
Abstract
Abstract
Background:
Multiple staging systems for classifying the severity of lymphedema exist. The International Society of Lymphology (ISL) stage is considered standard for clinical reporting, but the relationship between clinical and functional/imaging stage remains poorly defined.
Materials and Methods:
We reviewed the prospectively collected data of all patients who underwent physiologic lymphedema surgery for a 3-year period by the senior author. Patients who underwent preoperative clinical staging with limb volume calculations and intraoperative indocyanine green (ICG) staging were included. Correlations were examined between ISL stage, ICG stage, and preoperative volume difference.
Results:
A total of 212 patients met inclusion criteria. ISL stage and preoperative volume difference had a Pearson correlation coefficient of 0.579 [p < 0.001, 95% confidence intervals, CIs (0.479–0.664)]; ICG stage and preoperative volume difference had a Pearson correlation coefficient of 0.338 [p < 0.001, 95% CIs (0.204–0.460)]; and ISL stage and ICG stage had a Pearson correlation coefficient of 0.254 [p < 0.001, 95% CIs (0.114–0.383)].
Conclusion:
Clinical ISL stage does not correlate well with ICG stage in patients undergoing physiologic lymphedema surgery.
Introduction
S
International Society of Lymphology Staging System (Derived from Reference #10)
More recently, the introduction of indocyanine green (ICG) lymphography has added a new dimension to the diagnosis of lymphedema and has enhanced localizing functioning lymphatic channels intraoperatively for potential bypass.4–7 Several reports by Yamamoto et al. describe using an ICG lymphography dermal backflow (DBF) pattern system for staging.5,6,15 In an attempt to find more functionally relevant classification system, the senior author (D.W.C.) developed a four-stage ICG lymphography staging system based on the presence of functioning lymphatic channels and the extent of DBF (Table 2). 7 In a clinical setting, we have often observed that the clinical staging of lymphedema based on physical examination does not necessarily correlate with the ICG findings.
Indocyanine Green Staging System (Lymphedema Classification Derived from Reference #7)
DBF, dermal backflow.
The aim of the present study is to address the following question: “Does clinical staging have significant relevance in selecting physiologic surgical procedures for patients with lymphedema?” We reviewed our series of lymphedema patients treated with physiologic surgery to determine the relationship between clinical and ICG staging in an effort to ultimately better understand correlation between pathophysiological and physical manifestations of the disease. Furthermore, we aim to identify the relationship between staging and preoperative volume differences. The surgical outcomes of this study will be analyzed and published in another study.
Materials and Methods
We conducted a review of the senior author's (D.W.C.) patients who underwent physiologic lymphedema surgery from October 2013 to November 2016. This included patients who underwent vascularized lymph node transfer (VLNT), lymphovenous anastomosis (LVA), or combined VLNT+LVA. The study received approval from the Institutional Review Board of The University of Chicago Biological Sciences Division (IRB Reference #16-1315). Collected demographic data included patient gender, age, body mass index (BMI), duration of lymphedema, etiology (primary vs. secondary), and limb involvement (upper vs. lower). Patients with bilateral limb involvement were excluded. In addition, patients who underwent multiple staged surgeries were excluded.
Preoperative volume calculation and clinical staging
All patients were assessed preoperatively, typically the day before surgery, by trained lymphedema therapists who were blinded to the results of the ICG lymphography. Volumetric analysis was performed using an optoelectronic limb volumeter (Perometer model and software; Pero-System, Wuppertal, Germany), which uses infrared light to scan the limb and then performs a circumference measurement every 0.5 cm to calculate the total volume of the limb. Three measurements were performed and then averaged. The volume difference was calculated as follows: (volume of the lymphedematous limb–volume of the normal limb)/volume of the normal limb. The same therapist assigned a clinical ISL stage to each patient based on physical examination findings.
ICG staging
ICG lymphography was conducted on the day of surgery. For the upper limb, 0.01–0.02 mL of ICG (Akorn, Inc., Lake Forest, IL) was injected intradermally into each webspace and at volar radial and ulnar wrist of the lymphedematous limb. For the lower limb, ICG was injected into each webspace and just inferior to the medial and lateral malleoli. Soon after the injections, a near-infrared camera system (Photodynamic Eye; Hamamatsu Photonics K.K., Hamamatsu, Japan) was used to visualize fluorescent images of the lymphatic vessels, and lymphedema severity was classified using the previously described ICG lymphographic staging system. 7
Statistical analysis
Patient characteristics are reported as means with standard deviations or 95% confidence intervals (CIs). Statistical analysis was conducted using R version 3.2.3 (R Foundation for Statistical Computing, Vienna, Austria). Pearson correlation coefficients, CIs, and p-values were computed using the test for association/correlation between paired samples. And 95% CIs are reported for correlation data.
Results
Patient characteristics
A total of 226 consecutive physiologic lymphedema surgeries were performed in 219 patients, with 7 patients undergoing repeat procedures, leaving 212 patients for inclusion in the study. Preoperative patient characteristics are summarized in Table 3. Twenty-two (10.38%) were men and 190 (89.62%) were women. Thirty-two patients (15.1%) had primary lymphedema, whereas 180 (84.9%) had secondary lymphedema. Upper extremity involvement was present in 130 patients (61.32%), with the lower extremity involved in 82 patients (38.68%). Average age was 53.13 ± 11.7 years and average BMI was 27 ± 4.95. Patients had lymphedema for an average of 99 ± 124.59 months before surgery. Average preoperative limb volume difference was 23.4% [95% CIs (20.6–26.1)].
Preoperative Patient Characteristics
BMI, body mass index.
Correlations
ISL stage and preoperative volume difference had a correlation coefficient of 0.579 [p < 0.001, 95% CIs (0.479–0.664)]. ICG stage and preoperative volume difference had a correlation coefficient of 0.338 [p < 0.001, 95% CIs (0.204–0.460)]. Finally, in evaluating the relationship between ISL stage and ICG stage, a correlation coefficient of 0.254 [p < 0.001, 95% CIs (0.114–0.383)] was found. There was no difference between primary versus secondary or upper versus lower extremity.
Discussion
Despite advances in lymphedema treatment, a major challenge continues to be the lack of universally accepted assessment tools that correlate clinical and surgical findings. Such tools would aid in patient selection for different treatment modalities, as well as unify reporting on therapeutic outcomes. Accurate lymphedema staging is crucial for evaluation and follow-up for treatment of lymphedema. The ideal staging system should be comprehensive, reproducible, and have correlation between clinical, imaging, and functional assessments.
Clinical evaluation of lymphedema includes the incorporation of symptomology, reversibility, and appearance. Campisi et al. established a commonly accepted staging system attempting to incorporate all of these factors, with the original classification having five levels, ranging from subclinical lymphedema to elephantiasis. 12 In 2009 and 2013, the ISL met to agree on a simplified four-stage system, which is now generally accepted as standard. 10 The stages can be further divided by volume differential into minimal (<20%), moderate (20%–40%), and severe (>40%). However, the ISL system, although reproducible, does not sufficiently incorporate the physiologic features of lymphedema. Moreover, volume is a notoriously fickle examination tool, as it depends largely upon factors such as time of day when measurements are done and compliance with nonsurgical therapy.
Evaluation of lymphedema attained a new dimension with the introduction of ICG lymphography assessment. The use of a near-infrared camera to evaluate the limb after intradermal injection of ICG heralded a safe and minimally invasive way of viewing the superficial lymphatics up to a depth of 20 mm. 4 This also enabled the surgeon to delineate suitable lymphatics for LVA. 7 Various authors, primarily Yamamoto et al., sought to further define the role of ICG lymphography in diagnosing the severity of lymphedema, describing linear and DBF patterns of ICG spread in the extremities.5,6,12 They further divided the DBF into progressively worse patterns of splash, stardust, and then diffuse. In an analysis of 90 lower extremities correlating ICG staging with Campisi staging, they found that DBF patterns were more proximal in earlier stages, with progressive spread distally in more severe stages and worsening with duration of lymphedema. 5 In a mirror article analyzing 20 unilateral upper extremity lymphedema patients, they found a similar correlation with proximal to distal extent of DBF. 6 The group also suggests differing DBF patterns in primary and secondary lymphedema cases, as well as reduced velocity of dynamic ICG lymphography in worsening lymphedema.16,17 In a study linking these findings with clinical relevance, Akita et al. evaluated 50 gynecological cancer surgical patients pre- and postoperatively, finding a 27% incidence of lower extremity lymphedema. They suggested early intervention in stardust DBF patterns, as almost all of these patients had clinically significant lymphedema at 12 months. 18
Although commendable, the ICG staging systems relying on DBF patterns are time consuming, requiring up to 18 hours for recording, and can be complex in reading and interpretation for the less experienced operator.16,17 In 2013, Chang et al. presented a simplified ICG lymphographic staging system that could be used immediately preoperatively to identify appropriate lymphatic channels for bypass. 7 Furthermore, correlating the ICG stages with results of LVA surgery, we found that stage 1 and 2 patients received a higher mean number of bypasses and had significantly better results than patients with stage 3 or 4 lymphedema. The mean volume differential reductions at 6 and 12 months after LVA in the lymphedematous limbs of the stage 1 or 2 group were 52% and 61%, respectively, whereas the corresponding values were 16% and 17% in the stage 3 or 4 group.
Of note, besides clinical and ICG lymphographic staging, others have attempted to utilize lymphoscintigraphic findings and MRI to assess severity of lymphedema.2,3,13,19 In particular, Maegawa et al. analyzed lymphoscintigraphy in 142 cases of secondary lymphedema of the lower extremity. 2 They classified findings into five types and suggested that lymphaticovenous anastomosis was best indicated in type III. However, lymphoscintigraphy is invasive and involves the use of radioactive Technetium-99, whereas MRI is still relatively expensive.
This study demonstrates a weak correlation between clinical (ISL) and functional/imaging (ICG) staging. Therefore, we assert that physical examination findings alone should not be used in preoperative decision making for physiologic lymphedema surgery. Traditionally, LVA has been recommended for patients with clinically less severe disease (ISL stage I/II), whereas VLNT has been recommended for clinically more advanced disease. 20 This study challenges that paradigm. A patient with low ISL stage may, in fact, have high ICG stage, making the ability to perform LVA difficult due to lack of available target vessels (Fig. 1). Furthermore, as Chang et al. showed previously, these patients would experience less volume reduction if they underwent LVA alone. 7 The converse is also true, in that higher ISL stage does not necessarily indicate high ICG stage, and some patients with higher ISL stage may actually be good candidates for LVA (Fig. 2).
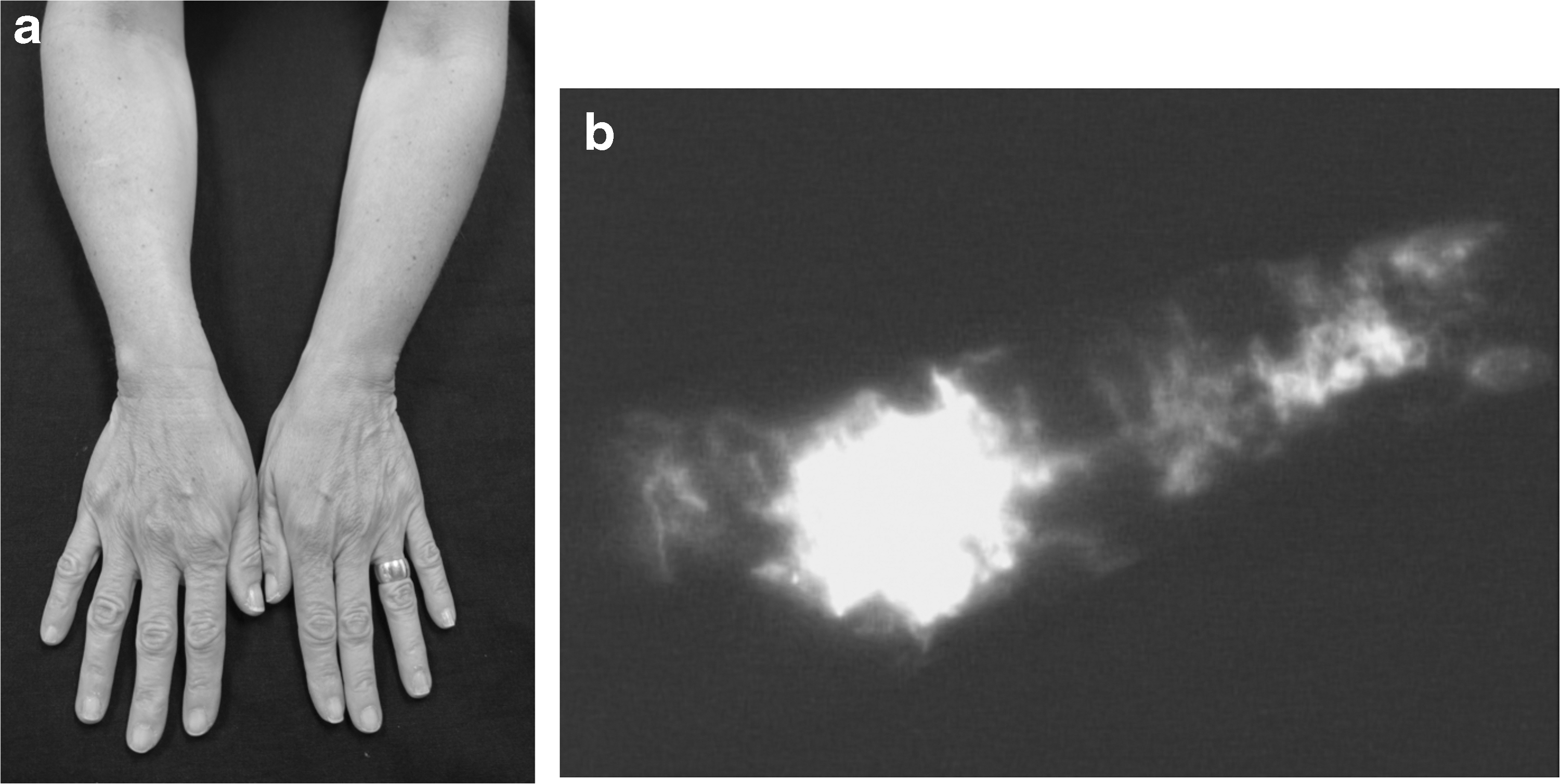
ISL stage I (mild) and ICG stage 3—62 years old F (BMI 26) with secondary RUE lymphedema (duration 59 months) after right axillary lymph node dissection and radiation. Patient underwent left supraclavicular VLNT to right axilla and LVA x3.
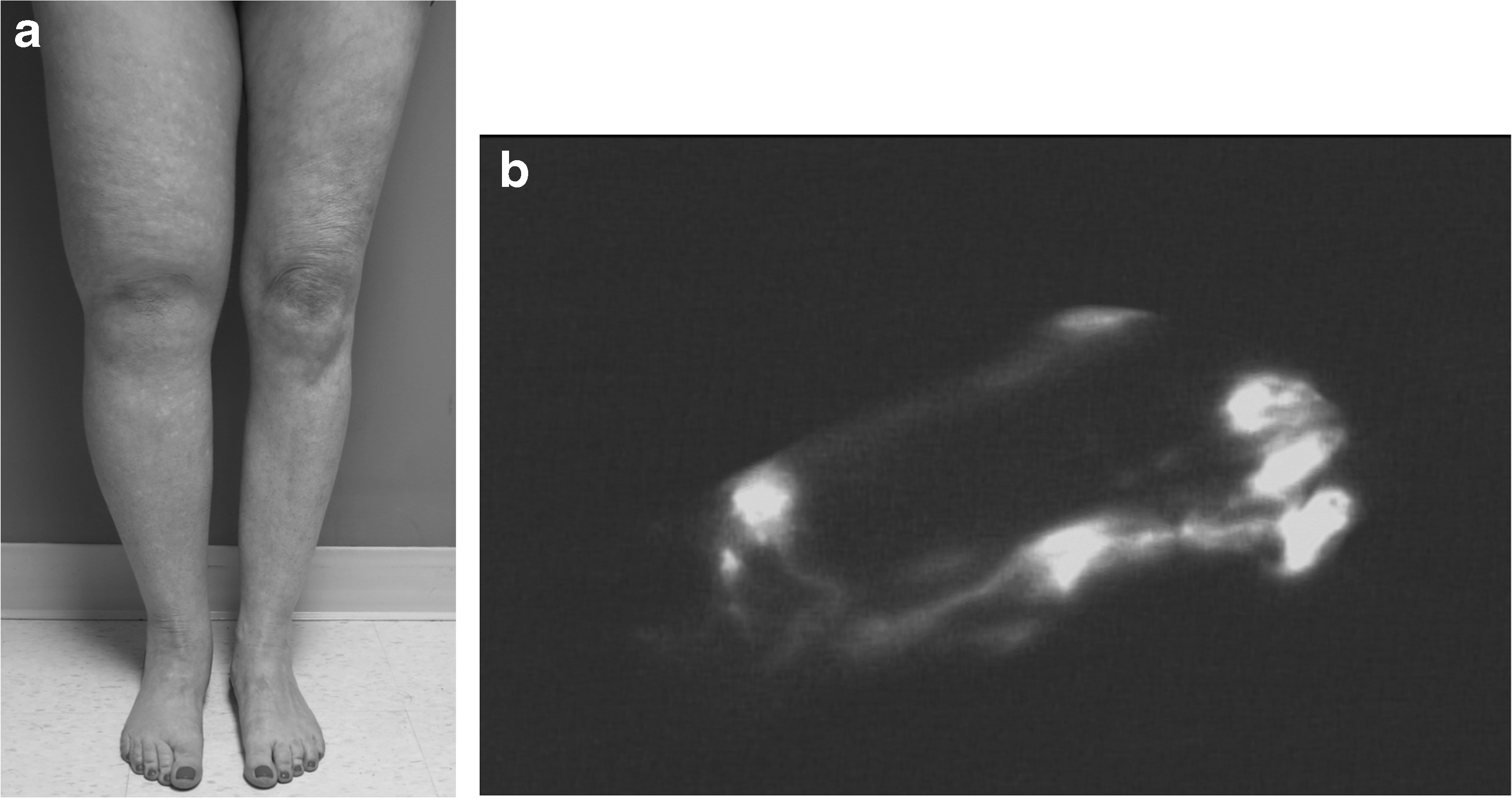
ISL stage II (severe) and ICG stage 2—55 years old F (BMI 25) with primary RLE lymphedema (duration 39 years). Patient underwent right supraclavicular VLNT to right groin and LVA x4.
A stronger correlation was observed between ICG stage and preoperative volume difference between limbs, although the strength of this correlation would still be considered relatively weak, and the difference between these correlations is not statistically significant (as indicated by the overlapping 95% CIs). Therefore, we do not suggest that volume difference alone be used as a surrogate measure for ICG stage. The strongest correlation was observed between ISL stage and preoperative volume difference. This correlation is significantly stronger than the other two reported correlations (as indicated by the nonoverlapping 95% CIs). This is not unexpected, as ISL staging relies on the physical examination, and this strong correlation further validates the ISL staging system as a clinical tool.
In the future study, we will correlate staging data with surgical outcomes and investigate how clinical and functional staging systems can be used to help predict surgical outcomes after physiologic surgery. Ultimately, we hope to have a better understanding of the significance of classification systems in selecting patients for lymphedema surgery.
Conclusions
“Does clinical staging have significant relevance in selecting physiologic surgical procedures for patients with lymphedema?” This study demonstrated weak correlation found between ISL and ICG stage, indicating that physical examination and clinical staging are inadequate for assessing lymphatic function.
Footnotes
Authors' Contributions
R.M.G., data collection and analysis, drafting, and revision of the article; A.S.H.O., project conception, data collection, drafting, and revision of the article; J.F., data analysis, drafting, and revision of the article; D.W.C., project conception, data collection, and revision of the article.
Author Disclosure Statement
No competing financial interests exist.