
Abstract
Background:
The L-Dex U400 is a recently developed measurement device to aid in the clinical assessment of unilateral lymphedema. Until now, little is known about variation in measurement results of the L-Dex U400. The aim of this study was to determine variation in measurement results in determining extracellular fluid of the arm with the L-Dex U400 under different measurement conditions on 2 days and to determine the reliability of these measurements in healthy subjects.
Methods and Results:
Thirty participants were included. Participants were measured on 2 days, 2 weeks apart. Each day they were measured six times, 1st basic measurement, 2nd after a 10-minute rest period, 3rd second observer, 4th after drinking 200 mL of coffee and rest for 30 minutes on the examination couch, 5th after 30 minutes of cycling on an exercise bike at 50 W and 50–60 rounds per minute, and 6th after a 10-minute rest period. The variance due to participants was 68% of the total variance and 32% was error variance. Lin's concordance coefficient (CCC), a reliability measure, ranged from 0.935 (first day, 1st and 2nd measurement of observer 1) to 0.517 (first and second day after a 10-minute rest period after cycling). In two CCCs, the lower limits of the 95% confidence interval were higher than 0.750. Repeatability coefficient was smallest for the basic observations on day 2 (4.6) and largest after cycling (8.0).
Conclusions:
Clinical decision-making based on L-Dex U400 measurements should be regarded with caution because of moderate reliability.
Introduction
Bioimpedance spectroscopy (BIS) is a noninvasive and relatively quick method to determine body composition. 1 BIS is also used to determine extracellular fluid (ECF) as a measure for unilateral lymphedema in the arm or leg.2,3 In mastectomy patients, BIS is used to assess lymphedema longitudinally. 4 In breast cancer patients suffering from lymphedema, effects of interventions to reduce lymphedema are evaluated using bioimpedance measurements. 5 For the detection of early lymphedema, BIS can be applied. 6
During BIS, an electric current with a frequency ranging from 3 to 1000 kHz passes through the body. 3 Current passes through ECF at low frequencies and does not go through the cell membrane. However, at high frequencies, the current passes through both intracellular fluid (ICF) and ECF. 7
The impedance measured is determined by the difference between resistance and reactance. 7 The resistance is the resistance of ECF for an electrical current. The reactance is the resistance of ICF for an electrical current. Resistance and reactance are measured at every frequency (3–1000 kHz) to calculate the amount of ECF. Generally, ECF is expressed as a ratio of affected and unaffected side. In healthy subjects, this ratio is on average for arms 1.00 (SD 0.03) and for legs 0.99 (SD 0.05). 2 However, for legs, this ratio ranged from 0.75 to 1.21 for men and from 0.62 to 1.14 for women. The technical measurement error is relatively small in bioimpedance measurements. 2
The L-Dex U400, a bioimpedance analyzer (ImpediMed, Ltd., Brisbane, Australia), is a recently developed measurement device to aid in the clinical assessment of unilateral lymphedema. The measurements with the L-Dex U400 are quick and easy to perform. The L-Dex U400 values range in healthy subjects between −10 and +10. L-Dex U400 values of −10 and beyond are commonly associated with procedural errors. Values greater than +10 indicate early signs of lymphedema. L-Dex U400 outcomes correlate well with outcomes of perometry values in lymphedema patients. 8 In the user manual of the L-Dex U 400, it is stated that participants should not drink before testing and that they should not perform sports shortly before the measurements since it might influence body fluid concentration. 9
Until now, the inter- and intraobserver reliability of the L-Dex U400 has been investigated scarcely.10,11 In addition, the differences in measurements between 2 measurement days and the influence of drinking coffee or physical activity are unknown. If reliability is unknown, changes in measurement results in people with lymphedema can be either interpreted as changes in ECF or as a lack of reliability of the L-Dex U400.
The aim of this study was to determine variation in measurement results in determining the ECF of the arm with the L-Dex U400 under different measurement conditions on 2 days and to determine reliability of these measurements in healthy subjects.
Materials and Methods
Participants
Between January 2014 and May 2014, potential participants were recruited at the Hanze University of Applied Sciences, Groningen, The Netherlands. They were informed about the study by means of a lecture and an e-mail in which they were asked to participate. Potential participants were also recruited at a local sports club (Korfball association in Beilen). If they were interested to participate, they mailed the researcher (C.Y.T.) and received additional information about the study. Inclusion criteria were being healthy, able to perform moderate physical activity, and being able to attend the 2 measurement days. Excluded were participants with heart, liver, or kidney disorders, pregnancy, or other known afflictions influencing the amount and content of ECF. Informed consent was obtained from all individual participants included in the study.
Measurement protocol
Participants were measured on 2 days, 2 weeks apart. Before the measurements, participants filled in the Par-Questionnaire, to screen for health problems. 12 In addition, they had to remove shoes, socks, watches, belts, and jewelry and were asked to lay supine on an examination couch.
Electrodes with hypoallergenic glue, ImpediMed dual tab, were placed according to the instruction manual. We performed a measurement on the dominant side, changed leads, and measured the nondominant side. The mean of these measurement results (the L-Dex) was used for further analyses.
Measurements were performed under different measurement conditions. The basic measurement was performed by J.B. a physical therapist with 5 years of experience with BIS. After a 10-minute rest, the second measurement was performed (J.B.) and the electrodes were removed. The second observer (C.Y.T.: a physical therapist with little experience with BIS), unaware of the previous electrode setting, placed a new set of electrodes and performed the third measurement.
Thereafter, the participant was invited to drink 200 mL of coffee and rest for 30 minutes on the examination couch, after which the fourth measurement was performed (J.B.). We arbitrarily chose coffee because it was readily available in the testing room. Thereafter, participants were asked to cycle for 30 minutes on an exercise bike at 50 W and 50–60 rounds per minute. Participants received their fifth measurement (J.B.) immediately after cycling and the sixth measurement after another 10-minute rest period (J.B.). The protocol on the second day was identical to that of the first day.
Measurement results were recorded in a data booklet. For each measurement, a separate page was used and after recording the outcome, the page was turned. The observers were not allowed to look at the results of previous measurements. After completion of 2 measurement days, participants received a gift voucher (€10).
We aimed to include 30 participants because variation in measurement results tends to stabilize with this number. The medical ethics committee approved this study on December 17, 2013 (METc 2013/245).
Measures
With the L-Dex U400, a ratio between the dominant and nondominant arm is determined. The ratio was determined by placing three dual-tab electrodes: one on each wrist and one electrode at the right ankle. The electrodes were placed with the green reference line, of the electrode, in line with the ulnar and radial styloïd process, with the longest section of the electrode pointing distally. At the ankle, the green reference line of the electrode was placed in line with the medial and lateral malleolus of the ankle, also with the longest section pointing distally.
Statistical analysis
Data were entered in a database and checked for correct data entry. In addition, data were checked for abnormal values for healthy subjects (less than −10 and >100). Values exceeding this range were labeled as invalid measurements.
To analyze the influence of different measurement conditions (observers, coffee drinking, physical activity, and measurement days) on measurement results, variance components were calculated. Besides the main effects of the measurement conditions, their two-way interaction effects were also calculated.
A restricted maximum likelihood method for estimating the variance components was used because of missing data due to invalid measurements. The sum of all variance components (main effects and interaction effects), minus the variance due to participants, was used as an estimate of the error variance. The contribution of the measurement conditions and their interactions to the error variance was expressed as a percentage.
In addition, to visually inspect the influence of measurement conditions on outcomes, a Bland and Altman plot was made on the X-axis, the mean value of all observations of the 2 days, and on the Y-axis, the difference between the 2 days.
Linn's concordance coefficient (CCC) was calculated as a measure for intra- and interobserver reliability for different observations of day 1 and 2 and test/retest reliability after drinking coffee and after rest. 13 To determine repeatability coefficient, a one-way ANOVA with subject as factor was performed. From the residual variance of the ANOVA, the repeatability coefficient was calculated (1.96 × √2 × √residual variance) for all observations, days, observers, and measurement conditions. Data analyses were performed in IBM SPSS version 22.2.
Results
Thirty healthy volunteers (16 women and 14 men) participated in this study (Table 1). The age ranged from 18 to 25 years with a mean of 22.1 ± 2.1. Most of the participants were right dominant. One participant was not able to attend the second measurement day, resulting in six missing measurements. In total, 17 invalid measurements (outside the range less than −10 and >100) were identified, 1 after rest, 3 after drinking coffee, 5 after cycling, and 8 after a 10-minute rest after cycling. An overview of the results of the different measurement conditions is given (Table 2).
Characteristics of Participants (n = 30)
Summary of the Results
The variance due to participants was 68.0% of the total variance, and thus, 32.0% of the total variance was error variance. Most important sources of error variance were participant × day interaction (33.4%) and condition × day interaction (6.0%). In total, 51% of the error could not be attributed to a certain condition (Table 3).
Variance Components of Measurement Conditions and Their Interactions
Negative variance components were set to 0.
Limits of agreement were −0.6 ± 2 × 3.7. One basic measurement, four measurements after rest, two after cycling, and two after a 10-minute rest period after cycling exceeded the limits of agreement (Fig. 1).
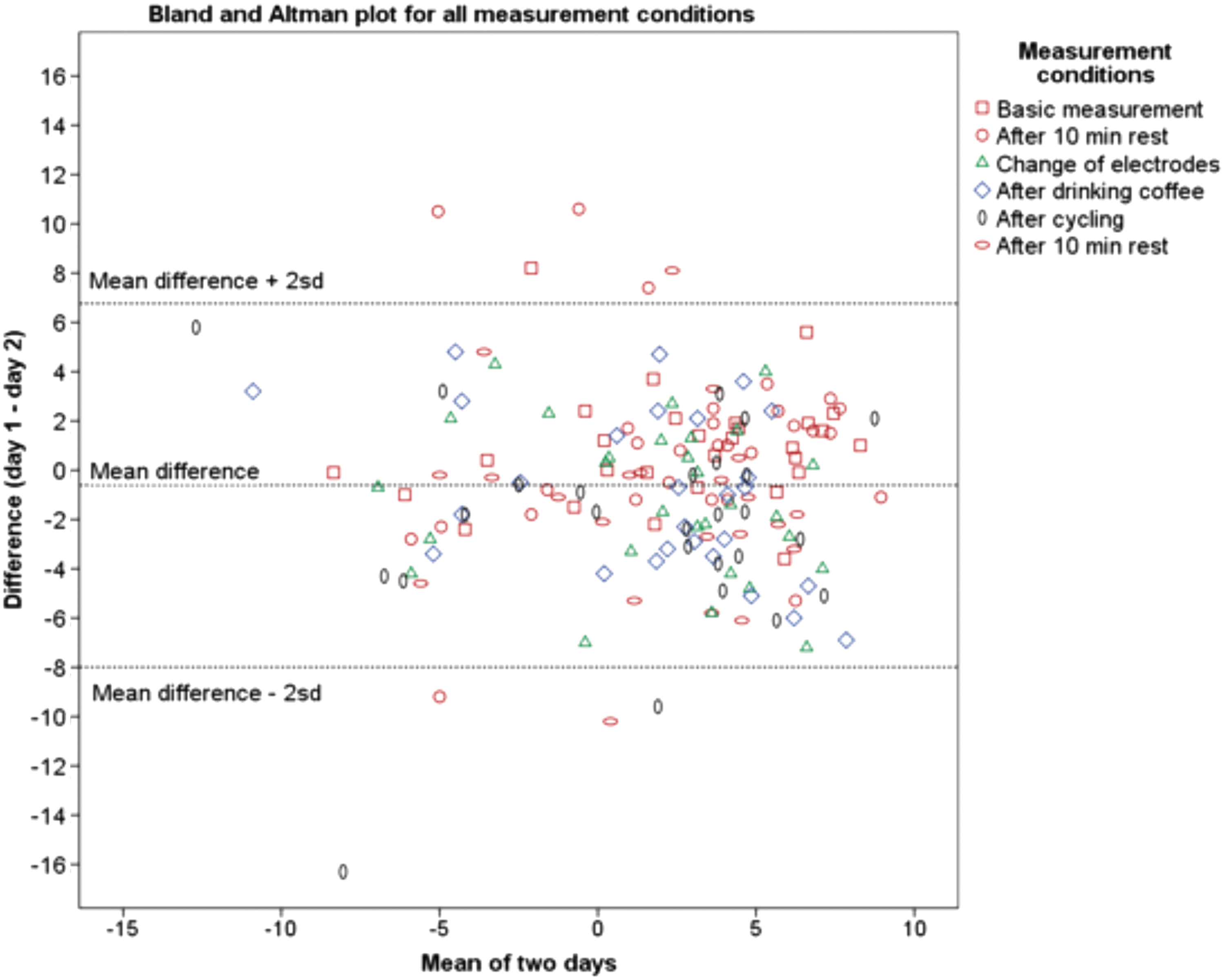
Bland and Altman plot for all measurement conditions. Limits of agreement were (mean ±2 SD) −0.6 ± 2 × 3.7. One basic measurement (red square), four measurements after 10-minute rest (red circle), two after cycling (black ellipse), and two after a 10-minute rest period after cycling (red ellipse) exceeded the limits of agreement.
Lin's CCC ranged from 0.935 (first day, first and second measurement of observer 1) to 0.517 (first day and second day after a 10-minute rest period after cycling). Four CCCs were larger than 0.75. For two CCCs, the lower border of the 95% confidence interval was higher than 0.75 (first day, first and second measurement of observer 1) and interobserver reliability at day 2 (Table 4).
Lin's Concordance Coefficient for Different Measurement Conditions
CCC, concordance coefficient; LB, lower border, Obs, observer; UB, upper border.
Repeatability coefficient was smallest for day 2 (4.6) and largest after cycling (8.0) (Table 5).
Repeatability Coefficients
Discussion
In this study, we found that 4 of the 10 CCCs were >0.75, a minimal requirement for reliability. 14 Only 2 out of 10 CCCs had a lower border of the 95% confidence interval above 0.75. The lowest CCC was calculated for measurements after a 10-minute rest period after cycling. Repeatability coefficients were large relative to the scale range of the L-Dex U400. The smallest repeatability coefficient was found for measurements on day 2. Clinically, this repeatability coefficient of 4.6 indicates that a measurement result on day 2 will fall within 4.6 points of the other measurements on day 2 in 95% of the measurements. No obvious clusters of measurement conditions can be seen, indicating that the variation in measurement results is not strongly related to the measurement condition (Fig. 1).
Our findings indicate that measurement results using the L-Dex U400 have a limited reliability in healthy subjects. The repeatability coefficient of 6.3 for all observations indicates that when one measurement is performed, the values of a second measurement will fall within 6.3 points of the first measurement in 95% of the measurements. The smallest repeatability coefficient between days was the basic measurement (4.8), indicating that clinical decisions based on L-Dex U400 should be regarded with caution, since changes in ECF assessed using the L-Dex U400 on day 1 and 2 in the first measurement can only be detected if the difference is 4.8 or larger. On a scale of −10 to 10, being the normal range of measurements, this value accounts for 24% of the scale range.
Effects of skin temperature and skin hydration on bioimpedance have been analyzed previously. 15 With an increase of skin temperature, from 20°C to 40°C, a considerable decrease in the resistance (35%) and reactance (18%) occurred. In addition, after emersion in a 30°C water bath for 10 minutes, resistance decreased with 20% and reactance with 25%. 15 We analyzed different measurement conditions, and as can be seen in Table 4, reliability was not considerably poorer after changing body position (coffee drinking, sitting on a chair).
However, reliability was poor after riding a bicycle and rest thereafter, which might be related to adhesion problems of the electrodes because 13 measurements after bicycle riding were invalid. In an earlier study, the effect of postural changes (supine, 70° head up tilt, and again 30 minutes supine) on the reliability of volume estimations using BIS was analyzed. 16 It was found that ECF and ICF significantly changed after postural changes and that a steady state could not be reached within 30 minutes after these posture changes. 16
To assess the efficacy of a single session of lymphatic massage in women with (n = 15) and without breast cancer-related lymphedema (n = 15), BIS and perometry were performed. 5 The authors concluded that massage was not effective since no significant change (neither in BIS nor in perometry) was found after a single session of massage. However, the authors failed to consider the possibility that the measurement instruments were not precise/reliable enough. 5
For reliability of BIS, they referred to the study of Czerniec et al. who assessed BIS (SFB7; ImpediMed Ltd.). 17 Intraclass correlation between sessions was 0.95 for the women with lymphedema and 0.81 for women without lymphedema. 17 High ICCs do not guarantee a small repeatability coefficient. Under strictly standardized measurement conditions (Bioelectrical Impedance Analyzer [BIA] 2000-M; Data Input Comp, Frankfurt, Germany) was found to be a highly reliable tool (small technical errors) at all frequencies.
Variations in outcomes were influenced by age, gender, and body mass of the study population. 18 Strong correlations between BIS and perometry have been reported ranging from 0.80, for ICF, to 0.90, for ECF. However, the data show a considerable underestimation of ICF as well as ECF of BIS relative to the estimate volumes based on perometry. This finding was expected by the authors of that article since the methods do not measure the same quantity, fluid volume, and total volume. 3
In another study, agreement between BIS and perometry was analyzed in 45 participants with and 21 without lymphedema of the arm. 19 Limits of agreement ranged in that study from −15.3 to 14.6. BIS misclassified 12 participants (27%) with arm lymphedema as having no lymphedema. 19 The difference between the methods increased with an increase of arm volume. 19
In a study evaluating swelling after total knee arthroplasty, intraobserver reliability and interobserver reliability expressed (using the SFB7; ImpediMed, Ltd.) as an ICC ranged from 0.90 to 0.99 and from 0.89 to 0.99, respectively. 11 For the detection of breast cancer-related lymphedema (using the XCA®; Impedimed, Ltd.), three groups were measured three times with a 5-minute interval. The ICC for agreement between measurements ranged from 0.99 for healthy women and women at risk for lymphedema to 0.69 for women with lymphedema. 10
Chronic lymphedema consisting of fibroses and fat cannot be measured with BIS. 20 Therefore, BIS is only useful in the early stages of lymphedema. Some patients in previously mentioned studies may have had progressed lymphedema influencing reliability negatively. To determine the validity of multifrequency (MF) and single-frequency BIA, outcomes of these measurement procedures were compared with those of Dexa. MF-BIA (MF-BIA) values had a better explained variance with Dexa values (r 2 = 0.92 for fat mass and r2 = 0.87 for fat-free mass) than single-frequency BIA (r 2 = 0.89 for fat mass and r2 = 0.76 for fat-free mass). However, changes in body composition assessed by means of Dexa and MF-BIA had a moderate explained variance (r 2 = 0.39 for fat mass and r2 = 0.32 for fat-free mass). 21
A limitation of the present study was the lack of experience of observer 2 with
In this study, we did not change electrodes after each measurement condition, which may be the reason why 17 invalid observations were found. Probably the electrodes became loosened during cycling and the conduction properties (measurement properties) of the electrodes changed. In the user manual, it is advised not to leave the electrodes attached to the skin for over 1 hour. In this study, all measurements were performed within an hour.
We studied healthy subjects only, which might have influenced reliability results. In a previous study, conflicting results have been reported regarding differences in reliability between patients with lymphedema and healthy subjects. 10 ICCs differed between healthy subjects, patients with lymphedema, and patients at risk for lymphedema, ICCs were 0.99, 0.99, and 0.69, respectively. 10 In another study, intraobserver reliability was larger for lymphedema patients (0.96) than for controls (0.21) when determining interlimb R0 ratio using BIS. For the affected arm R0 using BIS, the ICCs were 0.95 for lymphedema patients and 0.81 for controls. 17
In addition, in the user manual, it is stated that a full bladder and the menstrual cycle may influence measurement results. In our research, we did not ask women if they were menstruating or not, and we did not ask participants to go to the toilet before measuring. However, looking at the effects of coffee drinking, which induces filling of the bladder after some time, the repeatability coefficient was 6.7, not extremely different from the other repeatability coefficients. Measurement condition and interactions were responsible for 32% of the error variance, while 51% of the error variance could not be linked to any specific source. This finding indicates that reducing error variance is not easy.
For future research, it is important to be more specific before starting the measurement, such as go to the toilet and ask women if they were menstruating. More research with the L-Dex U400 in patients with lymphedema is needed to determine its clinical relevance of ECF levels.
Conclusion
We found that reliability was good for 4 of the 10 reliability indices and that measurement conditions influence measurement results of the L-Dex U400 considerably.
Footnotes
Acknowledgment
The authors thank C. Kingsford of ImpediMed, Inc., Brisbane, Australia, for providing them with the electrodes used in this study.
Ethical Approval
“All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.” The medical ethics committee approved this study on December 17, 2013 (METc 2013/245).
Author Disclosure Statement
ImpediMed, Inc., Brisbane, Australia, provided us with electrodes for free. No other competing financial interests exist.