
Abstract
Abstract
Background:
Bioimpedance spectroscopy (BIS) is commonly used in the assessment and monitoring of lymphedema. This study investigated electrodes as a source of variability that could impact the accuracy of BIS in the clinic and determined if Ag/AgCl electrocardiograph (ECG) electrodes could be used as an alternative to instrument-specific electrodes.
Methods and Results:
Two types of Ag/AgCl electrodes were studied: instrument-specific bioimpedance electrodes (
Conclusion:
Calculation of interlimb BIS ratios improves accuracy of clinical BIS. Ag/AgCl
Background
Bioimpedance spectroscopy (BIS) is a measurement technique that is growing in popularity for the detection and monitoring of lymphedema. It is used in both research1–4 and clinical practice5,6 to quantify tissue extracellular fluid (ECF). BIS passes a small alternating electrical current, from electrodes placed on the skin's surface, through the tissues in the body or a body region of interest, to determine the resistance or opposition to flow of the current through the ECF. 7 ECF volume is inversely related to resistance8,9 and as lymph is a major component of ECF, BIS is particularly well suited for detection of overall changes in volumes of lymphatic fluid.7,8
BIS assessment for lymphedema uses a tetrapolar electrode arrangement in which the voltage measurement and drive electrodes are separated, thereby minimizing skin contact resistance errors.10,11 The two measurement electrodes define the BIS measurement region to be quantified and the two distally located drive electrodes span the two measurement electrodes. The current is passed between two drive electrodes and the resistance at zero frequency (R0) is derived according to the Cole Model for the region defined by the measurement electrodes. 12 R0 represents the resistance of ECF, including lymph. Accurate placement of the measurement electrodes is critical as small placement errors can affect the measurement as resistance varies proportionately to interelectrode distance.13,14 Furthermore, a minimum distance between the measurement and drive electrodes has been suggested to reduce interference between electrodes. There is little research confirming an optimal or minimal distance for measurement and drive electrode spacing, although 5 cm has been suggested.6,13 While a 5 cm spacing is readily achievable when measuring whole limbs, it may be difficult or impossible to achieve this spacing when measuring short limb segments such as the hand 15 or when performing resistance measurements in babies or infants. 16 It is unclear what effect a smaller or greater distance between the drive and measurement electrode may have on measurement outcomes. While it is unknown if it is essential to standardize electrode placement and the spacing between the drive and measurement electrodes, some manufacturers have introduced electrodes that preset the separation distance (dual-tab electrodes).
The intrinsic electrical characteristics of the electrodes are an additional potential source of measurement variability. To mitigate this variability, some manufacturers of impedance analyzers may specify particular electrodes of a certain size and type for use with their instruments. Typical impedance electrodes for lymphedema assessment are Ag/AgCl gel electrodes and are similar to those commonly used for electrocardiograph (ECG) measurements, and in many situations, ECG electrodes are frequently used for impedance measurements. A wide range of electrode types are commercially available, which potentially adds further variability to resistance measurements. Nescolarde et al. 17 found significant variation in bioelectrical impedance vectors when using different electrode types to measure whole body resistance in 35 healthy subjects. It is unknown if this same variation is found measuring body segments such as what occurs in lymphedema. Other potential sources of variation are electrode age and size. Electrode gel is susceptible to changes in hydration over time and this may affect its electrical characteristics. A wide range of electrode sizes are available and in an attempt to provide sufficient space between electrodes 15 or to reduce costs, electrodes are sometimes cut in half. It is unknown whether electrode age and size affect resistance measurement in humans. It is therefore important to understand and quantify the impact of these potential sources of error in the clinical environment.
The aims of this technical report were therefore as follows:
to explore factors related to electrodes that could impact impedance measurement in the clinical environment, and to determine whether ECG electrodes could be used as an alternative to instrument-specific impedance electrodes in the measurement of unilateral lymphedema.
Materials and Methods
Participants were a sample of convenience from staff and clients associated with a lymphedema clinic in rural New South Wales, Australia. Any person who was pregnant or had cardiac (pacemaker or defibrillator) or metal implants in any limb was excluded from the study. Participants attended one or more measurement sessions of ∼10-minute duration. Ethics approval was obtained from the Human Research Ethics Committee of the University of Sydney (Project No. 2016/450). All participants provided written informed consent.
Equipment
Two different devices were used to address the aims of this study. A single low-frequency (10 kHz) 18 tetrapolar bioimpedance device (XCA ImpediMed Imp™) was used to investigate the resistance characteristics of the electrodes themselves. For the studies on human participants, a single-channel, tetrapolar BIS device that scans between 4 and 1000 kHz 19 (SFB7 ImpediMed Imp™) was used. Human BIS files were processed using the Bioimp software (vs 5.2.4.0) from which the resistance at zero frequency (R0) was derived. R0 was used as the variable for electrode comparisons since it is the variable used in the BIS assessment of lymphedema. Resistance is the opposition to current flow in the body conductors (the fluids), while reactance is the opposition to current flow due to the body's tissues acting as capacitors. Impedance is the total opposition to current flow through the body that includes both resistance and reactance. 7 As resistance and impedance values are identical at zero frequency, both terms can be used interchangeably in human studies, in which R0 is the parameter of interest; however, in this study, the term resistance has been used to reduce confusion. Integrity of the BIS hardware was assessed daily using the test cell supplied by the manufacturer.
Two types of electrodes were used: single-tab electrodes distributed specifically for bioimpedance measurements (
Protocol
Participant height, to the nearest 0.5 cm, and weight, to the nearest 0.1 kg, were measured to allow the calculation of body mass index (kg/m2). Resistance of participant limbs was measured using the principle of equipotentials. 13 Participants were positioned in supine for between 3 and 10 minutes, with the arms and legs extended for the assessment. Electrode placement sites were cleansed with an alcohol wipe and then marked with indelible ink to reduce positioning variability introduced by test–retest design. Sites marked for electrode placement on the hand were as follows: the base of the nail on the third finger 15 ; metacarpalphalangeal (MCP) joint of the third finger 7 ; mid-wrist in line with the ulnar styloid 13 ; and 46 mm distal from the mid-wrist position to replicate dual-tab electrode positions (Fig. 1). Electrode sites on the foot included the following: the base of the second and third toe 20 ; between the malleolus13,20; 46 mm distal from the malleolus position to replicate dual-tab electrode positions; and midway between the 46 mm and base of the second and third toe positions (to replicate the MCP position on the hand) (Fig. 2). Electrodes were centered over these sites.
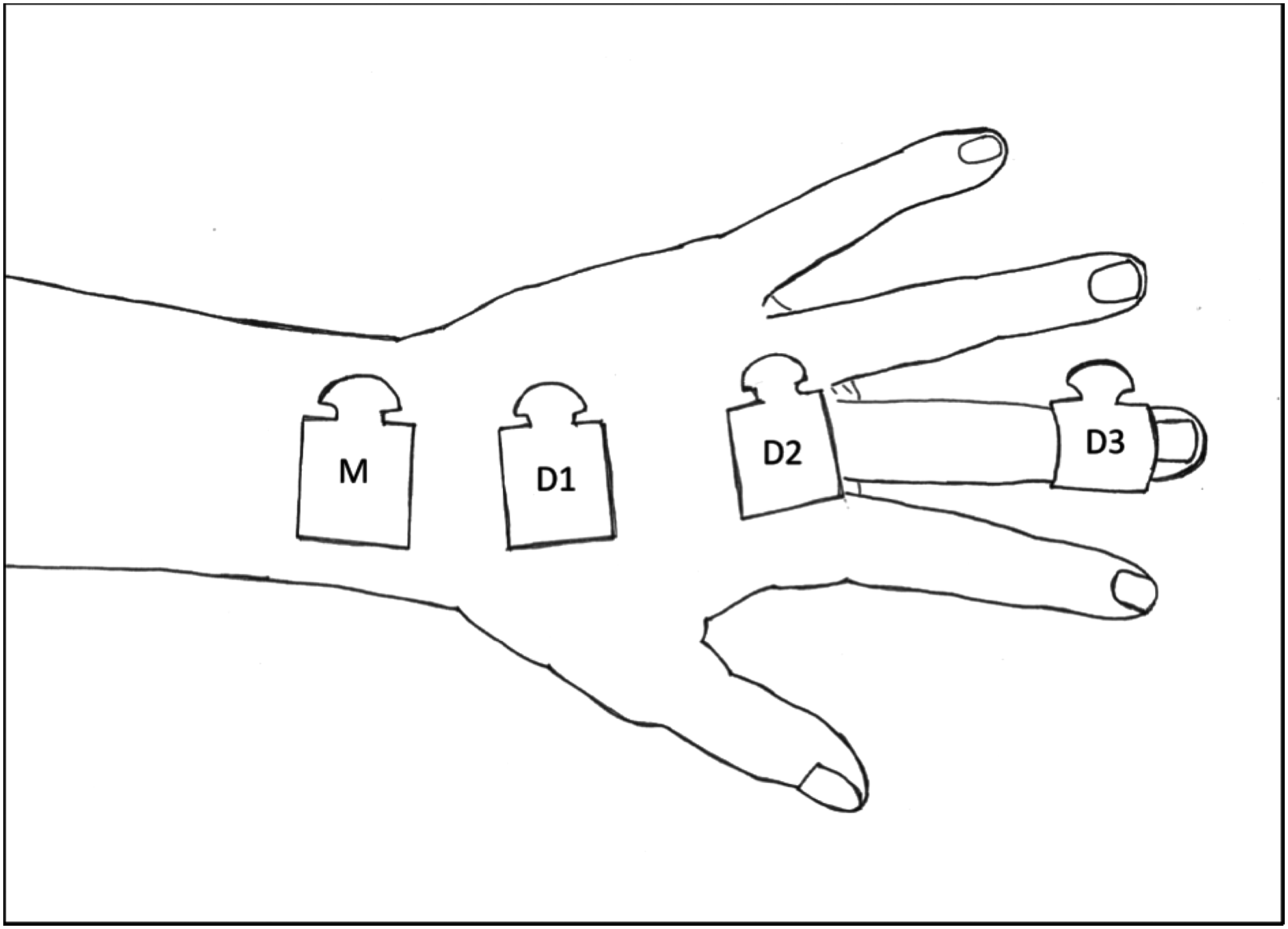
Position of drive electrodes on the hand. Electrodes labeled as follows: measurement electrode placed over ulnar styloid (M), drive electrode at 46 mm from ulnar styloid (D1), drive electrode over MCP at base of third finger, the currently used standard electrode position (D2), and drive electrode at base of nail of the third finger (D3). MCP, metacarpalphalangeal.
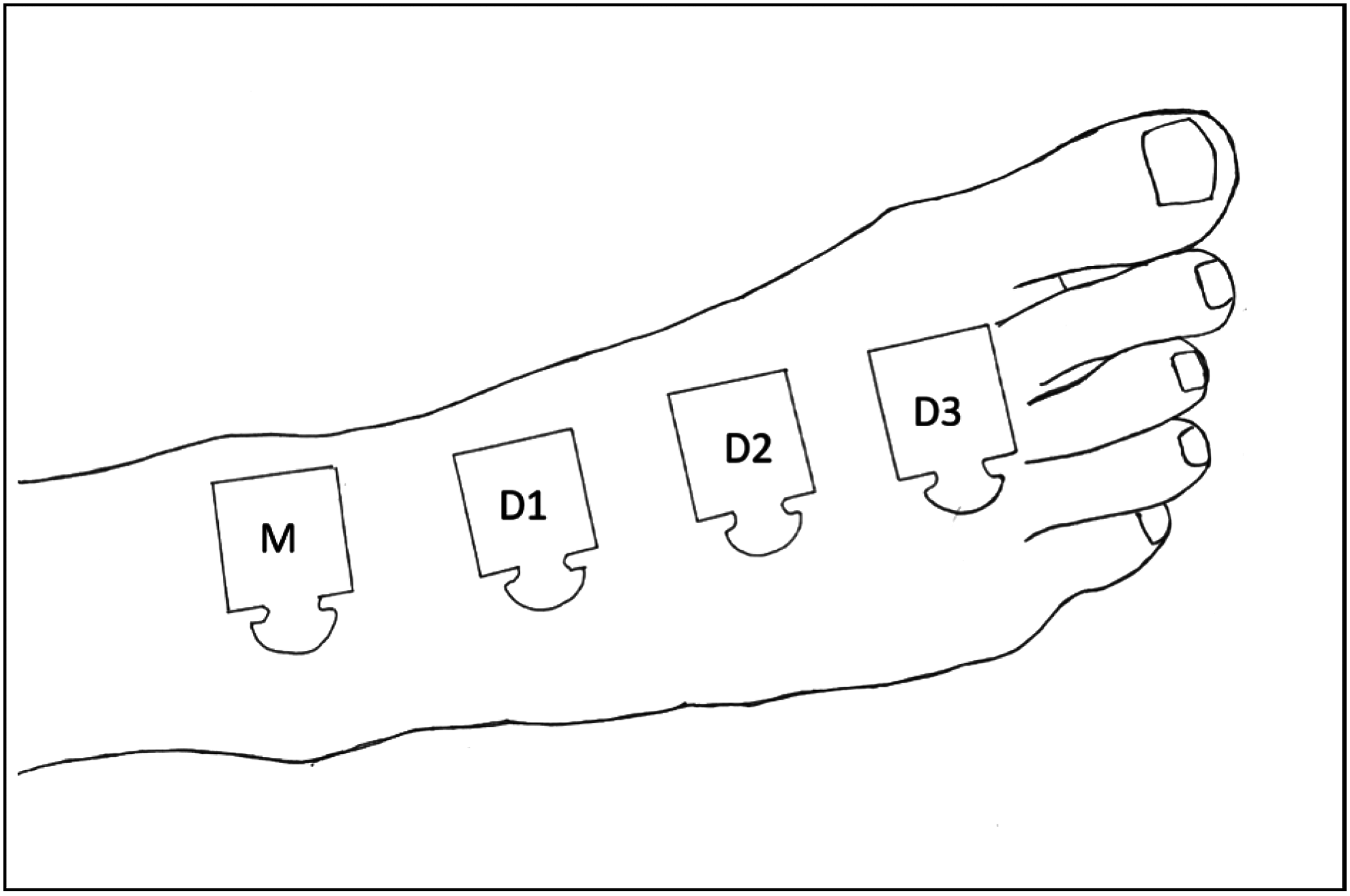
Position of drive electrodes on the foot. Electrodes labeled as follows: measurement electrode placed between malleoli (M), drive electrode at 46 mm from malleolus (D1), drive electrode midway between D1 and D2 to replicate MCP on hand (D2), and drive electrode at base of the second and third toe, the currently used standard electrode position (D3).
Six studies were undertaken, investigating effects of the following: (i) intrinsic electrode resistance; (ii) electrode age; (iii) drive electrode position in relation to the measurement electrode; (iv) electrode width/surface area; (v) concordance between resistance measured by
Participants included persons with and without lymphedema to provide a range of resistance values and were from a population of convenience. Participant characteristics for each of the six studies are shown in Table 1. In total, 34 participants, including 26 women, 3 of whom presented with upper limb lymphedema secondary to treatment for cancer, as well as 8 men, 1 of whom presented with lymphedema of the upper limb secondary to cancer, were included in this study. Of the participants without lymphedema, 12 persons participated in multiple studies. None of the participants without lymphedema (n = 30) exceeded the whole arm BIS ratio thresholds (3SD) for lymphedema as determined by Cornish et al. 5 In contrast, all participants with arm lymphedema exceeded these thresholds.
Participant Characteristics from All Studies
BMI, body mass index (kg/m2).
NA, not applicable, nonhuman study.
Studies
Determination of intrinsic electrode resistance
Electrodes from four different production batches of both the

Two electrodes were sandwiched together to form a test unit. Drive (D) and measurement (M) leads were attached to each electrode test unit and two resistance measurements taken of each unit. Three electrode test units from each batch were used to determine intrinsic electrode resistance.
Effect of electrode age on measurements of limb resistance
Two different production batches of
Effect of drive electrode position on limb resistance
Electrodes from a single current production batch of
Five female participants without a history of lymphedema (Table 1) underwent resistance measures of their right arm and leg using the 3 different drive electrode positions on 2 occasions, ∼1 month apart, providing measurements from 20 limbs. The order of measurements taken was proximal to distal on the first occasion and then distal to proximal on the second occasion to reduce the biological impact of lying in supine.21,22 The women were invited back for a second occasion to confirm that order of the measurements did not impact the resistance measures.
Three men and three women without history of lymphedema underwent resistance measurements of both arms and legs using the three different drive electrode positions to determine the effect of drive electrode position on interlimb BIS ratios. The order of the measurements was alternated to reduce the impact of lying in supine.21,22 These men and women also participated in study F (Table 1).
Effect of electrode width and surface contact area on limb resistance
The resistances of the arms and legs of five participants without lymphedema (Table 1) were measured with three electrodes of different widths:
Comparison of the limb resistance measured by bioimpedance and
cardiac
electrodes
Concordance between
Effect of mixing electrode batches and types on interlimb BIS ratios
Three men and three women without history of lymphedema underwent resistance measurements of both arms and legs using three combinations of electrode batches and types to determine effect of mismatched electrodes on interlimb BIS ratios (Table 1). Participant limb resistance was measured three times: once with electrodes from a single batch of
Data analysis
Resistance and reactance provided by the XCA device were used for comparison of electrode characteristics. For the BIS measurements in human participants, limb resistances, extrapolated from measured data to zero frequency (R0) according to the Cole model,
12
were used. In accordance with measurement protocols for unilateral lymphedema assessment, interlimb BIS ratios were calculated in those without lymphedema:
and in those with lymphedema (arms affected):
Technical error of measurement (TEM) was used to determine measurement imprecision resulting from intrinsic electrode resistance within electrode batches. Human BIS data were checked for normality using the Shapiro–Wilk test. Where data were normally distributed, a paired t-test determined differences among the data; Wilcoxon matched-pairs signed-rank test or Mann–Whitney was used where distribution was not normal. ANOVA, Kruskal–Wallis, and Friedmans tests were used to determine differences between related measures within measurement sets in each group of participants. Bland–Altman plots were used to evaluate the agreement among the different electrodes and width of electrodes; nonparametric tests were used when there were less than 10 measures, regardless of normality. Lin's concordance correlation coefficient was used to determine the extent to which data were in agreement. Data were analyzed using Prism 7 for Windows (version 7.01) and significance was set at p < 0.05.
Results
Determination of electrode resistance
Three test units from four production batches of both the
Electrode Resistance (Ω) Stratified for Production Batch
Measurements made with the Impedimed XCA at 10 kHz. TEM for resistance was calculated using the data from the two tests completed on each of the three test units in each batch.
TEM, technical error of measurement, values in Ω (% of resistance).
Effect of electrode age on limb resistance
One production batch each of current and expired
Effect of drive electrode position on limb resistance
The three drive electrode positions on the foot provided significantly different limb resistance readings. Similar findings were found with the different drive positions on the hand with one exception: those completed with the drive electrode at the MCP and nail bed of the third finger had a 0.3 Ω nonsignificant difference in mean resistance (Table 3). Limb resistance was highest when using the most proximal drive electrode position and lowest at the most distal position for both the arm and foot (Table 3). Measurement bias caused by drive electrode position ranged from 0.5% to 2.3% in the leg and 0.1% to 0.9% in the arm (Table 3). Changing the position of the drive electrode had a greater effect on resistance in the leg than in the arm (p ≤ 0.001 for all drive electrode positions). Conversion of the raw resistance measures into clinically relevant BIS ratios removed the bias effect of drive electrode position in both arms (p = 0.15) and legs (p = 0.96). Drive electrodes were positioned over the MCP of the third finger and base of second and third toe for the remaining studies.
Comparison of Limb Resistance Determined Using Different Drive Positions on the Hand and Foot
Forty-six millimeter between center of the measurement and drive electrodes to simulate dual-tab electrode spacing.
MCP, metacarpal phalangeal joint.
Effect of electrode width and surface contact area on limb resistance
Full-width
Comparison of Resistance Determined from Different Width Electrodes
Electrode width:
Electrode contact area:
Comparison of the limb resistance measured by bioimpedance and
cardiac
electrodes
The
Comparison of Resistance and Bioimpedance Spectroscopy Ratio Determined from Bioimpedance and Half-Width Cardiac Electrodes from 30 Participants
t-Test.
Wilcoxon.
BIS, bioimpedance spectroscopy.
The resistance data from the
Effect of mixing electrode batches and types on interlimb BIS ratios
The effect of combining electrode batches and electrodes types on an individual participant was assessed by changing the electrodes on one limb to a different batch or type of electrode so that two different types or batches of electrodes were used to determine the interlimb BIS ratios. The use of combinations of electrode types and batches did not significantly affect the interlimb BIS ratio for either arms (p = 0.43) or legs (p = 0.74).
Discussion
The importance of electrode characteristics and placement in resistance measurements has not been widely considered. 17 This study examined a number of factors that could impact bioimpedance measurement, but found only drive electrode position and electrode size made a significant difference on human absolute limb resistance measurements. The magnitude of these differences was small and could be minimized by adopting consistent BIS protocols or calculation of interlimb BIS ratios that are typically used in lymphedema assessment to reduce the impact of weight and body fluid composition changes.
The intrinsic resistance of the
Hypothetically, electrode age could also impact on the accuracy of resistance measures in the clinical environment. However, we found that using electrodes, which were almost 2 years past their expiration date and stored according to manufacturer's instructions did not impact on the accuracy of limb resistance measures. This finding should provide confidence to continue use of appropriately stored electrodes, at least up to twice their “lifetime,” an issue that may be of particular relevance in clinical situations with low rates of resistance measurement, which may prevent electrodes being used before the recommended use-by date.
Measurement error can be introduced if the measurement electrodes is not reliably positioned. For example, a change in position as small as 5 mm in both measurement electrodes (1 cm overall) can produce errors of 2%. 14 We found that the position of the drive electrode, in relation to the measurement electrode, also impacts on limb resistance, with limb resistance decreasing as the drive electrode was moved further away from the measurement electrode. The decrease in resistance could be due to reducing interference between electrodes as the distance between the electrodes increased. The magnitude of displacement of the drive electrode in this study was greater than the displacement of the measurement electrode assessed in previous studies, 14 but still produced differences in the resistance measured of up to 1% in the arm and 2% in the leg when comparing the proximal and distal drive electrode positions. This effect, while small and arguably practically insignificant compared to errors caused by measurement electrode placement, could potentially result in clinically relevant accuracy issues when accumulated with other small errors. To limit the cumulative effect of small errors in electrode placement and improve repeatability, a consistent approach to placement of all electrodes on each limb, for each measurement and over time, is recommended. Alternately, use of dual-tab electrodes that standardize this distance will minimize this error. However, assuming consistent positioning of electrodes within individual BIS measurements, any variation of position of the drive electrodes over time will be mitigated by conversion of absolute resistance measures into the clinically relevant interlimb BIS ratios, thereby contributing to the reliability of BIS for ongoing monitoring of lymphedema.
Electrode width and surface contact area impacted limb resistance. Differences in resistance were identified within (full-width and half-width
Interestingly, and as highlighted above, conversion of absolute limb resistance into clinically relevant interlimb BIS ratios appears to resolve many of the issue that may impact accuracy and reliability of BIS measurements in the lymphedema clinic. Not only does the interlimb BIS ratio account for changes in body composition and weight but also negates the effect of inherent electrodes differences, electrode size, and position of the drive electrode, and allows electrodes from different batches and in this case, different types of electrodes, to be mixed during individual measurements. The utility of the interlimb BIS ratio provides confidence in the accuracy of BIS for monitoring and assessment in the lymphedema clinic.
While there are a number of factors that could impact limb resistance measurements, this study has shown that the factors considered in this study have either no effect on the measurement of human limb resistance or small effects that could be overcome with consistent BIS protocols or conversion of limb resistance measurements into more clinically useful interlimb BIS ratios. Attention to detail at a technical level, and specifically electrode placement, can prevent cumulative bias in results. A consistent and easily followed BIS protocol enables
Conclusion
The interlimb BIS ratio commonly used in lymphedema practice provides a robust measure of limb edema that overcomes potential sources of error in the clinic. Ag/AgCl
Footnotes
Authors' Contributions
B.J.S. contributed to the study conception and design, data collection, analysis and interpretation of data, and article preparation; E.S.D., L.C.W., and S.L.K. contributed to the study conception and design, analysis and interpretation of data, and article preparation.
Author Disclosure Statement
Authors B.J.S., E.S.D., and S.L.K. have no competing financial interests. L.C.W. consults to Impedimed Ltd. Impedimed had no involvement in the design, undertaking, or article preparation of this study.