
Abstract
Abstract
Background:
The aim of this prospective clinical study was to compare the long-term efficacy of complex decongestive therapy (CDT) in obese and nonobese patients with breast cancer-related lymphedema (BCRL).
Materials and Methods:
A total of 59 patients (29 obese patients group 1, 30 normoweight overweight patients group 2) with unilateral BCRL were enrolled. All patients underwent CDT that included manual lymphatic drainage, intermittent pneumatic compression pump, multilayer compression bandaging, lymphedema exercises, and skin care. The CDT was performed for 1 hour a day, 5 days a week for 3 weeks. Patients were assessed according to limb volume difference before CDT, after CDT, and after 1 year.
Results:
The initial lymphedema volume of group 1 was 866.34 ± 389.34 mL and that of group 2 was 661.84 ± 470.6 mL (p = 0.031). The lymphedema severity percentage of excess volume (PEV) of group 1 was 33.37 ± 15.71 and that of group 2 was 31.86 ± 19.63, which was moderate lymphedema. After 15 sessions of CDT program, in group 1, lymphedema volume decreased to 771.46 ± 389.14 mL (post-CDT p = 0.013) and in group 2, lymphedema volume decreased to 468.38 ± 417.36 mL (post-CDT p < 0.0001), and in group 1, PEV decreased to 28.54 ± 16.84 (post-CDT p = 0.002) and that in group 2 decreased to 22.1 ± 16.87 (post-CDT p < 0.0001). After 1 year, group 1 reached the baseline values of the extremity volumes, but in group 2, the volumes of extremities could maintain their post-CDT values.
Conclusion:
Obesity is a factor that deteriorates the CDT efficacy. Early treatment, before developing fat accumulation and fibrosis, must be primary goal in the treatment of BCRL.
Introduction
Lymphedema is defined as persistent tissue accumulation of protein-rich interstitial fluid caused by malformation, dysplasia, or blockage of lymph drainage. 1 Breast cancer-related lymphedema (BCRL) is a common complication of breast cancer treatment. Complex decongestive therapy (CDT), which includes manual lymphatic drainage (MLD) compression therapy, exercise, and skin care, is the current standard treatment for lymphedema.2,3 Several studies have reported the effects of CDT in BCRL.1–4
The cardiovascular system has been a major focus of obesity studies; however, its effects on the lymphatic system remain mostly unknown. 5 Brorson et al. showed that both excess fat and muscle volume contributed to the excess volume in nonpitting arm lymphedema, which was evaluated with dual energy X-ray absorptiometry. 6 In longstanding nonpitting arm lymphedema, most of the increased soft tissue in the affected arm was due to increased fat. Because of the adipose–lymphatic link, liposuction can be an effective treatment in lymphedema patients.7,8
Lymphedema may be a form of regional obesity or lipodystrophy of the affected extremity. 9 Although conservative treatment can be used to reduce swelling, treatment often fails, possibly due to chronic edema being transformed from lymph fluid to subcutaneous fat. 6 Adipose deposition in late-stage lymphedema decreases the potential for response to mechanical treatments (CDT) and can be associated with severe infections, functional disability, skin changes, psychosocial morbidity, and malignant transformation. 9
It is well known that obesity can increase the risk of BCRL.9,10 In a prospective study, it is shown that patients with BCRL with a body mass index (BMI) >30 kg/m2 had three times the risk of developing upper extremity lymphedema compared with those with a BMI <25 kg/m 2 . 11 In another study, it was shown that patients who had undergone breast cancer surgery and developed lymphedema had a higher baseline and current BMI values compared with those who had not. 12 A randomized clinical study showed significant reduction in upper extremity lymphedema in patients who lost weight by dieting for 12 weeks. 13
In clinical practice, noticeable differences are seen in patient response to the CDT treatment of BCRL. 2 There is a popular belief that CDT efficacy is low in obese patients and healthy diet for normalizing BMI is the essential part of the lymphedema treatment. 14 But there is no prospective long-term follow-up study to investigate the effectiveness of CDT in obese patients.
Considering the links between obesity and lymphedema, we aimed in this prospective clinical study to compare the long-term efficacy of CDT in obese and nonobese patients with BCRL.
Materials and Methods
All patients were recruited in a single center dedicated to the treatment of lymphedema between 2012 and 2016. Thirty-three obese (BMI ≥30 kg/m2) and 28 overweight and normoweight (BMI <30 kg/m2), totally 61 patients with unilateral BCRL, were enrolled in the study and all were hospitalized. All patients had undergone modified radical mastectomy (MRM). All patients signed written informed consents and ethical approval was obtained from the local ethic committee.
Inclusion criteria were patients having unilateral lymphedema after their breast cancer surgery, >2 cm difference at the circumference of the measurements or >10% difference in volume between the two arms. Patients who had primary lymphedema, bilateral lymphedema, continuing radiotherapy and/or chemotherapy, active infection, arterial or venous disease, active rheumatic disease such as systemic lupus erythematosus, ulcers in the affected arm, congestive heart failure and uncontrolled hypertension, and those using any medications that affect the body fluid and electrolyte balance were excluded from the study. Patients who had undergone CDT or other interventions for lymphedema within 12 months were also excluded.
During the lymphedema treatment, one obese patient was diagnosed with recurrence of breast cancer, three obese patients were diagnosed with active infection, and two normoweight patients could not be followed up because of the social problems. Therefore, six patients were excluded from the analysis. As a result, a total of 55 patients were included in the final analysis (Fig. 1).
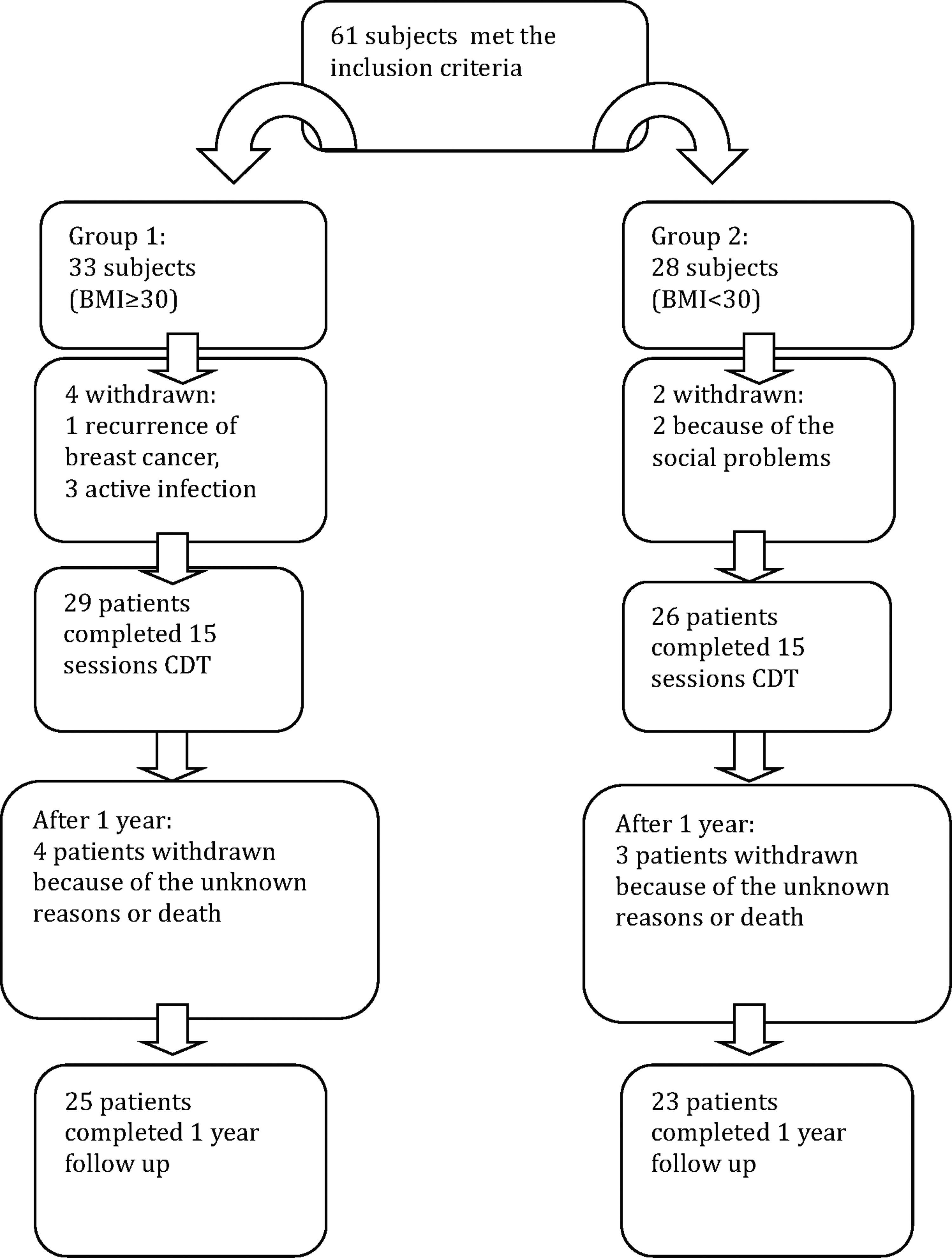
Flow diagram of the patients.
The demographic features of the patients, including age, duration of lymphedema, and number of chemotherapy and radiotherapy sessions, were recorded. The International Society of Lymphology staging was used for determining the lymphedema stage 15 (stage 1: mild edema that is reversible with appropriate limb position, may pit; stage 2: moderate edema that is not reversible with limb elevation. Pitting is present except in late stage 2 when more fibrosis occurs; stage 3: lymphostatic elephantiasis with trophic skin changes).
Truncated cone method was used to calculate estimated volumes for upper arm and forearm. Right and left arm circumferences were measured at 4-cm intervals, starting from the carpometacarpal joint. The volume of each limb was calculated from the circumference using the truncated cone formula. The reliability and specificity of the calculated volume have been established. 16
The severity of lymphedema is defined as percentage of excess volume (PEV), the excess volume (the difference between the arm with lymphedema (VL) and the healthy arm (VH) relative to the healthy arm volume (VH), PEV = [(VL−VH)/VH] × 100%. The PEV is better for defining the severity of lymphedema than the absolute difference volume. This method minimizes the effects of BMI on the calculation of lymphedema severity. 1 The efficacy of CDT, the response to the therapeutic intervention, was quantified as the percentage reduction of excess volume (PREV), formulated as PREV = 100% × [(baseline VL−post-treatment VL)/excess volume]. If PREV was 100%, the volume of lymphedema arm was successfully reduced to the level of the healthy arm. 1
All patients underwent CDT that included MLD, compression therapy with a short stretch bandage for 23 hours per day, intermittent pneumatic compression (Pressomed 2900; Medical Italia, EME physio, Italy) with 30–50 mmHg pressure, multilayer compression bandaging using Rosidal
All measurements were done before CDT, end of the 15 treatment sessions, and after 1 year. All circumferential measurements were done by the same examiner.
Statistical analysis
Statistical analysis was performed using SPSS version 15.0 for Windows (SPSS, Inc., Chicago, IL). Descriptive analyses were used for the demographic data, Spearman's rank correlation coefficient for finding the relationship between variables. The categorical variables were analyzed by independent T-test and Mann–Whitney U test. The Wilcoxon test was used to evaluate the values before and after the treatment within the group. A chi-square test was used to compare the proportion of patients between groups who had a >50% reduction in PREV values. The level of statistical significance was set at p < 0.05.
Results
The baseline characteristics of the 55 patients (29 obese patients, group 1; 26 normoweight–overweight patients, group 2) are shown in Table 1. All patients underwent MRM and axillary lymph node dissection (ALND). There were no differences regarding cancer type, radiotherapy, chemotherapy, physical activity levels, lymphedema stage, and duration in patient groups (p > 0.05) (Table 1).
Baseline Demographics and Clinical Characteristics
BMI, body mass index.
The initial lymphedema volume of group 1 was 866.34 ± 389.34 mL and that of group 2 was 661.84 ± 470.6 mL (p = 0.031). The lymphedema severity PEV of group 1 was 33.37 ± 15.71 and that of group 2 was 31.86 ± 19.63, which was moderate lymphedema based on the ISL definition (International Society of Lymphology, 2013) (p = 0.418). The baseline PEV was not associated with BMI, age, lymphedema duration, radiotherapy, or chemotherapy in two groups (p > 0.05).
On analysis on an intention-to-treat basis, after 15 sessions of CDT program, in group 1, lymphedema volume decreased to 771.46 ± 389.14 mL (post-CDT p = 0.013), and in group 2, lymphedema volume decreased to 468.38 ± 417.36 mL (post-CDT p < 0.0001), and in group 1, PEV decreased to 28.54 ± 16.84 (post-CDT p = 0.002), and in group 2, PEV decreased to 22.1 ± 16.87 (post-CDT p < 0.0001).
After 1 year of CDT treatment, four patients in group 1 and three patients in group 2 dropped out because of unknown reasons or death (Fig. 1). After 1 year, group 1 reached the baseline values of the extremity volumes, but in group 2, the extremities maintained their post-CDT volumes (Table 2).
Volumes of Extremities and Lymphedema Stages of Groups 1 and 2 at Baseline, Postcomplex Decongestive Therapy and After 1 Year
CDT, complex decongestive therapy; EV, excess volume; PEV, percentage of EV; PREV, percentage reduction of excess volume.
The CDT efficacy or PREV was 18.43 ± 44.9 in the obese group and 38.4 ± 47.21 in the nonobese group after CDT (post-CDT p = 0.019). It means that CDT effectively decreased the extremity volumes of nonobese patients, but in obese patients CDT was not effective as much as in the nonobese group. After 1 year, mean PREV in the nonobese group (13.84 ± 51.83) was higher than in the obese group (3.32 ± 51.83), but it did not reach statistically significant level (after 1 year p = 0.736) (Table 3).
Percentage Reduction Of Excess Volume Values of the Patients
Correlation analysis revealed that the baseline PEV values correlated negatively with post-CDT PREV values (r = −0.363, p = 0.006), but after 1 year, PREV values did not correlate with baseline or post-CDT PEV or BMI values.
Discussion
Our findings showed that CDT is effective treatment in obese and nonobese patients with BCRL. But CDT efficacy is lower in obese patients than in nonobese patients. After 1 year, obese group reached the baseline values of the extremity volumes, but in the nonobese group, the extremities could maintain their post-CDT volumes. The baseline excess volume was found to be more related with the less treatment efficacy, but after 1 year, we did not find any relationships between treatment efficacy and excess volumes or BMI.
The mean reduction of lymphedema volume after CDT ranged usually from 20% to 73%, but clinical response to CDT is difficult to predict and factors influencing the response to treatment are relatively unknown. 3 According to Liao et al., baseline lymphedema severity was the most important predictive factor for CDT efficacy. 1 Because of this finding, we included patient groups with relatively equal lymphedema severity. The mean lymphedema severity PEV of groups was moderate based on the ISL definition. According to Eyigör et al., there were negative correlations between post-treatment arm volume and physical activity level, postoperative duration, and postoperative weight gain. 2 In our study, there was no significant difference between two groups with respect to physical activity levels and lymphedema durations. So, these variables could not affect our results. In another retrospective CDT efficacy study, Vignes et al. found that duration of lymphedema from cancer treatment and BMI were the only two predictors of absolute reduction of lymphedema volume after intensive decongestive physiotherapy. 4 In this study, we showed that BMI affected the CDT results and treatment response. So, we thought that BMI is one of the strongest factors affecting the CDT efficacy in both short and long terms after CDT.
Possible explanations for the influence of obesity on health include 9 the stress placed upon the body, particularly the circulatory systems, by the actual physical increase in fat body mass and 10 the increase of endocrine-like functions (increased secretory peptides, etc.) of adipose tissue as they enlarge. 18 Obesity may reduce lymphatic function by either overwhelming normally functioning lymphatic vessels with increased lymph production and/or impairing the function of lymphatic vessels. An obese limb may compress lymphatic vessels or adipose tissue may cause inflammation which leads to damage in lymphatic vasculature. The size of the obese extremity increases, the elevated production of lymph may overwhelm the capacity of the lymphatic vessels to transport the fluid proximally. 19 So, this limited lymphatic capacity may be exacerbated after ALND and CDT may be inadequate in the obese group than in nonobese patients.
Arngrim et al. studied the subcutaneous adipose tissue lymphatic drainage of macromolecules in obese subjects. They found significantly impaired tissue clearance in obese patients. 20 Impaired lymphatic drainage of macromolecules in obese patients may lead to weak CDT response after axillary dissection. Weitman et al. showed that high-fat diet resulted obesity in wild mice has significantly decreased lymphatic transport in lymphoscintigraphy, and abnormal macroanatomy and microanatomy of lymph node and decreased lymph node uptake of interstitial fluid. 5 In light of these findings, we thought that our obese patients may have limited lymphatic capacity before breast cancer treatment and CDT could not work as much as in nonobese patients.
Obesity has effects on skin barrier function, collagen function, wound healing, microcirculation, and macrocirculation. 21 These factors may explain the increased tendency to develop cellulitis in obese patients. 22 Previous cellulitis may lead to lymphatic damage in obese patients. 23 We did not evaluate the cellulitis history of our patients. This may be a limitation of our study.
Long-term lymphatic volume overload induces chronic inflammation, progressive fibrosis, impaired homeostasis and remodeling of adipose tissue, impaired immunologic function, and regenerative capacity. Because these pathological changes are progressive and irreversible, treatment in the early stages of lymphedema is necessary for success of the treatment. 24 The lymphedema stages of our patient group were nearly equal. So, we concluded that the inadequate CDT efficacy in our obese patients was mostly due to high BMI.
Chronic lymph node stimulation has also been shown to result in the expansion of adipose tissue in a rat model. 25 These data link inflammation with adipose tissue metabolism and may help to explain the changes in adipose tissue biology that accompany chronic human inflammatory disorders, such as HIV-associated adipose redistribution syndrome, Crohn's disease, and obesity. 26 Furthermore, in the mouse, heterozygous functional Prox1 inactivation provokes abnormal adipose accumulation. In the affected animals, the presence of obesity is associated with abnormal lymph leakage from mispatterned and ruptured lymphatic vessels. It is hypothesized that the lymphatic vascular defects can cause adult onset obesity.8,25 So, our obese patients might have lymphatic vascular defects and this might lead to their obesity and worsen after axillary dissection in their arms.
Obesity causes a variety of cardiovascular diseases, the most common of which is hypertension, as well as microangiopathies. 27 It is known that obesity was associated with chronic venous insufficiency (CVI) and lymphedema.20,28 In addition, microangiopathy in lymphatic capillaries was shown in CVI patients. 29 BMI was also associated with skin microcirculatory dysfunction. 30 We thought that the underlying microangiopathies become more complicated after lymph node dissections, which reduces the success of CDT in obese patients with BCRL.
Another limitation of our study is that we did not have any secondary outcome measures such as functional measurement, subjective sensations, or quality of life. We evaluated only volumetric changes in arm as a primary outcome. In contrast, long-term follow-up and prospective design are the major strengths of our study.
The effect of climate on CDT outcomes should not be ignored. In our region, where our hospital is situated, summer months tend to be quite hot and patients are not tended to wear compression sleeves from July through September. In addition, adherence to compression garments was not good because of low-income levels of our patients. So, after CDT treatment, maintenance effective compression therapy with compression sleeve was very difficult especially in our obese patient group because of the large extremities and the climate conditions.
In conclusion, obesity is a factor that deteriorates the CDT efficacy. Early treatment, before developing fat accumulation and fibrosis, must be the primary goal in the treatment of BCRL. Weight reduction and encouragement of physical activity immediately after breast cancer treatment must be major treatment approaches in breast cancer survivors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.