
Abstract
Abstract
Background:
In a previous randomized controlled trial it has been demonstrated that arm compression sleeves worn immediately after breast cancer surgery, including axillary lymph node removal in addition to physical therapy are able to reduce the occurrence of early postoperative swelling and of arm lymphedema up to 1 year and to improve quality of life. The aim of the present investigation was to check the further development of the arm swelling in patients using compression sleeves or not, and to compare the quality of life in women treated due to breast cancer 2 years after surgery.
Materials and Methods:
Twenty from originally 23 patients who still wore their compression sleeves (15 mmHg) and 21 from 22 patients who had been randomized into the control group without compression could be seen after one more year. Arm volume measurements were performed and quality of life (QLQ-C30 and QLQ-BR23 questionnaires) was assessed.
Results:
Three from 20 patients in the compression group (CG) and 6 from 21 without compression showed arm lymphedema, defined by an increase of the arm volume exceeding 10% compared with the preoperative values. Significant improvement of several quality of life parameters were found in the CG.
Conclusion:
Light compression sleeves worn for 2 years are not only able to reduce the incidence of early postoperative edema and of lymphedema, but also lead to a significant improvement of important quality-of-life parameters like physical functioning, fatigue, pain, arm and breast symptoms, and future perspectives.
Introduction
Breast Cancer-Related Lymphedema (BCRL) remains one of major long-term complications of oncological treatment. Axillary lymph node dissection, sentinel lymph node biopsy, and radiotherapy are associated with the development of BCRL by damage of the distribution or function in the lymphatic system of the axilla.1–4
Breast cancer survivors are also at higher risk of decreasing physical activity (PA) and increasing sedentary behavior after cancer diagnosis. 5 BCRL and low level of PA lead to significant functional, psychological, and social morbidity decreasing health-related quality of life (HRQOL). 6 The majority of studies reported significantly poorer HRQOL outcomes in patients with BCRL resulting in decreased physical functioning and of psychological and social well-being in comparison to breast cancer survivors without BCRL.
There are some studies which have shown that compression combined with exercise regimes is a very effective treatment modality improving physical functioning and general health in patients with BCRL.7,8 This treatment requires lifelong management and the effectiveness depends on patient compliance.
Despite different attempts, scientific evidence concerning prevention of BCRL remains still poor.7,9 Appropriate physical exercises may have beneficial effects, including considerable improvement in range of shoulder motion after surgery,10,11 cardiorespiratory fitness, and quality of life, 12 but prospective randomized controlled trials evaluating especially the long-term effects of postoperative light compression combined with the exercises in women at risk for BCRL starting before surgery are lacking.
Recently, we could demonstrate that class I compression arm sleeves in combination with exercises are able to reduce the incidence of early postoperative arm swelling and of BCRL 1 year after surgery. 13
In that prospective, randomized trial comprising a total of 45 patients, who all were seen before surgery and then underwent surgery of the breast and of axillary lymph nodes, 4 from 23 patients (17%) in the compression group (CG) and 7 from 22 patients who had no compression (31.8%) showed an increase of the arm volume of more than 10% after 1 year. The difference between the two groups was not statistically significant, probably due to the low number of investigated patients. However, the rate of 32% arm lymphedema 1 year after surgery ranges in the upper assortment of reported data in the literature. 13
The aim of the present follow-up study was to detect arm volume changes during one more year, to check the further development of the arm swelling in patients using compression sleeves or not, and to compare the quality of life in women treated due to breast cancer 2 years after surgery.
Materials and Methods
Between 2014 and 2015, 45 women recognized by diagnosis were preoperatively randomly assigned to a CG, or to a control group without compression (No CG [NCG]). The exclusion criteria were: symptoms/signs of infection in the affected limb, signs of heart or renal failure, vein thrombosis, severe pulmonary insufficiency or liver disease, any evidence of active cancer or preoperative lymphedema (≥10% difference in limb volumes), and history of bilateral lymph node dissection. The two groups were comparable concerning baseline characteristics, including BMI, type of surgery, and additional oncotherapeutic modalities.13,14
From 45 patients recruited at the beginning, after 2 years 1 patient from CG died and 3 patients (2 from CG, 1 from NCG) resigned, finally 41 patients have continued prophylactic management, including circular-knit sleeves in class 1 (ccl1, 15–21 mmHg) for daily wearing with physical exercises (CG, n = 20) or physical exercise without compression (NCG, n = 21) in postoperative period. Compression sleeves, delivered by the same factory (MEDI Bayreuth, Germany), were ready made (standard), but fitted based on the individual limb measurements and exchanged every 6 months.
At each time of investigation, the volumes of both (the at risk and contralateral) arms were assessed by measuring the arm circumference and calculating the volume by using a simplified frustum formula. 15 These values were compared with the preoperative arm volumes. To assess the edema volume the so-called excess volume was calculated for each time point by subtracting the arm volume of the affected side from the volume of the contralateral side.
A postoperative increase of the arm volume exceeding 10% compared with the preoperative arm volume, had been defined as lymphedema.16,17
HRQOL was measured with European Organization for Research and Treatment of Cancer (EORTC) QLQ-C30 and QLQ-BR23 questionnaires, 18 in both groups 2 years postoperatively.
The research protocol was in accordance with the Helsinki Declaration, approved by the local ethics committee (No: 63/KBL/OIL/2014).
Statistics
The categorical variable data were presented as proportion and the continuous variables as mean (standard deviation) in normally distributed (according to Shapiro–Wilk test) or median (interquartile range 25%–75%). The associations between continuous or ordinal variables were compared within one group by Wilcoxon rank-sum test (non-normal distribution), comparison between the groups was done by Mann–Whitney U test. Mean of normally distributed variables was compared, and paired t test was used to examine the differences. Correlations among affected arm volumes, edema volumes, BMI, and HRQOL parameters were calculated using Spearman test. A p-value of less than 0.05 was regarded as significant.
Results
From 45 patients recruited at the beginning of this study, after 2 years 1 patient from CG had died and 3 patients (2 from CG, 1 from NCG) resigned, finally 41 women (20 in CG and 21 in NCG) could be checked after 2 years. BMI has not changed markedly through the observation time in both groups, although patients in NCG were constantly more overweight, compared with the CG (p = 0.02). At the end of observation the CG showed significantly lower mean affected arm volume compared with NCG (p = 0.023) (Table 1).
Comparison Between the Groups Initially, After 1 and 2 Years
Pairwise comparison with initial variables within a group using Wilcoxon rank sum test.
Comparison between the groups using Mann–Whitney U-test or ct-test.
IQR, interquartile range (25%–75%); NCG, no compression group; SD, standard deviation.
Arm volume changes compared with preoperative values
As presented in Figure 1 two patients in the CG group continued to show volume differences of more than 10% after one more year and one new case with BCRL occurred (solid lines). Only one patient who developed lymphedema after 1 year wore a class 2 circular-knit sleeve, (ccl2, 23–32 mmHg), whereas the other two patients continued to wear daily sleeves in class 1 and performed physical exercises. The remaining patients without arm swelling also continued wearing sleeves in ccl1.
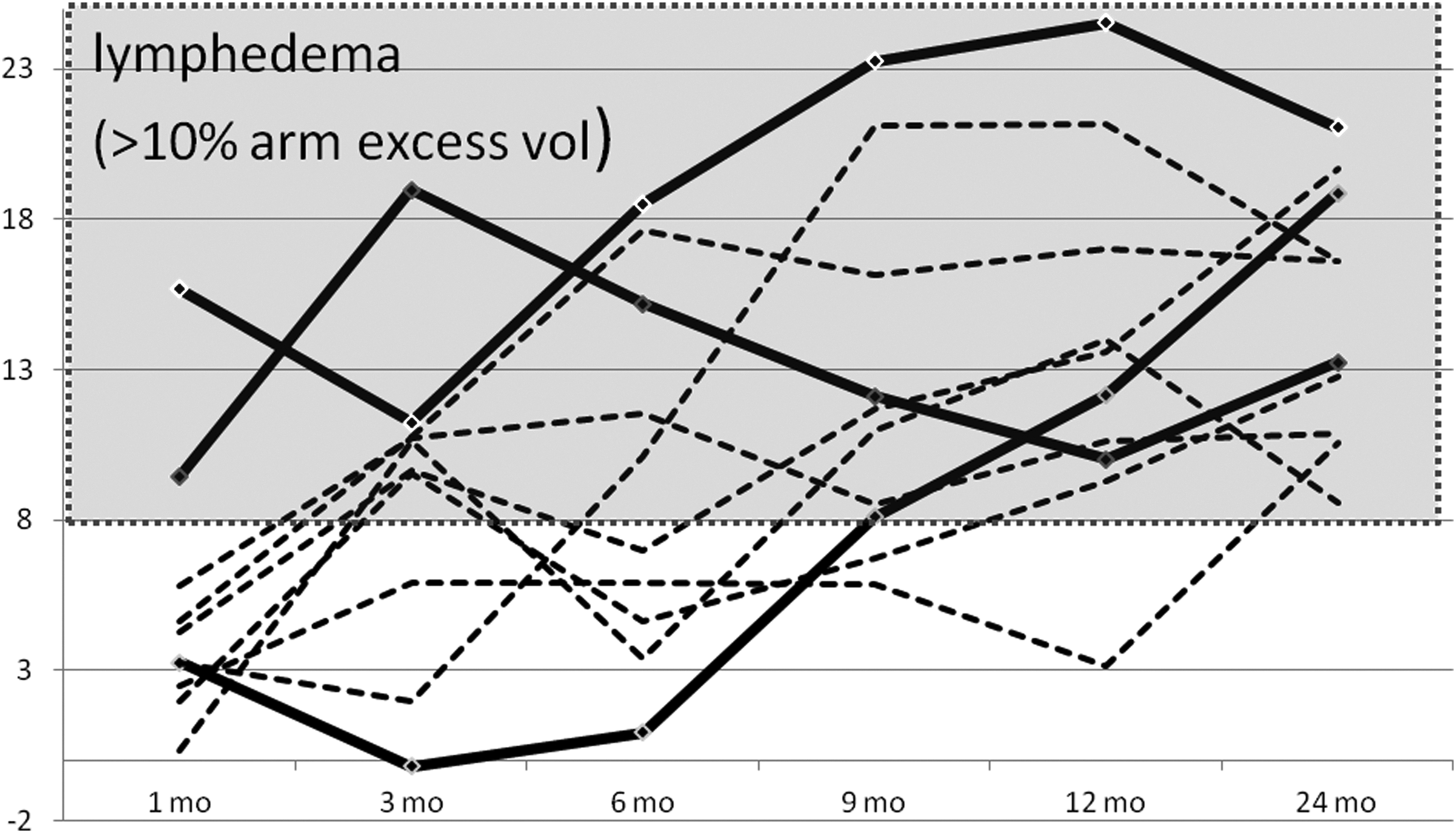
Arm lymphedema (in percentages) within three patients in CG (solid lines) and six patients in NCG group (dotted lines) during 2 years observation. NCG, no compression group.
From the 21 patients in the NCG group who could be followed up to 2 years, 6 patients developed lymphedema after 1 year. After one more year, one additional patient developed an arm volume difference of 10%, whereas another patient showed a value of less than 10%, so that 6 patients out of 21 were diagnosed with BCRL (Fig. 1–dotted lines). Only one patient starting with BCRL already 3 months after surgery was ready to use compression sleeves after 1 year, which in this case led to a reduction of the arm volume after 2 years to a value of 8.6%.
Excess volume changes (“Edema”) compared with contralateral arm
Figure 2 shows the excess volume defined by the difference of the affected arm volume minus the contralateral arm volume in milliliter as a measure of edema at each time point up to 2 years. As can be seen, the average values of edema are in the positive range in NCG, and negative in CG group.
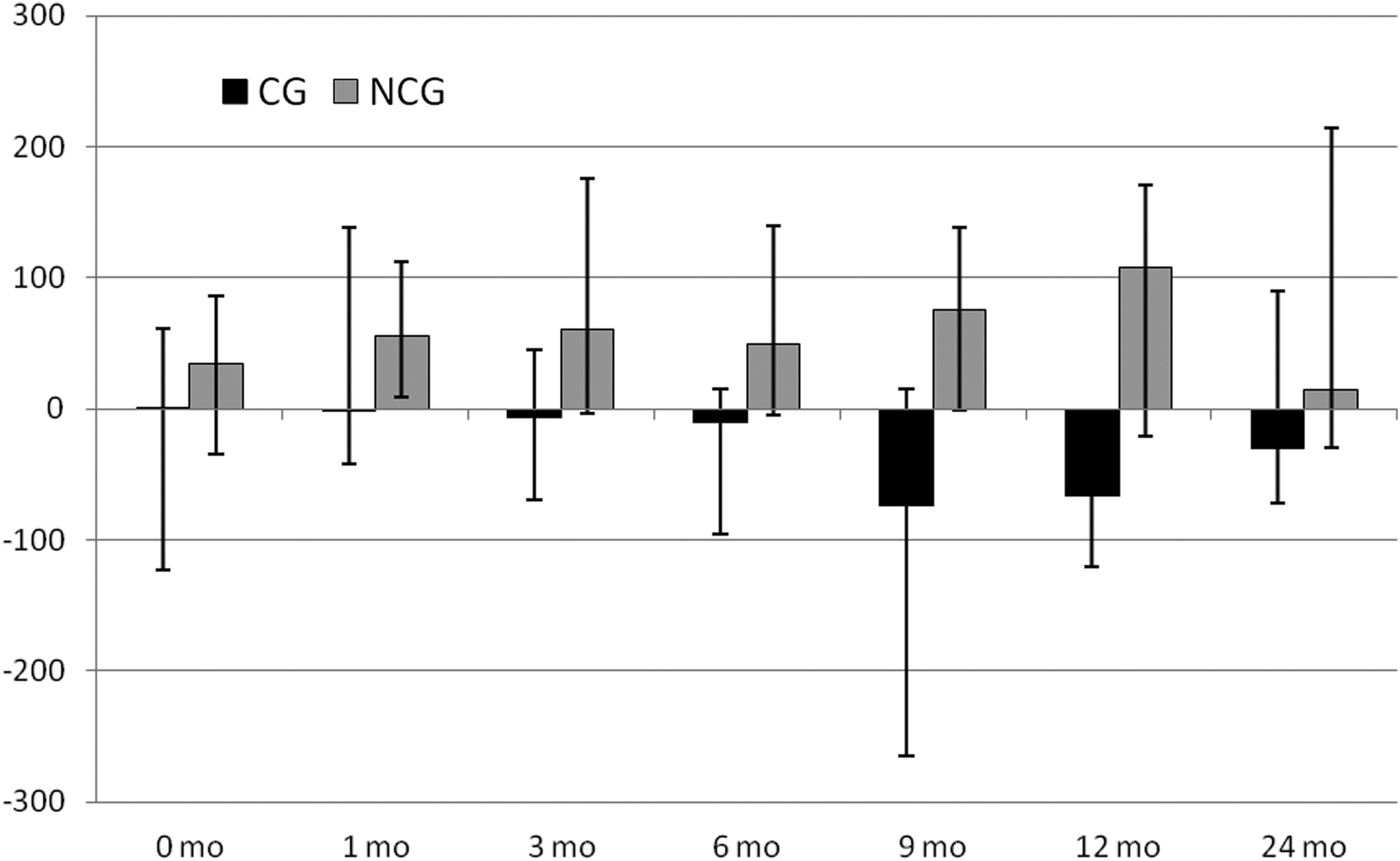
Median (IQR 25%–75%) edema volumes (mL) in CG and NCG groups.
All patients with recognized BCRL after 2 years were advised to wear arm compression sleeves in ccl2 and/or to perform physical therapy, but only one patient who developed new BCRL from NCG during the second year wanted to start with a class 2 sleeve.
Quality of life
The available data indicated significant differences between groups for some assessment points (functional scales and symptom scales) in QLQ-C30 and in QLQ-BR23 (Table 2). Pairwise comparison between the outcomes after 1 and 2 years showed more significant improvements (p-values in bold) in the CG (functioning, fatigue, pain, insomnia, future perspectives) than in the NCG group, which only demonstrated significant improvement of therapy side effects and arm symptoms.
Health-Related Quality Of Life Median Parameters According to EORTC qlq-c30 and EORTC qlq-br23 Within and Between Both Groups
Pairwise comparison with initial variables within a group (Wilcoxon rank sum test).
Comparison between the groups (Mann–Whitney U test).
EORTC, European Organization for Research and Treatment of Cancer.
Comparing the QOL data between the two treatment groups after 2 years, it can be shown that a significant improvement of several parameters was achieved in the CG only (functioning, fatigue, pain, future perspectives, therapy side effects, and breast and arm symptoms) and that wearing arm sleeves for another year was very beneficial, independent from the occurrence of lymphedema. After the first year only significant improvement of physical functioning, and arm symptoms were observed in the CG group.
Discussion
Our study showed that the majority of BCRL developed in the first year. Only two patients in the NCG showed new BCRL after 1 year.
It has been demonstrated that an increase of the arm volume exceeding 10% in comparison to the preoperative value is a reliable indicator of lymphedema. 16 In a prospective study using perometry on 1173 patients a relative volume change (RVC) of ≥5–<10% occurring >3 months after surgery was significantly associated with an increased risk of progression to ≥10% (HR: 2.97). 17 Additional significant risk factors included axillary lymph node dissection (p < 0.0001), and higher BMI at diagnosis (p = 0.0028). 19 Any range of RVC elevation occurring ≤3 months after surgery was significantly associated with increased risk of progression to ≥10%. This point emphasizes the importance of early postoperative arm swelling as a potential precursor of BCRL as this was underlined in our previous publication. 13
Our data also agree with the results of another prospective study performed with a more exact perometer by Stout et al., in which the authors have shown that already a volume increase of >3% after 3–6 months is a predictor of later lymphedema. 20 In our series, we found high degrees of statistical significance comparing the frequency of early onset and late manifestations of edema after 2 years for both groups of patients (Fishers exact test).
Various data were reported concerning the incidence of postoperative BCRL 2 years after oncological treatment. Togawa et al. gave a cumulative estimate of self-reported BCRL of 20% in a total of 666 patients. 19 In a study encompassing 371 patients, Monleon et al. reported a probability of developing BCRL within 12, 24, and 36 months postsurgery of 28.7%, 34.6%, and 38.3%, respectively. More extensive surgery, axillary lymph node dissection, chemotherapy, radiotherapy, and postoperative seroma were predictors of BCRL in the bivariate survival analysis. Only axillary lymph node dissection and radiotherapy maintained their significance in the multivariate model. 1
Our own data showed an incidence of arm lymphedema after 2 years of 3/20 patients wearing compression sleeves for the first 12 months and of 6 from 21 patients who had only physical therapy during the first year. This high incidence of BCRL in the NCG group (31.8%) was observed even though the rate of total lymph node dissection was much higher in the CG group compared with NCG. The relationship between isolated sentinel lymph node dissection versus total dissection was 15:7 in NCG, but 9:14 in the CG group. All patients had X-ray therapy in addition.
In a systematic review of 32 studies Rogan et al. concluded that compression sleeves do not aid in a volume reduction in the acute phase, but they can prevent additional swelling. 7 Our data seem to confirm this concept, especially concerning the occurrence of early swelling in the postoperative phase. When the arm volume exceeded 10% of the initial values, compression sleeves did not reduce arm swelling (Fig. 1–solid lines). However, it needs to be underlined that nearly all patients went on to use the light, prophylactic sleeves only and that they did not get a regular therapy phase with proper compression, which might have reduced persistent edema. Patients with developed BCRL require stronger compression, including multilayer bandaging during the intensive phase of decongestive lymphatic therapy (DLT) 8 as well as compression garments combined with PA in the maintenance phase.21,22 Also a lower HRQOL score is reported compared with those without BCRL due to resulting decrease in physical functioning, and psychological and social well-being. 6 In one cross-sectional study 20% of patients with BCRL had major impact on HRQOL. 23 Chronic BCRL is also associated with high direct and indirect costs. 24
Most previous studies concentrated on the effects of compression in combination with exercises for survivors with developed BCRL. 25 Some data demonstrate positive effects of compression with exercises in the maintenance phase of DLT, 8 whereas others describe neither a positive nor a negative effect regarding BCRL from compression use during exercise.26,27 Some studies question the clinical recommendation that garment must be worn during exercise and recommend an individualized approach.26,27
Early supervised physiotherapy may be effective in preventing BCRL, but the exact contribution of its components is unknown. 28 The prophylactic role of compression in combination with exercise to reduce the incidence of postoperative BCRL is also unclear. Prospective randomized trials evaluating especially the long-term effects of compression, with exercises on symptoms and quality of life in survivors at risk for BCRL, are still limited.
In our recent data we demonstrated that wearing compression sleeves in compression class 1 (15–21 mmHg) in addition to PA was able to reduce the incidence and amount of early postoperative edema and of BCRL. PA levels were essentially equivalent between women wearing and not wearing compression garments, and their HRQOL was not significantly diminished by this intervention. 14 After 2 years of observation in the patients who continued wearing compression sleeves and performed exercises in compression during a day, significantly lower mean affected arm volume was still observed compared with the group without compression (Fig. 2). This is even more important as arm swelling within the first year after breast cancer surgery may be transient, manageable by compression. 29 Similar observation was made in our study. Another article pointed at 2-week postoperative swelling, which may lead to BCRL. 30
There is no doubt that PA plays an important role during and after breast cancer treatment and women who participate in regular PA, may improve their survival, cancer recurrence, and mortality.31,32 All types of exercises (aerobic, resistance, or combined) improve physical fitness and quality of life33–35 in breast cancer survivors, but combined exercises are associated with better outcomes than aerobic or resistance exercises alone. 33 The positive influence on symptoms and quality of life is observed not only in combination with compression and breathing exercises, but also with complementary methods like yoga, which is often recommended as a supportive intervention for reducing fatigue and sleep disturbances and improving mental health. 36
In an effort to reduce the risk of BCRL, patients are commonly advised to avoid heavy lifting and strenuous use of limb-impacting activities of daily living, but this advice lacks evidence. Heavy-load activities among women following surgery do not increase the risk of BCRL. 37 The question concerning type of exercise for preventing BCRL is still open. It is difficult to say if exercises should be performed with or without compression in women at risk. Researchers are still looking for better solutions, especially for primary prevention. In our observation, the increased limb volumes in NCG group of patients suggest an insufficient protective role of PA alone in preventing BCRL. Also in another study a nurse led PA program twice a week for 6 weeks without adjunctive compression was not effective in early prevention of BCRL. 38
Breast cancer survivors often suffer from long-term psychological distress, chronic pain, and fatigue impairing their quality of life. Our data show a surprisingly positive influence of the compression sleeves with low pressure on these subjective symptoms. We found significant differences in quality of life between the groups with and without compression regarding some QOL parameters (functional scales and symptom scales) in QLQ-C30 and in QLQ-BR23 2 years after surgery.
Patients who used compression sleeves in combination with exercises reported higher HRQOL scores compared with the group without compression concerning physical and cognitive functioning as well as future perspective. The QLQ-BR23 data revealed lower fatigue, pain, therapy side effects, and breast and arm symptoms in the group with compression. It had been shown that BCRL is a major risk factor for developing chronic pain (odds ratio 2.58, 95% CI: 1.93–3.46, p < 0.00001). 39 Preventing BCRL may therefore lead to lower pain intensity. In fact our QOL comparison at 2 years showed significantly improved values for fatigue, pain, and breast and arm symptoms in the CG. The main reason for this surprising result seems to be a kind of safer feeling of our patients who are afraid of acquiring arm lymphedema. Due to the low pressure of the sleeves donning was easy, and uncomfortable constriction feeling could be avoided.
Better physical functioning as well as lower breast and arm symptoms can also be related to the exercises performed in compression. Patients might have exercised more in compression due to lack of the fear of developing BCRL. They did not have to refrain from domestic activities of daily living allowing better arm mobility and less shoulder pain. Some authors have discussed such precautionary behaviors in connection with the risk of developing BCRL. 40
Better future perspectives in the CG can lead to an improvement of social well-being. Seventeen of 20 examined women in the group with compression did not have to resign from their work. From an economic point of view, compression as a preventive method seems also cost effective, which should be further evaluated.
One limitation of our study was, besides the small sample size, the differences between the patients' age in both groups. However, age was not seen as a separate risk factor for BCRL in the literature. 41 The lower BMI within the experimental group could also play some protective role in BCRL incidence.
Our observations confirm the long-term benefits of compression garments in combination with adapted PA and during domestic activities. This can be considered as part of a prospective model of surveillance in addition to education, pre and postoperative arm measurements, and interdisciplinary cooperation. Studies in larger patient groups and longer observation periods up to 10 years could reveal more visible protective effects of compression as the cumulative incidence of BCRL may increase from 13.5% in 2 years to 41.1% in 10 years. 42
Conclusion
Compression sleeves in ccl 1 in combination with PA decrease the risk of BCRL and have a positive impact on performance, arm symptoms intensity, and HRQOL 2 years after breast cancer and lymph node surgery.
Footnotes
Acknowledgment
This work was supported by the University of Physical Education, Krakow, Poland, grant number, 51/BS/KRK/2014.
Author Disclosure Statement
No competing financial interests exist.