
Abstract
Abstract
Background:
In patients with arm or leg lymphedema, more fat has been found in the epifascial compartment of the edematous limb compared to the healthy limb. However, not much is known about subfascial fat accumulation in these patients. This study aims to investigate the intramuscular and intermuscular fat and muscle/water volume in lymphedema patients. The excess of intramuscular and intermuscular fat volume was also compared to the excess epifascial fat volume, the excess limb volume, and the duration of lymphedema.
Methods and Results:
Data from 13 patients (seven arm and six leg lymphedemas) were acquired using a 1.5 T magnetic resonance imaging (MRI) scanner before liposuction and at five time points (4 days, 4 weeks, 3 months, 6 months, and 1 year) after liposuction. From water-fat imaging, fat and muscle/water volumes within the intramuscular and intermuscular compartments were calculated. The relative excess volume was defined as (volume of edematous limb–volume of healthy limb)/volume of healthy limb. Elevated relative excess volumes of intramuscular and intermuscular fat were found at all time points. A decrease in the relative excess volume of muscle/water over time was found. This decrease was not correlated to the relative excess of epifascial fat volume, the relative excess of limb volume, or the duration of lymphedema.
Conclusions:
An excess fat volume was found in the intramuscular and intermuscular compartments in lymphedema patients. The results suggest that the subfascial compartment needs to be studied separately as no correlation between intramuscular/intermuscular fat accumulation and other measured parameters was found.
Introduction
L
The lymphatic system can be divided into two compartments: a superficial and a deep lymphatic system. The deep lymph vessels follow the deep veins embedded between the muscles in the subfascial compartment, whereas the superficial lymph vessels mostly follow the epifascial veins. 7 Studies of lymphedema associated with adipose tissue have mainly focused on the accumulated excess epifascial fat,5,6 even though the superficial and deep lymph vessels connect to the same lymph nodes. However, a recent study showed that not only the epifascial but also the subfascial fat volume was higher in the edematous limb compared to the healthy limb. 8 It is therefore not unlikely that in the case of inadequate lymph drainage, the deep lymph vessels might have a similar effect on the subfascial compartment as the superficial lymph vessels have on the epifascial compartment.
Not much is known about the effects of lymphedema on the subfascial compartment. However, it has been shown that accumulation of intramuscular and intermuscular fat is related to insulin resistance and diabetes type 2,9–12 inflammation,13,14 and chronic pain, 15 as well as reduced muscle function. 16 Therefore, it is of interest to further study the possible subfascial fat deposition in patients with lymphedema.
Common methods for diagnosing lymphedema include clinical examinations such as the pitting test and test for Stemmer's sign. 3 The excess volume can be calculated by the use of plethysmography or by measuring the circumference along the limb using the formula of the truncated cone. 17 However, these methods are not appropriate for studying how lymphedema affects the subfascial compartment as an accumulation of subfascial fat and fluid has little effect on the total excess limb volume. 18 Alternative methods for diagnosing and studying lymphedema are dual-energy X-ray absorptiometry, 6 lymphoscintigraphy, 19 computed tomography, 20 and magnetic resonance imaging (MRI).8,18,21 MRI can offer additional information about the edema due to the possibility of obtaining 2D and 3D images, as well as enabling more advanced data processing to separate water and fat.
An established imaging method for separating fat and water is the water-fat MRI. Although previously it has mainly been used to quantify fat in the liver22,23 and skeletal muscle,24,25 it was used in a recent study to investigate the fat accumulation in lymphedema patients. 8 Using this method, assessments of how both the epifascial and subfascial compartments are affected by lymphedema, the spatial distributions of fat and fluids over the whole limb, and quantitative measurements of the fat and fluid volumes8,18 are possible. This may provide a greater understanding of the underlying pathophysiology of lymphedema and how it affects patients.
The aim of this study is to quantify and examine the excess adipose tissue in the subfascial compartment in arm and leg lymphedema. Specifically, intramuscular and intermuscular fat and water accumulation will be explored using water-fat MRI. Furthermore, the change in accumulated fat and water from before and up to 1 year after liposuction is investigated and the relationships between the accumulated intramuscular and intermuscular fat, epifascial fat, and plethysmography measurements are evaluated.
Materials and Methods
Patients
Seven patients with arm lymphedema and six patients with leg lymphedema were recruited. The patient group consisted of patients with primary or secondary lymphedemas. The median duration (interquartile range) of lymphedema was 6.0 (3.5 to 8.5) and 9.0 years (4.5 to 14) for arms and legs, respectively. Breast cancer treatment was the cause of the lymphedema in the six patients with arm lymphedema. As for the leg lymphedema patients, three had been treated for cancer (two with uterus cancer and one with synovial sarcoma in the groin) and three had primary lymphedema (one male and two females). All patients had been treated conservatively before liposuction and were wearing compression garments daily. Thus, no or minimal pitting was found when performing the pitting test. 3
Ethics
The Regional Ethical Review Board in Lund approved the study. All patients signed a written informed consent to participate and could withdraw from participation at any time. The procedures followed were in accordance with the Declaration of Helsinki of 1964 and its most recent revision of 2013, and followed the Guideline for Good Clinical Practice E6(R2) (ICH Harmonised Guidelines, 2016).
Data acquisition
Water plethysmography was performed to measure the excess volume, that is the difference in volume between the edematous and healthy limb before the liposuction (baseline). The limbs were also examined with water-fat MRI before liposuction and at five time points (4 days, 4 weeks, 3 months, 6 months, and 1 year) after liposuction. Three patients could not be measured at 6 months due to technical problems and one patient was not examined at 1 year due to recurrence of breast cancer.
All MRI images were acquired using a 1.5 T MRI scanner (MAGNETOM Sonata, Siemens Healthcare) using a small flex coil for the arms and a large flex coil for the legs. Three slices were acquired using a multi-echo gradient echo sequence at eight echo times with the following acquisition parameters: first echo time = 1.83 ms, interecho time = 2.47 ms, flip angle = 10, repetition time = 600 ms, field of view = 400 × 200 mm2, voxel size = 1.6 × 1.6 × 5 mm3, number of averages = 4, and bandwidth = 815 Hz/pixel. The images were centered 10 cm distally of the humeral epicondyle or 16 cm distally of the femoral epicondyle for the arms and legs, respectively.
Data analysis
All MRI data was processed and statistical analysis was conducted using MATLAB (r2013/r2017; The MathWorks, Inc.).
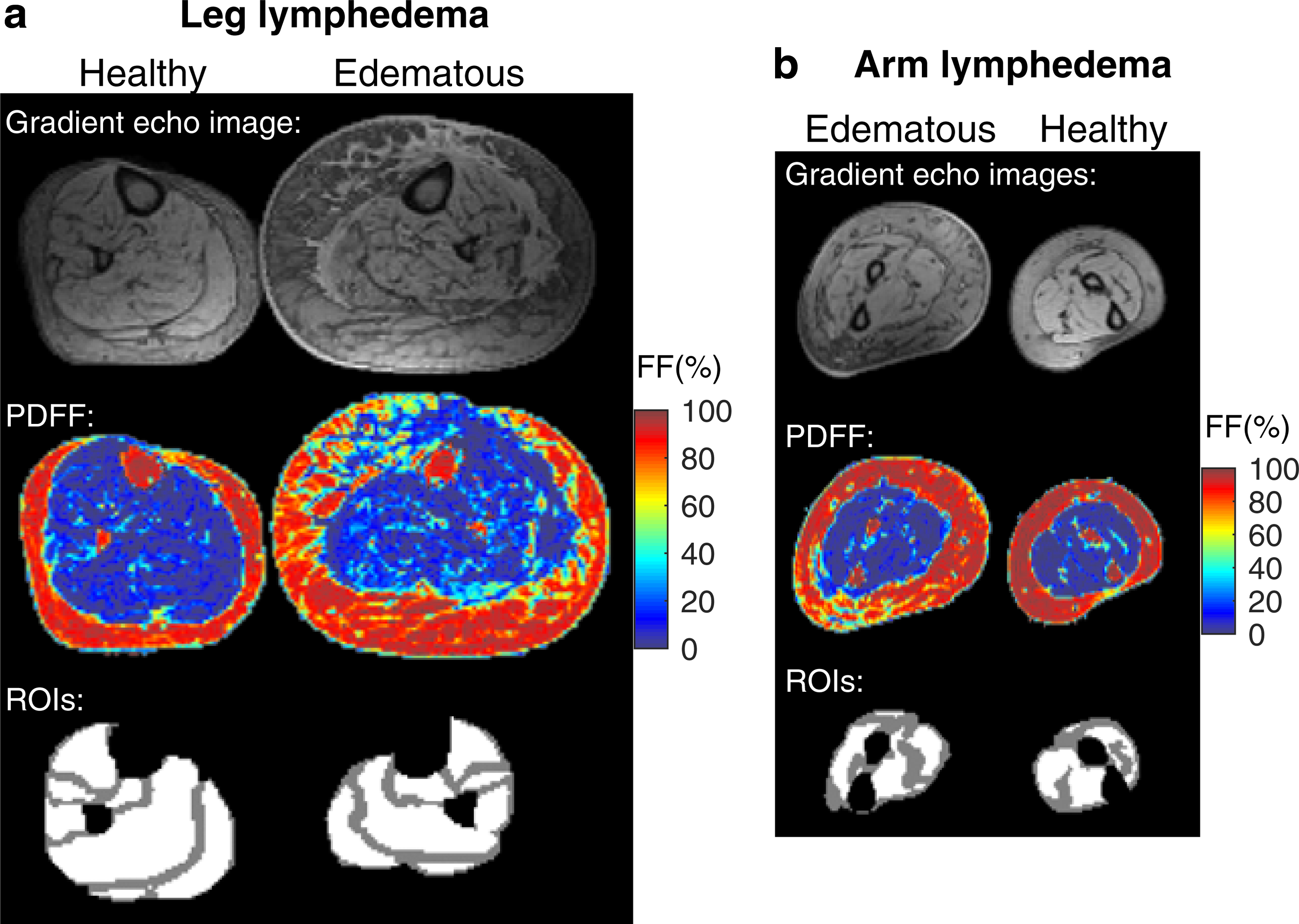
Using an MRI water-fat separation method, 26 separate images of water and fat were calculated from which the proton density fat fraction (PDFF) was calculated as fat signal/(water signal + fat signal) and the water fraction as water signal/(water signal + fat signal). On the original gradient echo images, regions of interest (ROIs) were drawn to separate the epifascial from the subfascial compartments, and to separate the intramuscular from the intermuscular regions of the subfascial compartment. In the legs, the latter was achieved by delineating seven muscle groups: the soleus, tibialis anterior, tibialis posterior, gastrocnemius medialis, gastrocnemius lateralis, peroneus longus, and extensor digitorum longus. In the arms, only two intramuscular compartments were outlined, each containing several muscle groups, as the spatial resolution of the MRI images was too low for more detailed outlining. The voxels within the ROIs were defined as intramuscular, whereas the remaining voxels within the subfascial compartment, excluding the bones, were categorized as belonging to the intermuscular ROI. By using only two ROIs to define the intramuscular compartment of the arms, intermuscular space was inevitably included in the intramuscular ROIs. To minimize this bias as much as possible, visible fat streaks within the intramuscular ROI, which were predicted to be intermuscular fat, were recategorized as intermuscular ROI. All ROIs, in the arms and legs, were manually drawn 1–2 pixels inside the margin. As a result of this margin, some intramuscular voxels were included in the intermuscular compartment since the intermuscular ROI is defined by the voxels outside of the drawn ROIs.
For both healthy and edematous limbs, the fat volumes of the epifascial, intermuscular, and intramuscular compartments were calculated as the sum of all voxel PDFFs within the corresponding ROI multiplied by the voxel volume. The relative excess volume of fat between healthy and edematous limbs was then calculated as (fat edematous limb–fat healthy limb)/fat healthy limb. Correspondingly, the water volume within the intramuscular compartment was calculated by taking the sum of the water fractions over all voxels multiplied with the voxel volume.
Statistical analysis
In all the data analysis and statistical tests, arm and leg lymphedemas were treated as one joint group. Using a Wilcoxon signed-rank test, the relative differences in fat volume, water volume, and PDFF were tested against zero (no difference between the healthy and edematous limbs). Wilcoxon signed-rank tests were also performed to test if the fat volume difference between healthy and edematous limbs changed over time. The relative excess of water/muscle volume was calculated and statistically tested in the same manner as described above. Since the parameters were not normally distributed, median and interquartile ranges were used. The outcome of these tests was considered to show exploratory results, and therefore nominal p-values are presented without any adjustment for multiple comparisons. For all tests, p < 0.05 was considered a significant result.
Spearman's ranked correlation test was used to investigate whether the excess intramuscular and intermuscular fat volumes correlated with each other, or with the excess epifascial volume, the excess total limb volume measured by plethysmography, and the duration of lymphedema, respectively.
Results
The median (interquartile range) excess volumes measured with plethysmography were 1345 mL (865 to 1548) and 3733 mL (2920 to 5618) in the arms and legs, respectively. The median duration of all lymphedemas, both arms and legs, was 6 years (3.75 to 10.5).
The multiecho gradient echo images, the resulting PDFF map using water/fat separation, and muscle ROIs of a typical leg and arm patient are depicted in Figure 1. In the PDFF maps, an overall elevated PDFF can be seen in the subfascial compartment of the edematous limbs compared to the healthy limbs, especially in the legs.
In Figure 2a, the relative excess volume of intramuscular fat between edematous and normal limbs is shown. At four time points (4 days, 4 weeks, 3 months, and 6 months postliposuction), a significant difference (p = 0.0034/0.011/0.040/0.037) in the relative excess volume of intramuscular fat was found between the edematous and healthy limbs. No significant difference between baseline and the postliposuction time points could be found. The corresponding difference for intermuscular fat is shown in Figure 2b. All time points show significant differences (p = 0.0005/0.027/0.0012/0.013/0.0020/0.0093) between edematous and healthy limb fat volume, whereas only two time points, 4 days and 4 weeks postliposuction, differ significantly from baseline (p = 0.0034/0.022).
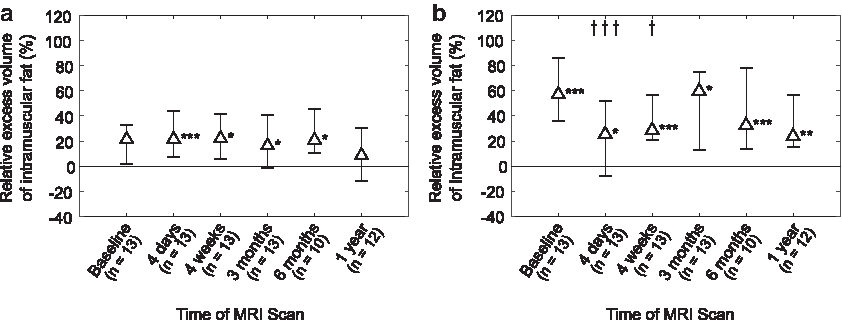
Relative excess volume of fat in
The relative excess volume of intramuscular muscle/water of the limbs is shown in Figure 3. A decrease over time in muscle/water volume can be seen where the three last time points (3 months, 6 months, and 1 year after treatment) are significantly different from baseline (p = 0.027/0.027/0.0027). No significant difference between the edematous and healthy limbs is found at any time point, although a declining trend can be seen.

Relative excess volume of muscle/water in the intramuscular compartment between edematous and normal limbs. The marker represents the median value and the error bars mark the first and third quartiles. Significant differences from baseline are marked with daggers (†). (†p < 0.05).
A significant difference in PDFF between the edematous and healthy limbs was found at all time points postliposuction (p = 0.006/0.013/0.005/0.037/0.034), as depicted in Figure 4. In contrast, no significant difference between baseline and other time points was found.
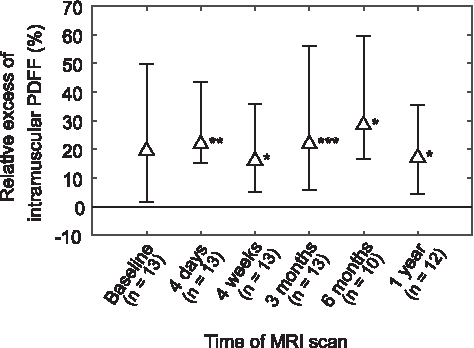
Relative excess of PDFF in intramuscular fat between the edematous and normal limb. The marker represents the median value and the error bars mark the first and third quartiles. Significant differences between the healthy and edematous limbs are marked with asterisks (*). (*p < 0.05, **p < 0.01, ***p < 0.001).
The relationship between the relative excess volumes of intermuscular and intramuscular fat at baseline is presented in Figure 5. The Spearman's ranked correlation coefficient was calculated to be 0.40 (p = 0.18) and indicates that there was no correlation between the accumulated excess fat in the intermuscular and intramuscular compartments.
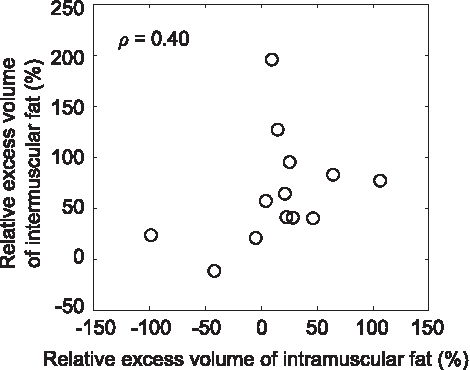
Spearman's correlation between the relative excess of intermuscular and intramuscular fat volumes between the healthy and edematous limbs. The Spearman's correlation is 0.40 (p = 0.18).
Comparisons of the relative excess of intramuscular and intermuscular fat, respectively, with the relative excess volume of epifascial fat, the relative excess of total limb volume measured with plethysmography, and the duration of lymphedema, are shown in Figure 6. All comparisons were performed at baseline. No correlation could be found in any comparison. The Spearman's coefficients were 0.19 (p = 0.53) and −0.15 (p = 0.63) for the comparison of the relative excess volume of epifascial fat with the relative excess volumes of intramuscular and intermuscular fat, respectively. The corresponding Spearman's coefficients for the relative excess of total limb volume and the duration of the lymphedema were 0.55 (p = 0.052) and 0.13 (p = 0.63), and 0.09 (p = 0.76) and 0.01 (p = 0.97), respectively.

Spearman's correlation between the relative excess intramuscular and intermuscular fat, respectively, and the relative excess of epifascial fat volume
Discussion
In this study, the subfascial compartment of patients with lymphedema was investigated. Generally, an increased fat accumulation in both the intramuscular and intermuscular regions of the subfascial compartment could be seen at all time points, whereas the muscle/water volume decreased over time. No significant correlations between the excess accumulation of fat in the intramuscular and intermuscular compartments and the excess epifascial fat accumulation, total limb volume, or the duration of the lymphedema were found.
Liposuction aims to remove excess fat in the epifascial compartment, thus leaving the subfascial compartment undisturbed. This probably explains why excess intramuscular and intermuscular fat were found at almost all time points after baseline, compared to the obvious effect on the epifascial compartment where the fat volume of the edematous limbs decreased below that of the normal limbs. 8
A decrease in water/muscle volume in the subfascial compartment was shown in a previous study using the same patient data as in this study. 8 It was suggested that the decrease in water volume originated from a decline in muscle mass due to a reduced mechanical load after liposuction. However, no differentiation was made between the intermuscular and intermuscular compartments. This study showed a decrease of muscle/water volume in the intramuscular compartment, which supports the hypothesis that there is a decrease in intramuscular muscle/water volume due to the reduced mechanical weight after liposuction of the edematous limb.
The fact that the water volume and the intramuscular fat volume decreased somewhat over time, after 3 months and after 1 year, respectively, while the intramuscular PDFF remained relatively constant throughout the follow-up, suggests that the small reduction in intramuscular fat volume was due to an overall reduction of total muscle mass rather than a pure loss of fat, which would result in a decrease in PDFF as well.
No correlation between the intramuscular and intermuscular fat accumulation was found. This suggests that lymphedema might not affect the intramuscular and intermuscular compartments equally. However, there is a possible source of bias due to the incorrect categorization of some intramuscular and intermuscular voxels when drawing the ROIs.
No correlation was found between the relative excess of accumulated fat in the epifascial compartment and the intramuscular and intermuscular compartments, respectively. In the same manner, the relative excess of total limb volume measured with plethysmography did not correlate with the intramuscular and intermuscular fat volume. This can be explained by the fact that the accumulation of subfascial fat might be limited due to the physical constraint of the fascia, whereas the epifascial compartment is only limited by the more elastic skin. In other words, measurements of the epifascial fat accumulation or limb volume only might not be enough and further studies of the intramuscular and intermuscular compartments are needed to fully understand how lymphedema affects the limbs.
No correlation between the duration of the patients' lymphedema and the relative excess volumes of intramuscular or intermuscular fat could be found. This corresponds well with a previous study where no correlation between the excess fat volume in the epifascial compartment (measured by DXA and plethysmography) and duration was found in the arms of patients with breast cancer-related lymphedema. 6
Although the MRI water/fat quantification method used in this study is commonly used,22–24,27 it is limited in this application as the method cannot separate free water (e.g., edema) from muscle tissue. This means that excess fluids accumulated within a muscle cannot be identified and therefore, it might be difficult to optimally evaluate muscle tissue changes. Other MRI methods, mainly based on T1- and T2-weighted as well as two-point Dixon images, have been used to study patients with lymphedema.18,21 However, these methods have primarily been proposed as segmentation methods to separate bone, muscle, and epifascial fat and fluid.
During this study, some limitations were identified. The study population was small and statistical analysis was performed without differentiating between arms and legs. The spatial resolution of the MR images was too low to easily separate the intramuscular fat from the intermuscular fat, especially in the arms, introducing a possible bias to the results as intramuscular fat is overestimated due to the inclusion of intermuscular fat. This was only partly compensated by the recategorization of intramuscular fat to intermuscular fat in areas with visible intermuscular fat streaks. Another source of bias arises from the ROI margin of 1–2 pixels, which was used when drawing the intramuscular ROIs. This allowed some of the intramuscular pixels to be included in the intermuscular ROI. As a result, the intramuscular fat is underestimated, and consequently the intermuscular fat is overestimated.
Conclusion
This study shows that the previously reported excess subfascial fat is present both in the intermuscular and intramuscular compartments. Both the excess intermuscular and intramuscular fat were fairly constant during the whole 12-month follow-up of this study. The relative excess volume of intramuscular muscle/water decreased over time, which may reflect a decreased load on the extremities due to the liposuction and concomitant reduction in muscle volume. Although it is too early to postulate any metabolic consequences, this article describes a phenomenon of increased intramuscular and intermuscular fat in patients with lymphedema, which has not been described previously. The study also shows that the intramuscular and intermuscular compartments need to be studied separately as no correlations with measurements using plethysmography or fat accumulation within the epifascial compartment were found. Further research with water-fat MRI is needed as it may provide an alternative for studying the detailed pathophysiological consequences of lymphedema in both the epifascial and subfascial compartments.
Footnotes
Acknowledgment
The project was supported by the Swedish Cancer Society, Stockholm, and Skåne County Council's Research.
Author Disclosure Statement
No competing financial interests exist.