
Abstract
Abstract
Background:
Yellow nail syndrome (YNS) is a rare disease manifesting as a triad of yellow–green dystrophic nails, lymphedema, and chronic respiratory disease. The etiology of YNS is obscure and investigations are few. A single lymphatic pathogenesis has been proposed to account for all the associated features, and despite the lack of evidence for a unifying lymphatic mechanism, this hypothesis prevails. The objective was to explore the lymphatic phenotype in YNS and to establish whether lymphatic dysfunction could be a major contributing factor to the disease process.
Methods and Results:
Four-limb lymphoscintigraphy was performed on patients with YNS and on healthy, age-matched controls. All 17 patients had lower limb swelling, and 14 (82%) had upper limb swelling also, including 5 (29%) with hand involvement. None of the YNS lymph scans was completely normal. Combined qualitative and quantitative assessment showed that 67% of YNS scans were clearly abnormal compared with 36% of healthy control scans. Mean axillary and ilio-inguinal nodal tracer uptakes were 41%–44% lower in the YNS group than in the controls (p < 0.0001).
Conclusions:
YNS is a lymphatic phenotype because lymphatic insufficiency was found to exist in all patients and the insufficiency was widespread (upper and lower limbs), with a common mechanistic fault of poor transport. The origin of the lymphatic fault is unclear. In healthy individuals, lymphatic abnormalities may be relatively common in the fifth decade of life onward.
Introduction
S
The study's aim was to explore the lymphatic phenotype in YNS and to establish whether lymphatic dysfunction identified by lymphoscintigraphy could be a major contributing factor to the disease process, and not simply a secondary phenomenon. We assessed lymph drainage in the upper and lower limbs of carefully characterized YNS patients relative to an age-matched, healthy volunteer group in a case–control study. A secondary objective was to establish the prevalence of lymphatic abnormalities in healthy, middle-aged to elderly controls for which there are no published data.
Materials and Methods
Participants
Seventeen patients of mean age 64 years (confidence interval [CI]: 59–68 years, range 49–82 years), 7 men and 10 women, with a diagnosis of YNS were recruited from St George's University Hospitals NHS Foundation Trust, London; Cheltenham General Hospital, Cheltenham; Lytham Hospital, Lytham St Anne's, Lancashire; Oxford University Hospitals NHS Foundation Trust, Oxford; Royal Brompton Hospital, London; Royal Derby Hospital, Derby; Royal Hampshire County Hospital, Winchester; Parkside Hospital, Wimbledon, London; University Hospitals Bristol NHS Foundation Trust (Bristol, United Kingdom). Diagnosis of the syndrome was made by the consultant skin or chest physician, but this was confirmed by clinical assessment. Fifteen healthy controls aged 65 years (CI: 58–72 years, range 44–82 years), 7 men and 8 women, were also recruited. The controls were spouses or friends of the patients and had no history of limb swelling, abnormal nails, chronic respiratory disease, or venous disease. The study was approved by the Research Ethics Service of the Health Research Authority of the United Kingdom (reference number 12/LO/1330) and the procedures followed were in accordance with the ethical standards of the responsible committee and with the Declaration of Helsinki. The use of the radiopharmaceutical was approved by the Administration of Radioactive Substances Advisory Committee (ARSAC) (295/3230/29476). All participants gave written informed consent.
Clinical assessment
A detailed history was taken to ascertain the YNS symptoms, when they had first occurred, their duration, whether remission had occurred, what treatments had been given, and whether other conditions such as venous disease could account for the edema. The nails were assessed for slow growth, transverse overcurvature, thickening, onycholysis, dystrophy, color change, and cuticle loss. Figure 1 shows a sequence of nail images from one patient over a 4-year period. The limbs were examined for signs of edema (loss of skin translucency; increased skin and subcutis thickness; pitting edema; smoothing of contours around joints) and the toes were tested for Stemmer's sign.14,15 The clinical findings are shown in Table 1. The controls were similarly assessed to exclude lymphedema and nail abnormalities.

The left hand of a patient with yellow nail syndrome (YNS-011) over a 4-year period. In
Resolution of nail abnormalities was reported. Patients YNS-001, -002, -007, -008 and -012 reported venous disease also. Treatment information not shown.
COPD, chronic obstructive pulmonary disease; L, left; N, no; R, right; Y, yes; YNS, yellow nail syndrome.
Lymphoscintigraphy
Four-limb lymphoscintigraphy was performed according to standard local procedure. 99mTc-Nanocoll (0.2 mL, 25 MBq; GE Healthcare, Little Chalfont, Buckinghamshire, United Kingdom) was injected subcutaneously into the web space between the first and second metacarpophalangeal joints of each hand and between the first and second toes of each foot. Imaging was performed using a single head Argus Epic gamma camera (MIC Ltd., Fleet, Hampshire, United Kingdom; 128 × 128 matrix, low-energy general purpose collimator). Static images (2-minute acquisitions) of the hands and feet were obtained immediately postinjection and at 1 and 2 hours postinjection, and of the axillary and ilio-inguinal lymph nodes at 2 hours postinjection. Dynamic whole body images were obtained at 15 minutes and 2 hours postinjection. Participants were sitting for hand imaging and otherwise supine. No exercise was performed. Two YNS scans and one control scan were of insufficient quality and were excluded. Figure 2 shows whole-body images at 2 hours.

Four-limb lymph scans obtained 2 hours after injection of radiotracer from two patients with YNS and two healthy controls. Left side of image = right side of participant. Patient YNS-003: reduced regional node and lymphatic tract imaging (delay) in all four limbs; right (R) axilla = 0.9%, left (L) axilla = 0.6%, R groin = 2.5%, L groin = 0.9%. This patient was very slim and the upper limbs are positioned at the sides of the body (in the other images they are held across the abdomen). Patient YNS-030: asymmetric nodal uptake (1), limited aplasia (2) and tortuous tracts (3); R axilla = 0%, L axilla = 0%, R groin = 1.7%, L groin = 1.7%. Control YNS-018: tortuous tracts (3) and popliteal nodes (4); R axilla = 5.4%, L axilla = 5.4%, R groin = 15.2%, L groin = 5.6%. Control YNS-028: normal scan; R axilla = 2.1%, L axilla = 1.8%, R groin = 12.1%, L groin = 8.0%.
Quantitative analysis of lymph scans
Regions of interest were drawn around the regional lymph nodes and depots. Lymphatic function was assessed quantitatively as the regional nodal uptake at 2 hours. Nodal uptake was the nodal activity expressed as a percentage of the activity in the hand or foot depot postinjection, corrected for radioactive decay. Reduced lymph transport was assumed if <3% of the injected radioactivity is present in the axillary nodes and <8% in the ilio-inguinal nodes at 2 hours, thresholds obtained from normative patient data and used in lymph scan assessment at St George's Hospital and elsewhere. 16 Image analysis was performed independently by two operators to verify the nodal uptake values.
Combined qualitative and quantitative assessment of scans
The scans were inspected independently by two consultants blinded to participant status. Abnormal morphological features were (1) reduced regional node and lymphatic tract imaging (delay), in advanced cases functional aplasia (no imaging of tracks and nodes) or functional hypoplasia (very weak imaging of tracks and nodes), at 2 hours; (2) imaged popliteal nodes, indicating lymph diversion via the subfascial (deep muscle) system; and (3) dermal backflow (rerouting through the skin). Scans were assessed as either clearly abnormal (major morphological abnormality and reduced regional nodal uptake in the same limb), indeterminate (either a major morphological abnormality with normal uptake or normal morphology with reduced uptake), or normal (normal morphology and normal uptake). These outcome measures were considered the most discriminating and in line with recently published criteria. 16
Statistical analysis
Means and 95% CI are given, with the range for ages. Standard deviations (SDs) are shown in Figure 3. Sample size analysis showed that ∼15 participants would have ∼75% power to detect an effect size equivalent to ∼1 SD unit difference between a control and patient group in a two-sided test with an alpha (Type I error) rate of 0.05; despite limited available data on uptake and drainage from healthy individuals this might be defined as clinically important. All data sets were normally distributed. Group comparisons were made using one- or two-way analysis of variance (ANOVA) and Tukey's posttest. Significance was accepted at p < 0.05. All analyses were conducted in GraphPad Prism, version 7 (GraphPad Software, La Jolla, CA).
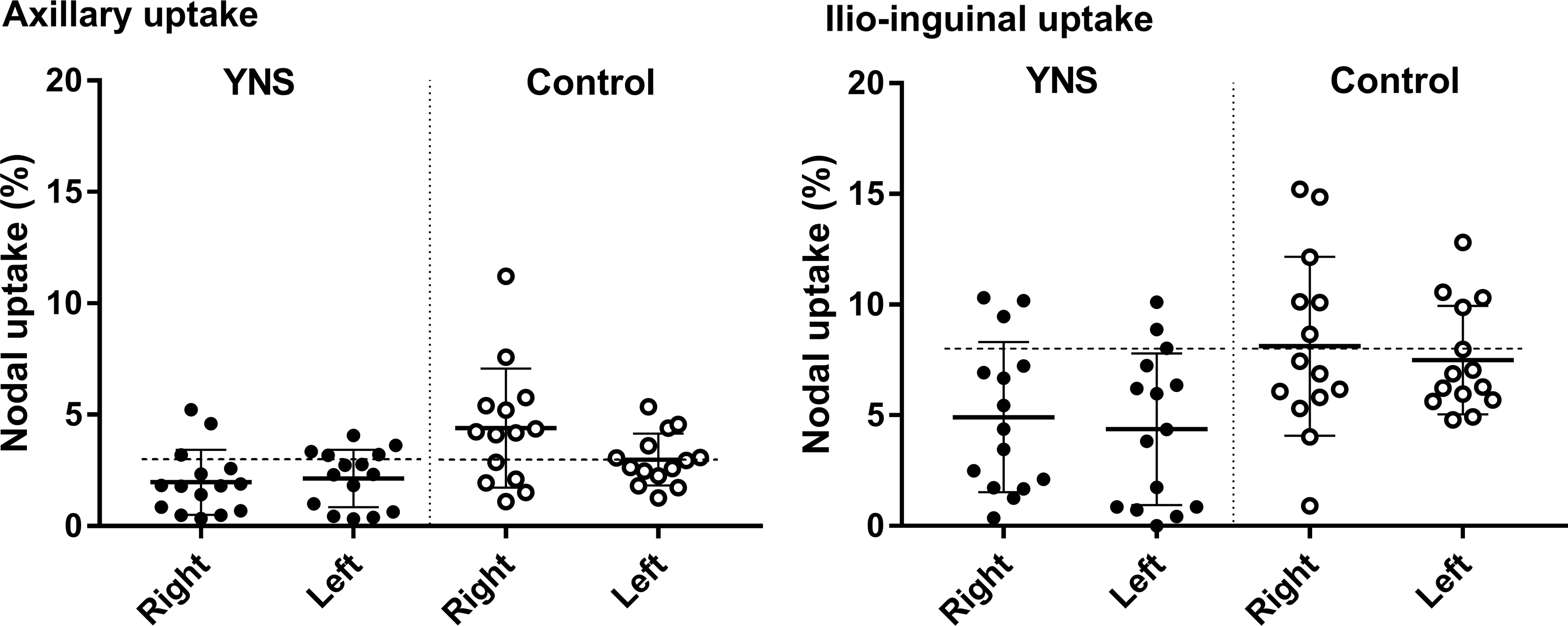
Axillary and ilio-inguinal nodal uptakes in patients with YNS and healthy controls. Nodal uptakes (%) for the right and left upper and lower limbs of individual participants are shown (n = 15 for YNS and n = 14 for controls), together with the means and SD. The dotted horizontal lines represent the normal lower limits of 3% for axillary uptake and 8% for ilio-inguinal uptake. Axillary uptake and ilio-inguinal uptake were both significantly lower in the YNS than the control group (p < 0.001 for averaged right and left values; see text). SD, standard deviation.
Results
Clinical findings in the YNS patients
On examination, 15/17 (88%) patients had nail abnormalities consisting of yellow–green discoloration, transverse overcurvature, thickening, onycholysis, and evidence of shedding (Fig. 1). The two patients with normal nails had exhibited YNS nail abnormalities previously for which documented evidence was seen. All patients had swelling below the knee; one patient had swelling confined to the feet, and one had above- and below-knee swelling. Stemmer's sign was positive in 12/17 (71%) patients. Three of the five patients with a negative Stemmer's sign had documented evidence of lymphedema and had been prescribed compression garments; the other two had characteristic below-knee swelling that pitted to some extent, indicating that lymphedema was indeed present. A negative Stemmer's sign does not exclude lymphedema. 17 Fourteen of the 17 patients, (82%) had upper limb swelling, but this was mild compared with the lower limb swelling; in 5 patients, the hand was swollen. One patient had generalized truncal swelling and one patient had facial swelling. The YNS had first presented at a mean age of 54 years (CI: 49–58 years, range 39–74 years) with a nail abnormality in 5/17 (29%), lymphedema in 6/17 (35%), or a respiratory manifestation such as sinusitis or chronic cough in 10/17 (59%). Four of the 17 patients (24%) reported two presenting symptoms. Nine of the 17 patients (53%) reported spontaneous resolution of their nail abnormalities (Fig. 1). Swelling presented initially in the ankles, feet, or hands. Hand swelling was the presenting symptom (in combination with nail abnormalities) in two patients. Fluctuation but not complete resolution of the edema was reported. Cellulitis affecting the lower limbs was reported in 4/17 (24%) patients, bronchiectasis in 13/17 (76%), and pleural effusion in 1/17 (6%).
Lymphatic function
Combined qualitative and quantitative assessment of lymph scans
YNS group: 10/15 (67%) YNS scans were clearly abnormal, 5/15 (33%) scans were indeterminate, and no scan was normal. While quantification was considered the more reliable outcome measure, it was deemed necessary to have both abnormal qualitative and quantitative measures to be sure of a clearly abnormal scan, particularly in view of the high rates of abnormalities in the healthy controls. The consistent morphological abnormality in the clearly abnormal scans was reduced imaging of regional nodes and lymphatic tracts, and functional aplasia was evident in all four limbs of YNS-016 and in the left lower limb of YNS-030. Four of the five indeterminate YNS scans showed normal morphology with reduced uptake.
Control group: 5/14 (36%) control scans were clearly abnormal, 6/14 (43%) scans were indeterminate, and 3/14 (21%) scans were normal. The morphological abnormalities in the abnormal scans were reduced nodal imaging, bilateral popliteal node imaging, and mild dermal backflow, with reduced uptake. The indeterminate control scans showed reduced uptake only.
Figure 2 shows the whole-body scans from two YNS patients (YNS-003 and YNS-030) and two controls (YNS-018 and YNS-028). Further details are given in the legend.
Quantitative findings
Figure 3 shows all the regional nodal uptake values for the upper and lower limbs of the YNS and control participants. Axillary uptake in the YNS patients (2.1%, CI: 1.3%–2.8%, n = 15) was lower than in the healthy control group (3.7%, CI: 2.7%–4.6%, n = 14) (right and left sides averaged), and ilio-inguinal uptake was also significantly reduced (YNS 4.6%, CI: 3.0%–6.3%, controls 7.8%, CI: 6.2%–9.4%; p = 0.0002, 2-way ANOVA). Ilio-inguinal uptake was higher than axillary uptake (p < 0.0001). Mean nodal uptake was thus reduced by 44% (axillary) and 41% (ilio-inguinal) in the patients relative to age-matched healthy controls. The mean axillary nodal and ilio-inguinal uptakes for each limb in the YNS group were below the accepted normal values, and at least one limb of every patient showed reduced uptake. In the control group, surprisingly, nodal uptakes were also near or below what is generally considered the normal limit. The given normal limits have been derived from a reference population of patients, not from healthy controls, and from all ages (therefore not matched with our control participants).
Hand swelling is not often seen in primary lymphedema. In two patients hand swelling was one of the first manifestations of the syndrome. Axillary uptake in the five patients with hand swelling was therefore compared with those without hand swelling and with the controls. Axillary uptake in the swollen hand group was 67% lower than in the nonswollen hand group (right and left sides averaged; n = 5 and 10, p = 0.060, one-way ANOVA, Tukey's posttest) and 76% lower than in the controls (n = 14, p = 0.001) (Fig. 4). Ilio-inguinal uptake in the swollen hand group showed a similar trend. Therefore, hand swelling appeared to indicate more profound lymph drainage impairment overall.

Axillary nodal uptakes in participants with and without hand swelling. Axillary uptakes (%) were compared in YNS patients with and without swollen hands and in controls (n = 5, 10, and 14 respectively, right and left sides averaged, means and 95% CI shown). Uptake was substantially lower in the swollen hand group than in both the nonswollen hand group (p = 0.060) and the control group (p = 0.001, one-way ANOVA, Tukey's post-test). ANOVA, analysis of variance; CI, confidence interval.
Discussion
There seems little doubt that YNS is a lymphatic phenotype because lymphatic insufficiency was found to exist in all patients and in the majority the insufficiency was widespread, including the upper limbs. The patients were assessed carefully on clinical grounds to confirm the diagnosis of YNS; the two patients without nail abnormalities had exhibited such abnormalities previously, but these had undergone remission. The main findings were as follows: (1) all patients had clinical evidence of lower limb lymphedema, 82% had mild upper limb involvement also, including 29% with hand swelling. (2) Using the combined qualitative and quantitative outcome criteria, 67% of scans in the YNS group were clearly abnormal (i.e., both qualitatively and quantitatively abnormal) and, surprisingly, 36% of scans in the control group were also clearly abnormal. (3) Evaluation of lymphatic function by quantitative analysis alone showed that regional nodal uptake was reduced by 41%–44% in both the upper and lower limbs of YNS patients relative to the control group.
Lymphatic function in the YNS patients
All the patients recruited for this study fulfilled the three criteria for YNS, namely the presence of discolored, dystrophic nails, lymphedema, and respiratory disease. The two patients without nail abnormalities had exhibited this previously when the diagnosis was originally made. The mechanism for the lymphatic insufficiency was consistent in all patients where it was observed, namely a failure of lymphatic transport through the main channels and not lymphatic obstruction or lymph reflux, mechanisms that are frequently observed in other forms of primary lymphedema. This means that there is either reduced uptake of material by initial lymphatics or reduced subsequent transport through the main collecting lymphatics adjoining the nodes. Patient scans with normal morphology of lymph drainage routes nevertheless all showed reduced uptake, the prevailing abnormality. The worst abnormality was functional aplasia, that is, no discernible drainage, which was interpreted as “shut down” of main lymphatic collector vessel drainage. Therefore, it seems likely that lymph vessel function diminishes progressively as the disease worsens, with morphological abnormalities becoming evident as the YNS becomes more advanced. Our findings are consistent with those of Samman and White, who performed direct contrast lymphangiography on four patients with YNS and identified a consistent reduction in the number of limb lymphatic collector vessels; in one patient, no main lymph vessels could be visualised. 1
From our findings, it was not possible to determine whether lymphatic dysfunction is a primary phenomenon in YNS. In other words, is there genetic predisposition for a weakness in lymph drainage in patients who subsequently develop the syndrome? The occurrence of congenital and familial forms of YNS would support the possibility of a genetic etiology, but there were no cases of a family history in the patients studied here. Alternatively, shut down of main collector vessels, possibly as a result of obliteration/atrophy of peripheral lymph vessels, could occur as a result of extrinsic or environmental factors, but such factors are unknown. There have been anecdotal reports of toxic materials such as titanium causing YNS. 3
The majority of patients had some upper limb involvement, although this was mild, and five of these had hand swelling. To our knowledge, upper limb lymphedema has not been previously reported in YNS. Lymphedema has been reported mainly to affect the lower limb and also the face and genitals.1,4,7,13 Upper limb involvement is less common than lower limb involvement in primary lymphedema and the upper limb has received less attention. In a recent series of patients with primary lymphedema (of any type) and upper limb swelling, the hand was always involved. 18 Our observation of substantially reduced axillary uptake in the subgroup of YNS patients with swollen hands is noteworthy, although based on a low n. The evidence for greater lymphatic impairment in the swollen hand subgroup indicates that such patients merit closer long-term clinical scrutiny. Lymphatic function in YNS (and in other forms of lymphedema) when hand swelling is present requires further exploration.
Lymphatic function in the healthy controls
Healthy age-matched controls were included for the first time in a case–control study involving lymphoscintigraphy. The difficulty in recruiting healthy volunteers for lymphoscintigraphy (because of the radiation dose) was overcome by recruiting sympathetic spouses and friends of the patients. To our surprise, however, 36% of the control scans were clearly abnormal and a further 43% were indeterminate (with a morphological abnormality or reduced uptake). The lymphatic insufficiency detected in these controls was not severe enough to manifest with clinical edema. Lymphoscintigraphy is considered to be a highly sensitive and reproducible imaging technique for lymphatic dysfunction,19–24 and the control group observations may be representative of the general population in the fifth decade of life onward. In view of this unexpected finding, further exploration of lymphatic function in healthy, middle-aged to elderly individuals is clearly warranted and would provide a sounder basis for the interpretation of patient scans.
Conclusions
A similar study published by our group in 1996 concluded that the underlying cause of YNS is not primarily a lymphatic abnormality because lymphatic drainage was significantly reduced in the legs of patients with YNS, but not to the level seen in lymphedema. 13 Our more modern study was more robust because of more careful assessment of patients before recruitment, greater numbers of patients with YNS, a more sensitive protocol for quantification of lymph transport, and inclusion of healthy volunteers as controls. We now conclude that lymphatic insufficiency is a significant contributory factor to the pathogenesis of YNS, and our findings provide the strongest indication that YNS is a lymphatic phenotype. The extent of the lymphedema, the presenting feature in a third of the patients, and the identical mechanistic fault in all patients together indicate that lymphatic dysfunction is an integral and determining feature of YNS. Future research should include genetic studies because it is difficult to see how the cause can otherwise be determined.
Footnotes
Acknowledgments
The research was supported by a grant from the Princes Exchange Foundation, Edinburgh for “the advancement, promotion or undertaking of medical research into the detection, diagnosis, treatment, causation, and prevention of YNS and/or Lymphoedema.” The grant was made possible by a legacy from a patient with YNS, to whom we are indebted. We thank the patients, their friends, and their families. We also thank the consultant skin and chest physicians and the Lymphoedema Support Network for help with recruitment; Dr David Lovell (St George's, University of London) for statistical advice; the staff of the Radiopharmacy Department, St George's Hospital for radiopharmaceutical preparation; and Mick Rogers (MIC Ltd.) for gamma camera technical support.
Author Disclosure Statement
No competing financial interests exist.