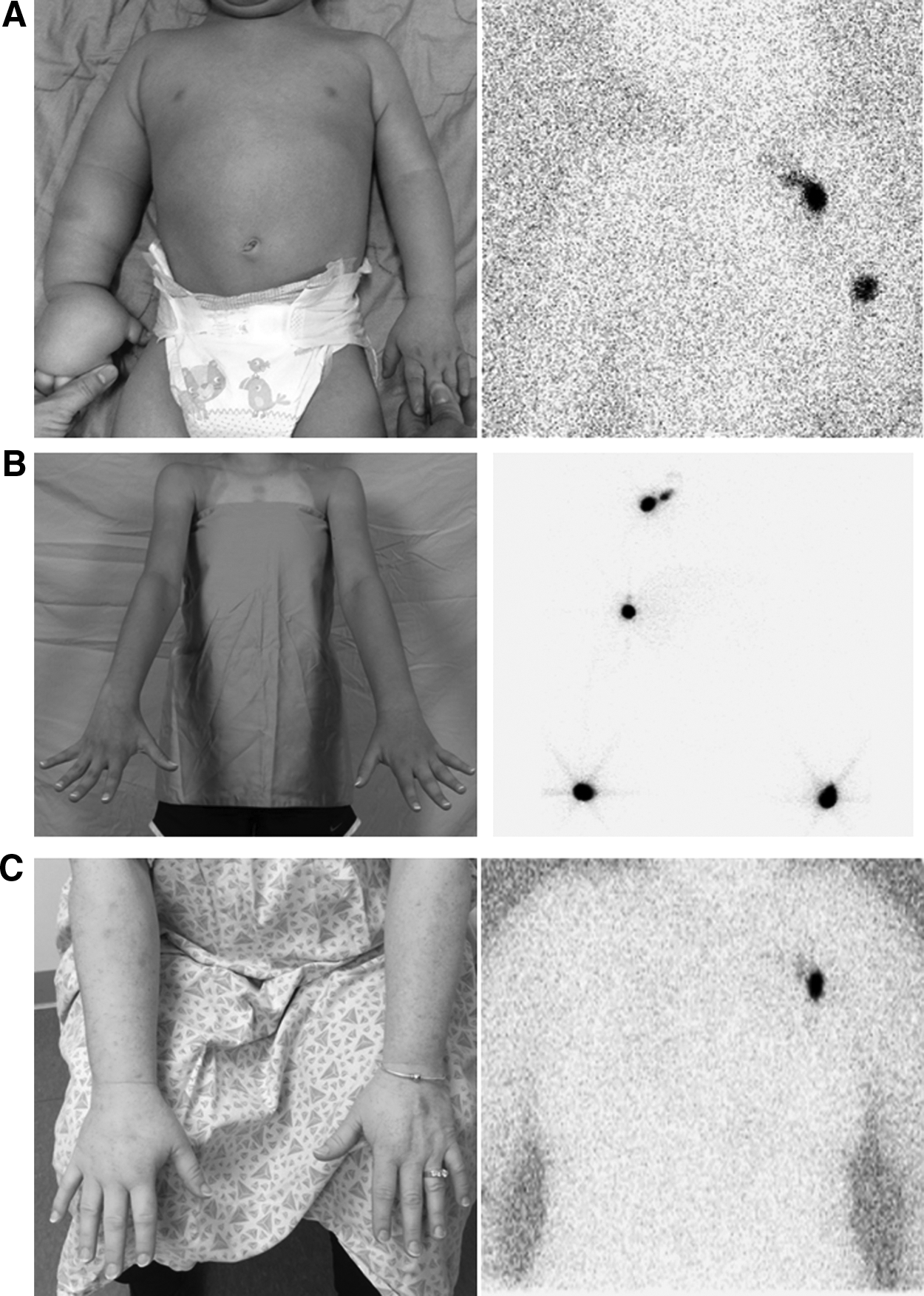
Fifteen patients had a lymphoscintigram at our institution using a standard protocol. Twelve subjects did not have tracer uptake into the axillary nodes at the completion of the study 4 hours after injection of the radiolabeled colloid into the hands. Three patients exhibited minimal tracer accumulation into the axillary nodes of the affected arm 45 minutes after injection that was significantly less than the contralateral normal extremity. Two subjects exhibited dermal backflow on the study indicating tracer accumulation in the dermal lymphatics. Twelve individuals exhibited primary lower extremity lymphedema (6 unilateral, 6 bilateral), and 2 of these had Turner syndrome (Fig. 2). None of the patients in the study had a family history of lymphedema. Six individuals (26%) exhibited systemic lymphatic anomalies that included gastrointestinal lymphangiectasia, pleural effusions, chylous ascities, microcystic lymphatic malformation of the face, and/or bone and spleen lesions. Five patients experienced an infection and one developed lymphangiosarcoma.
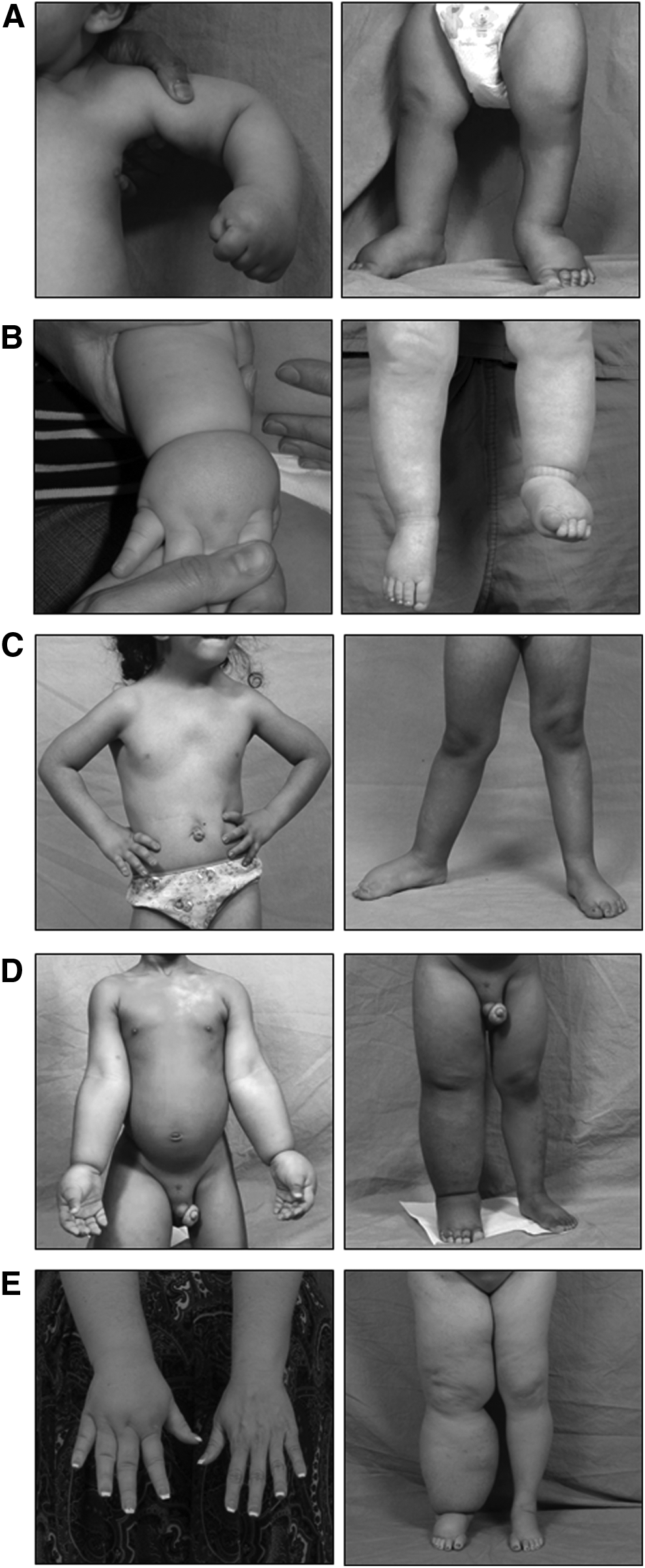
Phenotypes of primary upper extremity lymphedema.
Discussion
Ten percent of patients referred to our Lymphedema Program with primary lymphedema had arm involvement, which is comparable with other series of primary lymphedema: 4% (1/25), 13 6% (6/107), 12 10% (5/52), 17 and 11% (14/125). 1 Males and females were affected equally, similar to findings of other authors. 18 One-half of patients also had lymphedema of one or both of their legs. In contrast, only 5% (12/222) of patients with primary lower extremity lymphedema in our database have the disease of the upper extremities. Six subjects (26%) had systemic lymphatic dysfunction, which is greater than for patients with lower extremity lymphedema. 19 Age of onset of arm lymphedema was similar to that for the lower extremities.12,19,20 Three patients had bilateral arm involvement (13%), whereas primary leg lymphedema affects both legs in 50% of cases. 19 The risk of lymphangiosarcoma might be greater in primary upper extremity lymphedema compared with lower extremity lymphedema. The only patient with lymphangiosarcoma in our experience was a patient with primary arm disease (1/23), compared with no cases in individuals with primary lower extremity disease (0/222). Other examples of lymphangiosarcoma arising in primary arm lymphedema have been described.2,7
Thirteen percent of our cohort exhibited dermal backflow by lymphoscintigraphy compared with 31% of patients with primary lower extremity lymphedema. 21 This may be explained by the underlying lymphatic structural anomaly. Lymphangiographic studies of primary lower extremity lymphedema showed that 56% have hypoplastic lymphatics, 14% have aplasia, 6% only exhibit dermal backflow, and 24% associated with combined vascular malformations (e.g., Klippel-Trenaunay, Parkes Weber syndromes) have hyperplastic lymphatics. 12 Because lymphangiographic studies of primary upper extremity lymphedema have not been performed, the underlying anatomy is unknown. Patients with primary arm lymphedema might have a different pattern of underlying lymphatic structural anomalies. Proximal transit of lymphatic fluid against less gravitational force compared with the leg also might influence the presence of dermal backflow.
Several mutations have been identified in patients with primary lower extremity lymphedema (e.g., VEGFR3, FOXC2, SOX18, and PTPN14). 14 Two mutations have been associated with primary arm lymphedema in combination with lower extremity disease and other abnormalities (GJC2 and CCBE1). 14 Patients with Turner syndrome (45, X) have an ∼50% risk of lymphedema that typically presents in infancy and usually involves all four limbs.10,11 Interestingly, germline mutations in patients with isolated arm involvement have not been identified,14,17 and no case of familial transmission has been reported. None of the patients in our cohort had a family history of arm lymphedema.
Although mutations associated with the etiology of isolated primary upper extremity edema are unknown, the subsequent pathophysiology of the disease is the same as for other types of lymphedema. Subcutaneous adipose tissue develops and the limb enlarges. Patients are at risk for infection and psychosocial morbidity. Because primary upper extremity lymphedema is so rare, we advocate for lymphoscintigraphy to confirm the disease. One-fourth of patients referred to a lymphedema center with “lymphedema” have another condition and many other diseases can cause an overgrown arm.22,23 Lymphoscintigraphy is 96% sensitive and 100% sensitive for lymphedema. 15 A patient with a high suspicion of arm lymphedema who has a normal lymphoscintigram should have the test repeated 1 year later because a latency period can exist until the study shows abnormalities. 15 If an adult presents with upper extremity swelling and confirmed as lymphedema by lymphoscintigraphy, we also will image the axilla with CT or MRI to ensure the patient does not have a mass causing secondary lymphedema.
Primary arm lymphedema is managed similarly to other types of lymphedema. Individuals are treated with compression therapies and are encouraged to maintain a normal body mass index and to be active.19,23,24 Patients who fail conservative therapies are candidates for operative intervention. We prefer liposuction to remove the overgrown subcutaneous adipose, which also might improve their lymphatic function.25–28 Individuals with primary lymphedema generally are less amenable to physiologic procedures (e.g., lymphatic–venous anastomosis and vascularized lymph node transfer) because they have aplastic or hypoplastic lymphatic vessels. They are also at higher risk for donor site lymphedema if undergoing a vascularized lymph node transfer because individuals often have systemic lymphatic abnormalities. Patients with suspected primary arm lymphedema should be referred to specialists focused on this disease.
Footnotes
Author Disclosure Statement
No competing financial interests exist.