
Abstract
Abstract
Many basic and clinical studies have demonstrated that atherosclerosis is a chronic inflammatory disease. Although there are many factors affecting atherosclerosis, the role of lymphatic vessels in this disease has been neglected. Traditionally, lymphatic vessels have been considered to be passages for transporting interstitial fluid to the blood circulation. However, as early as the last century, researchers found that there are numerous lymphatic vessels surrounding sites of atherosclerosis; however, the relationship between lymphatic vessels and atherosclerosis is not clear. With further research, lymphatic vessels were determined to be involved in the induction and resolution of arterial inflammation and also to play a positive role in plaque cholesterol transport. There are abundant immune cells around atherosclerosis, and these immune cells not only have a significant impact on plaque formation but also affect local lymphangiogenesis (IAL). This promotion of IAL seems to relieve the progression of atherosclerosis. Therefore, research into the relationship between lymphatic vessels and atherosclerosis is of great importance for improving atherosclerosis treatment. This review highlights what is known about the relationship between lymphatic vessels and atherosclerosis, including the effect of immune cells on IAL, and reverse cholesterol transport. In addition, we present some of our views on the improvement of atherosclerosis treatment, which have significant clinical value in research.
Introduction
I
In recent years, it was found that lymphatic vessels not only directly participate in the induction and resolution of inflammation but also play an important role in cholesterol transport.4,5 In the early stages of atherosclerosis, an abundance of immune cells accumulates in the plaques, and these immune cells not only have a significant effect on atherosclerosis but also affect local lymphangiogenesis (IAL).6–8 Inflammation-associated IAL is thought to alter the course of inflammation and tissue repair, which was confirmed in a study on the inhibition or induction of IAL in mice. 9 It is an indisputable fact that lymphatic vessels are involved in reverse cholesterol transport (RCT) 10 ; however, the process of HDL entry into lymphatic capillaries is unclear, and further studies are warranted to elucidate this process.
Atherosclerosis is a chronic inflammatory disease, and the functional activation of lymphatic vessels has been shown to be crucial for resolving chronic inflammation and limiting acute inflammation. 5 Furthermore, plaque cholesterol excretions also rely on lymphatic vessel transport. 11 Taking these facts into consideration, perhaps strategies to improve lymphatic function or promote IAL may contribute to alleviating the progression of atherosclerosis. Therefore, it is necessary to better understand the relationship between lymphatic vessels and immune cells in atherosclerosis and, moreover, how HDL enters lymphatic vessels and eventually gets excreted through the liver. Such an understanding is necessary for the treatment and prevention of atherosclerosis. This review primarily describes links between atherosclerosis and lymphatic vessels, including arterial inflammation and cholesterol transport, and provides a theoretical basis for the treatment of atherosclerosis.
The Function and Structure of Lymphatic Vessels
In the 18th century, some researchers called lymphatic vessels “absorbents” (vasa absorbantia), because their function is to absorb liquid waste. 12 Further studies have found that the lymphatic vasculature plays an important role in inflammation, cholesterol transport, and other diseases.4,13
Blood vessels deliver oxygen, nutrients, and hormones to organs and tissues, and these compounds exchange molecules with surrounding tissues through capillaries. Blood pressure can cause plasma to leak continuously into the interstitial space from the capillary, and thus, the protein content of plasma and interstitial fluid is different. The key function of the lymphatic system is to return this protein-rich interstitial fluid to the bloodstream. 14 The interstitial fluid contains macromolecules, leukocytes, and activated antigen-presenting cells (APCs), which enter the blind-ended lymphatic capillaries. 14 The collected fluid, immune cells, and macromolecules form lymph, which is transported by collecting lymphatic vessels to the lymph nodes (LNs). 12 In the lymphatic vasculature, the LN is an especially organized microstructure that supports optimal immune surveillance. The “filtered” lymph (including both naive and activated lymphocytes and macromolecules) exits the LN through efferent lymphatic vessels. The lymph in the lymphatic vessels eventually returns to the blood circulation through the lymphatic-venous junctions in the jugular area. 15 Together, lymphatic capillaries, collecting lymphatic vessels and LNs provide protective immunity for the body. 16
The relatively large vessels of the lymphatic capillaries are the thinnest lymphatic vessels, composed of a monolayer of oak-leaf shaped endothelial cells. 17 Anchoring filaments are a characteristic feature of lymphatic capillaries; they connect the abluminal membrane of endothelial cells to the surrounding elastic fibers, involving the lumen lymph flow. 18 Lymphatic capillaries are not sheathed in smooth muscle cells, and the basement membrane is scarce or nonexistent. However, there are smooth muscle cell layers and basement membrane around the collecting lymphatic vessel, and the lumen is accompanied by valve structure (Fig. 1). The contraction of smooth muscle cells (SMCs) contributes to lymph propulsion, and the valves prevent backflow. 14 Lymph propulsion can also be influenced by external factors, such as inflammatory responses, skeletal movements, and interstitial pressure. 19 However, it is important to emphasize that lymphatic vessels are not only part of the venous system but also appear to deliver larger molecules and cells that do not readily traverse the venous wall. In patients with tumors, lymphatic vessels can transport molecules with a larger radius than tumor necrosis factor-α (3.24 nm), 4 while the radius of the lipoprotein is undoubtedly much larger than this.
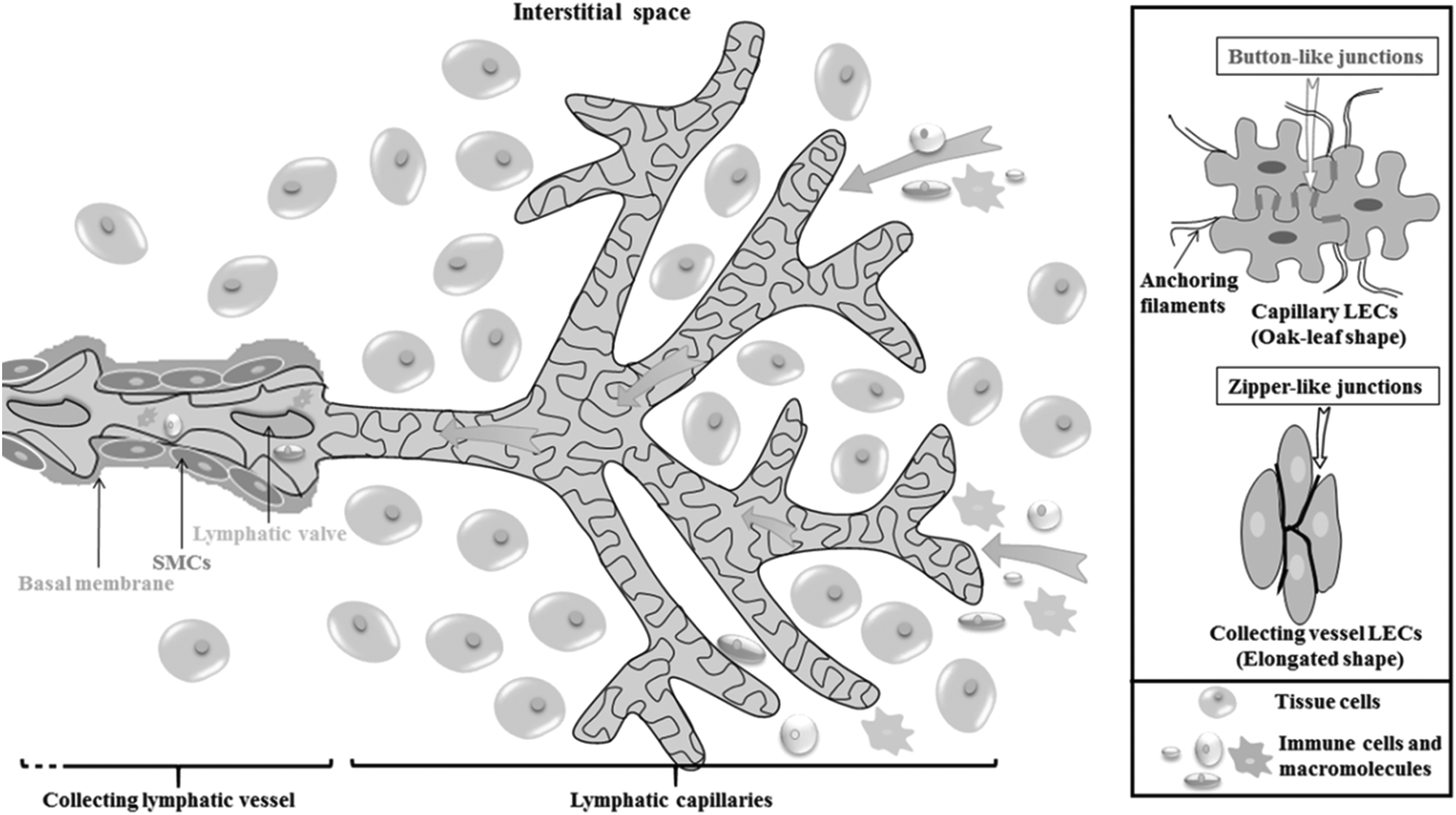
Structure of lymphatic capillaries and collecting lymphatic vessels. Initial lymphatic capillaries consist of LECs with “button-like” junctions that allow for easy entry of fluid, proteins, and immune cells into the lumen. Collecting lymphatic vessel transport the lymph toward LNs and eventually to the blood circulation. Intraluminal lymphatic valves, SMCs, and skeletal movements coordinate lymph propulsion and the direction of flow. LEC, lymphatic endothelial cell; LN, lymph node; SMCs, smooth muscle cells.
Early Lymphatic Vessels and Atherosclerosis-Related Clues
Earlier studies indicated that the coronary artery is protected from atherosclerosis due to the widespread presence of lymphatic vessels around it. 20 An initial study was performed to confirm whether there were lymphatic vessels in the wall of the artery. In the early 1990s, Sacchi and Comparini 21 studied the lymphatic vessels of the carotid and thoracic aorta in rabbits using histological methods. It was found that lymphatic vessels were not detected in the intima or media of the arteries, but a small number of lymphatic vessels were found in the adventitia and surrounding areas. As the research progressed, the adventitial lymphatic vessels were increasingly found to be related to the progress of atherosclerosis. Xu et al. 22 further expanded on the relationship between lymphatic vessels and intima by studying the rat aortic wall.
An essential finding of this study was that aortic intimal hyperplasia after balloon-induced endothelial injury is accompanied not only by significant adventitial angiogenesis but also by the extensive proliferation of adventitial lymphatic vessels. Drozdz et al. 23 studied eighty-one arterial segments of large arteries (abdominal aortas and iliac arteries) that were obtained from deceased organ donors. Lymphatic vessels were identified using antiLYVE-1 and anti-D2-40/podoplanin immunohistochemical staining. It was found that the density of adventitial lymphatic vessels increased with the progression of atherosclerosis, depending on the thickness of the intima. Kutkut et al. 24 further studied the location of lymphatic vessels in arteries. This group not only demonstrated that lymphatic vessels are present in the adventitia of human coronary arteries, but they also detected small lymphatic vessels within atherosclerotic lesions. In conclusion, lymphatic vessels exist in the adventitia of various animal arteries, such as rats, mice, and rabbits, similar to the human condition.
Arterial Inflammation Promotes IAL
In healthy adults, lymphatic vasculature is stable and has no IAL. However, lymphatic vessels undergo significant changes in inflammatory-induced pathologies, including IAL and lymphatic vessel hyperplasia. 25 Arterial inflammation is an important component of atherosclerotic disease-specific immune responses against autoantigens or pathogen-derived antigens in the blood vessel wall, and this inflammation could initiate and maintain atherosclerotic processes. At present, basic and clinical studies have confirmed that atherosclerosis is a chronic inflammatory disease. During atherosclerosis, the adventitial lymphatic vessel density increases with increasing intima thickness. A few years ago about the relationship between arterial wall IAL and atherosclerosis have been studied. Grzegorek et al. 26 analyzed 26 iliac artery specimens and found that the chemokine receptor CCR7 of CCL19/CCL21 plays a putative role in atherosclerosis and IAL.
Under arterial inflammation conditions, an abundance of immune cells accumulates around injured blood vessels. 27 Although inflammation is confined primarily to the plaque itself, increasing reports indicate that many immune cells (including macrophages and granulocytes) infiltrate the arterial wall,6,28 which also appears to affect adventitial IAL. 29 In addition, lymphatic vessels in the adventitial can also promote the recruitment of immune cells that accumulate in the peripheral tissue. 9 Macrophages and antigen-bearing dendritic cells (DCs) enter the lymphatic vessels in peripheral tissue by discontinuous “button-like” junctions or preformed portals30,31 and by collecting lymphatic vessels which continue to move into regional LNs, which are key locations for producing specific immune responses. Numerous prolymphangiogenic signaling pathways are activated upon exposure to inflammatory stimuli, and the role of VEGF-C/VEGFR3 is the best-characterized pathway in the process of IAL. 9 Proinflammatory cytokines induce the transcription of VEGF-C messenger RNA, likely through the activation of NF-κB-mediated promoters, suggesting that these cytokines regulate IAL during inflammation. 32 This interaction between immune cells and lymphatic vessels contributes to the immune system response to inflammatory stimuli.
Lymphatic Vessels and Immune Cells in Atherosclerosis
Macrophages
Macrophages can generally be divided into the following three groups: perivascular macrophages, tissue-resident macrophages, and recruited macrophages. 33 Macrophages are the most abundant immune cell type present in atherosclerotic lesions. However, the distinctions between these macrophages are unclear, because an exclusive lineage marker has yet to be identified for these subpopulations, and many studies have simply merged this group. 34 In this study, we primarily emphasize the effect of plaque macrophages on IAL.
Bone marrow-derived macrophages are dispatched into the blood circulation and transported into the plaque, where they clear debris and phagocytose pathogens. Then, they move from plaque to regional LNs through lymphatic capillaries, which is a significant process for resolving inflammation. 35 Llodra et al. 36 studied a mouse model of atherosclerosis documenting the migration of macrophages into regional LNs during plaque clearance. In inflammatory tissues, LECs express chemotactic or adhesion molecules that promote the migration of macrophages to LNs. In turn, macrophages secrete paracrine lymphatic growth factors, such as VEGF-C/VEGF-D, to stimulate IAL.37,38
Numerous studies support the dramatic accumulation or recruitment of macrophages and the production of VEGF-C during inflammation-induced IAL. 29 Apart from paracrine mechanisms, macrophages are also thought to promote IAL by transdifferentiation into LECs. 38 Most of the evidence for this phenomenon is based on the colabeling of lymphatic markers and macrophage and cell-lineage studies that are similar to the analogous studies showing the transition of macrophages to blood endothelial cells. 29 Hall et al. demonstrated, via time-course analysis of lipopolysaccharide-stimulated IAL in the mouse diaphragm, that macrophage-derived LEC progenitors incorporated into the inflamed lymphatic vasculature and that cultured macrophages can be induced to express lymphatic markers. 39 The interactions between lymphatic vessels and macrophages lead to a reciprocal regulatory relationship during IAL.
Dendritic cells
DCs constitute a unique family of APCs that play a significant role in innate and adaptive immune responses. 40 DCs have been identified in both the normal and pathological intima. Thus, they play a role in all stages of atherosclerosis, with multiple functions, such as lipid accumulation, foam cell formation, proinflammatory cytokine secretion and antigen presentation.41,42 CCR-7 and its ligand CCL21/CCL19 are part of the most prominent chemokine pathway involved in DCs migration. 43 The LEC-secreted CCL21 is deposited at the basement membrane of collecting lymphatic vessels and aids the lymphatic vessels around atherosclerosis in recruiting DCs. 44 Inflammatory stimuli trigger LECs to express leukocyte adhesion receptors, such as VCAM-1, ICAM-1, and E-selectin, which mediate the entry of DCs into the lymphatic vessels and their trafficking through the afferent lymphatic vessels. 45 Furthermore, accumulating evidence indicates that the VEGF-C/VEGFR3 pathway is involved with activated DCs and LECs and is largely involved with the migration of DCs across the lymphatic vessels in LNs. Blocking VEGFR3 signals during corneal transplants and cardiac allografts leads to the ablation of DC migration from the transplant to host LNs. 29
Therefore, from the initial entry into the lymphatic capillaries, and then through collecting lymphatic vessel to LNs, DCs are always closely related to lymphatic vessels. Investigation into the molecular basis for DC migration will further elucidate the biological characteristics and functions of DCs and provide an important base for the treatment of atherosclerosis.
B and T cells
Multiple autopsy studies have reported the presence of B cells (or B lymphocytes) in both the plaque and adventitia surrounding atherosclerotic lesions, with a predominance of B cells in the adventitia. 46 The role of B cells in atherogenesis is less understood, although the contributions of macrophages, DCs, and other immune cells have been well studied. B cell aggregates have been observed near the adventitial microvessels and may undergo selection, maturation, and antibody production after antigen presentation by DCs. However, there is an abundance of B cells in LNs, which usually orchestrate IAL. Angeli and Randolph 47 demonstrated that B cells secrete VEGF-A, promoting LN angiogenesis during inflammation, resulting in increased intranodal DC mobilization and optimized immune activation.
T cell (or T lymphocyte) activation requires direct contact with an antigen, and naive T cells constantly circulate through secondary lymphoid organs (SLOs) in pursuit of antigen. 48 Antigen-specific naive T cells proliferate upon antigen encounter in SLOs and become activated effector T cells, which are then released from the SLO and enter the site of plaque inflammation. 49 Throughout the life cycle of T cells, lymphatic vessels and blood vessels act as highways for T cell circulation. Although there is much known about the migration of T cells across and within the blood vasculature, little is known about T cell migration into the lymphatic vasculature. Rademakers et al. 27 dissected the lymphatic vessel and found that plaque draining LNs in atherosclerotic apoE−/− mice aggravated intima thickness, with increased T cell accumulation in plaque and adventitia as a most prominent feature. Increased T cell accumulation was also observed following the systemic inhibition of VEGFR3-dependent IAL. This finding suggests that lymphatic vessels play an important role in trafficking T cells in the plaque. However, this study did not explain how the T cells in the plaque enter the lymphatic vessels. This study also found that adventitial IAL could not be halted by VEGF-C/D inhibition but was at least partly arrested due to non-classical IAL via the CXCL12/CXCR4 axis.
T cell recirculation through afferent lymphatic vessels is thought to contribute to immune surveillance with novel antigen specificity by continually replenishing T cell pools in peripheral tissues. 50 Furthermore, interferon gamma (IFN-γ) secreted by T cells downregulates the major lymphatic players, resulting in reduced IAL. 51 These findings suggest that T cells have an antilymphangiogenic effect in balancing the prolymphatic drive of macrophages and B cells to maintain lymphatic homeostasis in LNs. A better understanding of the role of plaque T-cell subsets in lymphatic function and IAL will contribute to the development of treatment for inflammation or vascular injury-induced atherosclerosis.
IAL Relieves the Progression of Arterial Inflammation
There is growing evidence that inflammation-induced IAL is not merely a bystander but profoundly alters inflammatory and tissue repair processes. 9 Studies have shown that immune cells closely interact with lymphatic vessels in a variety of pathophysiological processes, resulting in pro/antilymphangiogenic effects as well as DC migration. Inflammatory disorders and IAL are highly interconnected, and the regulation of IAL by macrophage-derived lymphatic growth factor modulation is a potential strategy for treating acute and chronic inflammatory disorders, as several preclinical and clinical studies have already indicated. Furthermore, B cell-induced LN-angiogenesis is clinically exploitable to promote efficient vaccine delivery or DC migration into LNs. However, in some diseases, IAL does not relieve the progress of the disease, and sometimes, it has the opposite effect. For example, in diabetic animal studies, there was IAL around islet cells, and this IAL could cause the pathogenesis of inflammation; inhibition of VEGFR3 reduced IAL at the islets, leading to a decrease in inflammation and thereby preserving the islets. 19 In tumor research, IAL can promote the metastasis of tumor cells through lymphatic vessels, a process of the malignant dissemination of tumor cells. 52
However, the induction of IAL may have beneficial effects against atherosclerosis. The most important complication of atherosclerosis is acute coronary syndrome, often culminating with myocardial infarction (MI). MI is followed by a robust inflammatory reaction characterized by the coordinated mobilization of different leukocyte subsets that aid in scavenging dead cardiomyocytes and released macromolecules while promoting granulation tissue formation and remodeling. 53 Studies have shown that after MI, cardiac lymphatic vessels undergo a profound lymphangiogenic response and that ectopic VEGF-C stimulation augments this lymphangiogenic response, resulting in a transient improvement in post-MI cardiac function. 54 Therefore, inducing IAL could provide a pathway for inflammatory cell efflux to tip the balance in favor of wound healing within the injured adult heart. 54 However, there is also an increase in the density of lymphatic vessels around atherosclerosis, 23 but it is unclear why the increased lymphatic vessels cannot alleviate the lesion. Perhaps newly formed lymphatic vessels are deficient in function 55 or the number of these newly formed lymphatic vessels is too low to cause a reversal of stubborn diseases such as atherosclerosis.
Lymphatic Vessels and Cholesterol Transport
RCT and HDL uptake
Cholesterol, which is a key component of the cell membrane, plays a vital role in controlling membrane fluidity and cell permeability. 56 Abnormal levels of cholesterol may cause atherosclerosis, hypercholesterolemia, type 2 diabetes, and other conditions. Accumulated cholesterol in peripheral tissues needs to be transferred back to the liver for recycling or excreted in bile acid with the feces; this process of removing cholesterol is known as RCT. 57 The macrophage cholesterol transport that occurs on the arterial intima is called macrophage-specific RCT (m-RCT). 58
A typical feature of early atherosclerosis is the accumulation of macrophages or foam cells with a high cholesterol load in the intima and the formation of stripe lipid plaques. 57 Therefore, the primary means of reducing cholesterol in cells include promoting the efflux of cholesterol from macrophages and reducing the accumulation of cholesterol in macrophages. The efflux of cholesterol from macrophages requires the action of ATP-binding cassette transporters A1and B1 (ABCA1, ABCG1),59,60 and the efflux of cholesterol can occur through uptake by HDL, which becomes HDL cholesterol (HDL-C). Finally, the major site of HDL-C uptake is the liver, which accounts for 65% of the total HDL-C uptake, through the HDL receptor scavenger receptor B1 (SR-B1). 61 ABCA1 also mediates the formation of nascent HDL particles (preβ1-HDL) between cholesterol and lipid-poor apolipoprotein A1 (apoA-I), which are eventually modified into larger particles by a series of enzymes, such as lecithin cholesterol acyltransferase. 62 Mature HDL can be remodeled with the involvement of many lipases (endothelial lipase or hepatic lipase) and SR-B1 to form smaller disc-shaped HDL and spherical HDL particles that are susceptible to faster catabolism. 4
Currently, the level of HDL is measured in the plasma, but most of the life cycle of HDL occurs in the interstitial space, and the return of interstitial HDL to the plasma requires transport through the lymphatic vessels. 63 The source of HDL in the interstitial fluid is partly derived from the plasma and partly derived from the synthesis of the initial HDL (preβ-HDL). 4 Much research has been done on the promotion of cholesterol efflux from macrophages and the final metabolism of HDL-C. However, lymphatic vessels participate in RCT, and many aspects of this process remain to be clarified.
The study of lymphatic vessels in RCT
The key function of lymphatic vessels is to return abundant lipoproteins in the peripheral tissues to the bloodstream, maintaining lipoprotein concentrations in peripheral tissues at a low level. 64 Nanjee et al. 65 found that the concentration of HDL cholesterol was 30% higher in lymph compared to blood, by carefully analyzing the various lipoprotein fractions in human lymph. Another recent study using fluorescent analogs to track cholesterol transporters out of the skin also concluded that skin RCT is quantitatively dependent on lymphatic vessels. 66
To determine whether lymphatic vessels have an essential role in transporting HDL cholesterol, Martel and Randolph 57 studied the role of lymphatic vessels during RCT in atherosclerotic mice. They removed the aorta from donor atherosclerotic apoE-deficient mice with labeled cholesterol and transplanted the aorta into recipient apoE-deficient mice, and then they applied the anti-VEGFR3 antibody (blocking lymphatic regrowth) or the control antibody (allowing lymphatic regrowth) treatment to recipient mice. It was found that the labeled cholesterol was retained in aortae of anti-VEGFR3 antibody-treated mice, indicating that lymphatic vessels participate in m-RCT. 57 Moreover, lymphatic vessels passively transport cholesterol from the peripheral tissues to the blood circulation, as expected, depending on the HDL and SR-B1 activity. SR-B1, which is the only membrane receptor on the cell that mediates HDL interactions and has HDL transport function, can exist in many types of cell membranes (including LECs). It is interesting that the “button-like” structure of the lymphatic capillaries appears to be able to introduce HDL into lymphatic capillaries in a nonselective manner, such as following interstitial fluid and macromolecules. However, some researchers believe that cholesterol selectively enters the lymphatic vessels, mediated through SR-B1. Lim et al. 66 used anti-SR-B1 antibodies to block the lymphatic vessel transport of HDL and found a significant reduction of labeled cholesterol in the plasma, lymph, and LNs; this finding indicates that SR-B1 is indispensable for the participation of lymphatic vessels in RCT (Fig. 2).

HDL-C enters the adventitial lymphatic vessels from the arterial intima. ABCA1 and ABCG1 promote efflux of cholesterol in macrophages or foam cells. HDL uptake cholesterol will be transported to the surface of LECs, combined with the SR-B1 by “caveolae” delivery to the lymphatic lumen, and then returned to the plasma compartment. SR-B1, scavenger receptor B1.
Therefore, the manner of entry of plaque HDL into the adventitia lymphatic vessels remains to be further elucidated. It is also possible that plaque HDL enters the adventitial lymphatic vessels is a manner that integrates these two methods. Lymphatic vessels are indisputably involved in RCT, but the question remains whether local IAL can accelerate plaque cholesterol transport. To investigate these issues, we first need to clarify how plaque HDL enters the adventitial lymphatic vessels, which is related to lymphatic transport efficiency.
Drug Delivery and Therapeutic Outlook
Lymphatic drug delivery systems have been extensively studied because drugs can bypass the first-pass metabolism of the liver via the lymphatic route, which increases oral bioavailability. 67 The current treatments for atherosclerosis are primarily lipid-lowering drugs, antiplatelet drugs, and vasodilators, but these drugs do not have a radical effect. Lymph has a one-way flow in the lymphatic vessels, and using the lymphatic system for drug delivery to treat atherosclerosis is estimated to be unfeasible. However, lymphatic system drug delivery may improve atherosclerosis in patients with impaired lymphatic function.
Recent studies have shown that Panx1 and apoA-I play a role in the regulation of lymphatic function, which provides a new potential therapeutic target for the prevention and treatment of atherosclerosis.68,69 Interstitial injection targeting the lymphatic system could be used to specifically deliver drugs to collecting lymphatic vessels or draining LNs. In pathologies such as chronic inflammation and lymphedema, functional IAL may be desired. In developed countries, the major cause of lymphedema is the destruction of the LNs or lymphatic vasculature by radiation therapy or cancer surgery. 13 Promising results have been demonstrated by several recent experimental therapies, including the induction of IAL with growth factors, apart from LN transplantation, in the treatment of lymphedema. 13
IAL is thought to be necessary to limit acute inflammation and to resolve chronic inflammation. 5 It may be feasible to relieve the development of chronic inflammation by delivering lymphatic growth factors under the condition of arterial inflammation. For example, Güç et al. 70 used a low and single dose of fibrin-binding VEGF-C to induce local, functional IAL, which promoted immune cells to migrate to the LN, in turn reducing the development of inflammation and improving wound healing. There is an abundance of immune cells at sites of atherosclerosis, and these immune cells are closely related to IAL. Understanding the relationship between immune cells, IAL and atherosclerosis is important for improving atherosclerosis treatment. In the meantime, RCT also quantitatively depends on the lymphatic transport, and the promotion of local IAL may be able to increase plaque cholesterol metabolism.
The role of the lymphatic system in antigen trafficking could serve as a sophisticated platform for next-generation vaccines. The interstitial fluid can be doped by injecting specific antigens, which are transported to the LNs where the desired immune response can be triggered. 71 Recent examples of nanoparticles that are designed to reach the LNs and modulate the immune response are PEGylated polystyrene nanoparticles and PEGylated cationic liposomes.72,73
Overall, it is hypothesized that improving lymphatic function or promoting IAL could aid in the treatment of atherosclerosis. Recent advances in the fields of preclinical disease models, molecular lymphatic markers, and noninvasive imaging methods have provided exciting new insights, indicating that targeting the lymphatic vasculature may provide promising new opportunities for the in vivo imaging of and drug delivery to sites of atherosclerosis or other conditions.
Unsolved Problems
The involvement of the lymphatic vessels in m-RCT is an indisputable fact. However, there are still many questions to be answered regarding the relationship between RCT and lymphatic vessels. For example, as atherosclerosis progresses, lymphatic vessel density increases, but why does this increase not relieve the inflammation of the arteries? Researchers have extensively used apoE-deficient animals to clarify the relationship between lymphatic vessels and m-RCT.11,66 However, the basis of lymphatic defects in apoE-deficient mice is still not clear, and researchers have considered the use of VEGF-C/VEGFR3 signaling deletion to clarify the role of lymphatic vessels in cholesterol transport. It was previously shown that lymphocytes, macrophages, and DCs could egress from the regressing atherosclerotic plaque through the lymphatic system, but the relationship between these cells in atherosclerosis and lymphatic vessels needs to be further elucidated.
The mode of entry of HDL into the lymphatic capillary also needs to be further elucidated, including the selective loss of SR-B1 in LECs, to confirm that HDL-C transport in lymphatic vessels reflects the direct uptake by lymphatic endothelium rather than passive movement with the interstitial fluid. Lymphatic vessel dysfunction exacerbates atherosclerosis. 74 Conversely, is it possible to improve lymphatic function or promote IAL as a new method for the treatment of atherosclerotic diseases? Therefore, to better clarify these mechanisms, we need to establish models to avoid some of the caveats, one of which is the inflammation inherent in a surgical operation, which can promote IAL.
Conclusions
IAL is the most frequent phenomenon occurring under inflammatory conditions. IAL is not only closely related to inflammatory symptoms but also can influence the course of inflammation significantly. Atherosclerosis is a sign of chronic inflammation and a large number of immune cells gathered in the lesion. Immune cells in atherosclerosis can induce the expansion of the lymphatic vessels so that they can transport inflammatory cells to the LNs and produce specific immune responses, thereby reducing the local inflammatory response. In cholesterol transport, after the uptake of cholesterol, HDL can enter the lymphatic lumen through the receptor SR-B1 on the surface of the cell and then circulate with the blood and eventually transfer to the liver metabolism.
Increasing research has found that lymphatic vessels are closely associated with atherosclerosis. Perhaps in the near future the neglected lymphatic vessels will become an essential component in the treatment of atherosclerosis. However, the relationship between atherosclerosis and many aspects of lymphatic vessels remains unclear, requiring future studies to understand the mechanisms of IAL in atherosclerosis. Overall, the presence of lymphatic vessels and IAL appears to be beneficial in atherosclerotic conditions.53,75 Researchers and clinicians should be aware that treating this disease through the lymphatic system may be a double-edged sword and that the background and complexity of lymphatic biology must be fully taken into account.
Footnotes
Acknowledgments
The study was approved by the University of South China Medical Ethics Review Committee. The authors sincerely acknowledge the financial assistance provided by the National Natural Science Foundation of China (No. 81770490) and the Construct Program of the Key Discipline in Hunan Province (Basic Medicine Sciences in University of South China).
Author Disclosure Statement
No competing financial interests exist.